Article Text

Abstract
Context The 2011 American Heart Association guidelines identified pregnancy complications as a risk factor for cardiovascular disease in women. However, miscarriage was not mentioned within the guidelines, and there is no consensus on the association between miscarriage and future risk of cardiovascular disease.
Objective To confirm or refute the association, a meta-analysis of published papers was conducted.
Data sources PubMed, Web of Knowledge and Scopus were systematically searched to identify appropriate articles. Reference lists were then hand searched for additional relevant titles.
Study Selection To be included, articles had to assess the association between miscarriage and subsequent cardiovascular disease in otherwise healthy women. Only women who had miscarriages were considered exposed. Pooled association measures, using random effects meta-analysis, were calculated for coronary heart disease and cerebrovascular disease. Publication bias and between-study heterogeneity were evaluated.
Data Extraction Two authors individually reviewed all studies and extracted data on patient and study characteristics along with cardiovascular outcomes.
Results 10 studies were identified, with 517 504 individuals included in the coronary heart disease meta-analysis and 134 461 individuals in the cerebrovascular disease analysis. A history of miscarriage was associated with a greater odds of developing coronary heart disease, OR (95% CI) =1.45 (1.18 to 1.78), but not with cerebrovascular disease, OR=1.11 (0.72 to 1.69). There was a strong association between recurrent miscarriage and coronary heart disease OR=1.99 (1.13 to 3.50). Evidence was found for moderate between-study heterogeneity and publication bias in the coronary heart disease analysis.
Conclusions The meta-analysis indicates that a history of miscarriage or recurrent miscarriage is associated with a greater risk of subsequent coronary heart disease.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Coronary heart disease (CHD) is the leading cause of death in women in every major developed country and most emerging economies.1 Effective interventions exist to reduce the risk of CHD in women and men who are at high risk. Hence, better approaches for identifying individuals at increased risk of CHD could lead to the more effective targeting of preventative treatments.
A large body of work mostly published in the last 10 years has shown that women who experience complications of late pregnancy are at risk of CHD in later life. The resulting concept that the unique cardiovascular stress that occurs during pregnancy can improve risk prediction was recently acknowledged in the 2011 American Heart Association guidelines, which incorporated obstetric complications in the classification of cardiovascular disease (CVD) risk in women.2 The cardiovascular impact of a range of obstetric complications was discussed, including pre-eclampsia,3–5 preterm birth4 ,6 ,7 and gestational diabetes.8 ,9 However, the long-term cardiovascular implications of miscarriages were not considered.
Miscarriages are the most common complication of pregnancy, with 12%–24% of all clinically recognised pregnancies ending in miscarriage;10 ,11 and approximately a third of all pregnancies, including those not brought to clinical attention, lost through miscarriage.11 ,12 Although there is no standard international definition for the gestational boundaries of a miscarriage, the majority of miscarriages occur during the first 12 weeks of gestation.13
There are a range of joint risk factors for CVD and miscarriage, including obesity,14 smoking and alcohol intake.12 Subsequent to controlling for these confounders, evidence has arisen for an association between a miscarriage and CVD, with a dose–response relationship found in some studies.15 The aim of the present study was to determine the association between miscarriage and future CVD in women through a meta-analysis of two distinct outcomes: CHD, using 517 504 individuals with 1685 cases, and cerebrovascular disease, using 134 461 individuals with 663 cases.
Methods
Study selection
The databases of the US National Institutes of Health (PubMed), Scopus and Web of Knowledge were systematically searched for relevant articles between November and December 2011. No restrictions were applied to the publication period of the articles. Both medical search headings and open text fields were used to identify articles. The search terms for the exposure were: ‘Spontaneous Abortion’, ‘Habitual Abortion’, ‘Recurrent Abortion’, ‘Recurrent Miscarriage’, ‘Habitual Miscarriage’, ‘Miscarriage’, ‘Foetal Death’, ‘Fetal Death’ and ‘Pregnancy Loss’ and search terms for the outcome were: ‘Cardiovascular Disease’, ‘Coronary Artery Disease’, ‘Myocardial Infarction’, ‘Heart Attack’, ‘Coronary Heart Disease’, ‘Ischemic Heart Disease’, ‘Ischaemic Heart Disease’, ‘Stroke’, ‘Transient Ischemic Attack’, ‘Transient Ischaemic Attack’, ‘Vascular Accident’ and ‘Apoplexy’. The search in PubMed was restricted to articles relating to humans. Once relevant articles were identified their references lists were searched for additional articles.
To be included in the meta-analysis, articles had to assess the association between miscarriage and subsequent CVD in otherwise healthy women. Papers only evaluating therapeutic abortions, stillbirths, neonatal deaths or ectopic pregnancies were excluded in order to minimise heterogeneity in the exposure. Two different exposures were evaluated: a history of miscarriage, where one or more miscarriages was considered exposed; and recurrent miscarriage, where exposure was defined as either two or more, or three or more miscarriages, depending on the data provided in the study. Both exposures were compared with no miscarriages.
Where studies did not provide the necessary association measures, the raw data provided within the papers were used to calculate an unadjusted estimate.
All cardiovascular outcomes were of interest, including CHD, angina, non-fatal and fatal myocardial infarction, ischaemic and haemorrhagic stroke, and transient ischaemic attacks (TIA). Outcomes were segregated into two groups: CHD, which comprised any diagnoses of CHD, as well as individuals who had undergone Coronary Artery Bypass Graft; and cerebrovascular disease, where outcomes of interest were ischaemic and haemorrhagic stroke and TIA.
Finally, only cohort or case-control studies were included, as an association measure was required. The decision to include studies was hierarchical; initially study titles, then abstracts and finally the fully body of the text were assessed.
As some articles assessed the same association using data from the same individuals, the article containing the greater number of participants or, where the same number of participants was used, the article with more detailed analytic information was selected.
Data extraction
The literature search and data extraction were conducted by two investigators (CTO-W and EEH). A predesigned data abstraction form was used by both reviewers to collect information from articles. The data collected included lead author, year of publication, study design, population studied, exposure and outcome evaluated, number of cases, number of non-cases, the association measure, point estimate and 95% CI, and any adjustment/stratification/matching variables. Any differences between reviewers were discussed and resolved by a third individual (AMW).
Bias within each individual study was evaluated using the validated Newcastle–Ottawa Scale, a semiquantitative scale designed to evaluate the quality of non-randomised studies.16 It allocates a maximum of nine stars to a study. Study quality was judged on the selection criteria of participants, comparability of cases and controls, and exposure or outcome assessment.
Statistical analysis
In studies where no appropriate association measure was provided, if possible, the raw aggregated data (ignoring matching designs, where necessary) were used to estimate unadjusted associations. The inverse variance weighted method was used to combine ORs, rate ratios and HRs to produce a pooled OR, under the rare outcome assumption. Random effects models were used for all analyses to allow for between-study heterogeneity. Heterogeneity was assessed using the Cochrane χ2 statistic and the I2 statistic. Sensitivity analyses were conducted to evaluate the effect of different levels of adjustment and the potential impact of bias in individual studies. Publication bias was evaluated through a funnel plot and Egger's test. All tests were two-tailed and p values of 0.05 or less were considered significant. STATA release 10 (V.10.0, STATA, College Station, Texas, USA) was used for all statistical analyses.
Results
Descriptive analysis
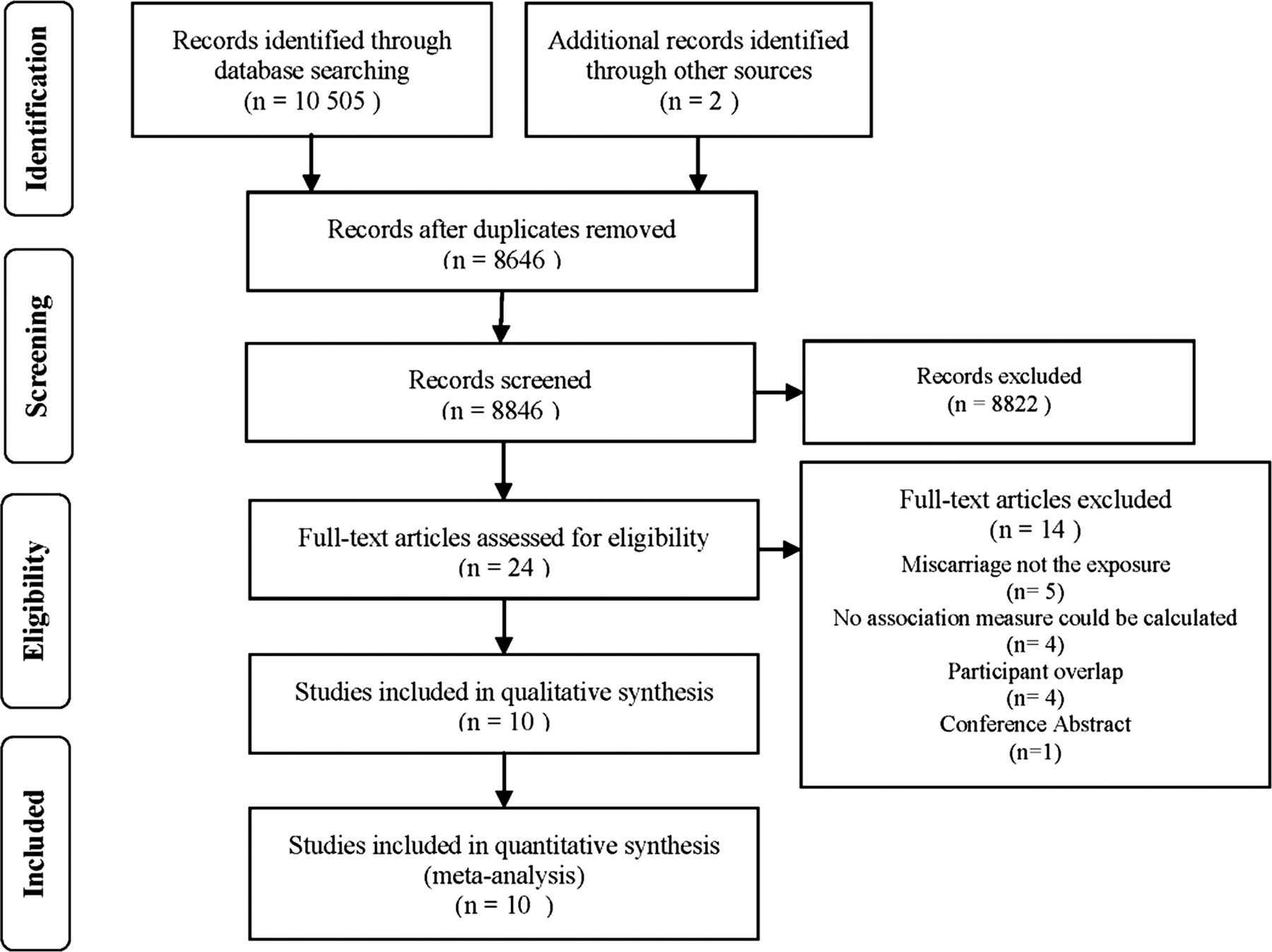
Figure 1 shows the flow diagram of the search results. All studies were based in either Europe or North America. Five cohort studies and five case-control studies were found, two of which used hospital-based controls. Ten studies evaluated the association between miscarriage and CHD; this included 517 504 women, 1685 of whom were cases (table 1). Three of these studies also analysed stroke outcomes; a fourth study with combined stroke and TIA outcomes was also identified, resulting in 374 598 women, with 2542 stroke and TIA cases (table 2).
Studies that evaluated the association between miscarriage and CHD
Studies that evaluated the association between miscarriage and cerebrovascular disease

Flow diagram of study exclusion and inclusion.
Nine studies reported associations with a history of miscarriage of which five made minimal or no adjustment for confounders. Seven studies reported an association between recurrent miscarriage and CHD, four of which made minimal or no adjustment for confounders. One study used a combined exposure, including both spontaneous and therapeutic abortions.17
As association measures were not provided in the papers by Winkelstein and colleagues,26 ,27 they were calculated from the raw data available in the paper; however, the matched nature of the data was ignored as a result.
The quality of included studies, as assessed using the Newcastle–Ottawa quality assessment scales, scored moderately high in exposure and outcome assessment and selection of participants; however, a number of studies did not adjust for more than one confounder or the raw data were used, precluding any adjustment, and consequently the case-control studies did not score well on the comparability section (table 3).
Assessment of study quality through the Newcastle–Ottawa Scale
Meta-analysis
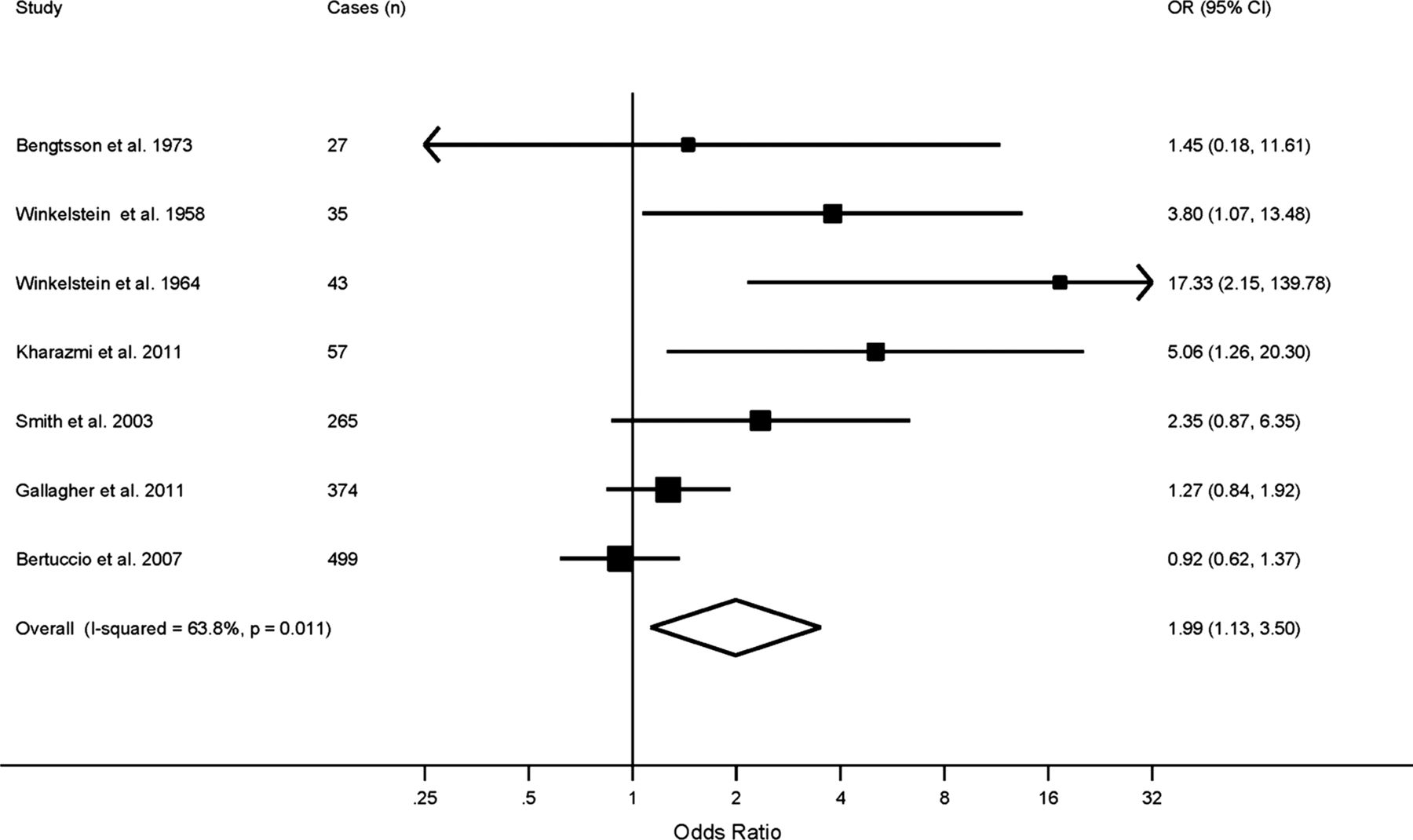
Figures 2 and 3 show the forest plot of the association between miscarriage and CHD. When all studies of CHD and miscarriage were combined, a history of miscarriage was associated with a 45% higher risk of CHD, OR=1.45 (CI 1.18 to 1.78); there was little evidence of between-study heterogeneity (χ2: p=0.203, I2=28.2% (0%, 68%)). There was a strong association between recurrent miscarriage and CHD: OR=1.99 (1.13 to 3.50), although between-study heterogeneity was evident (χ2: p=0.011, I2=63.8% (18%, 84%)).

Forest plot showing the ORs and 95% CIs for studies investigating the association between a history of miscarriage and coronary heart disease. The I2 statistic and the Cochrane χ2 statistic both suggested little between-study heterogeneity, I2=28.2% (0%, 68%), χ2: p=0.203.
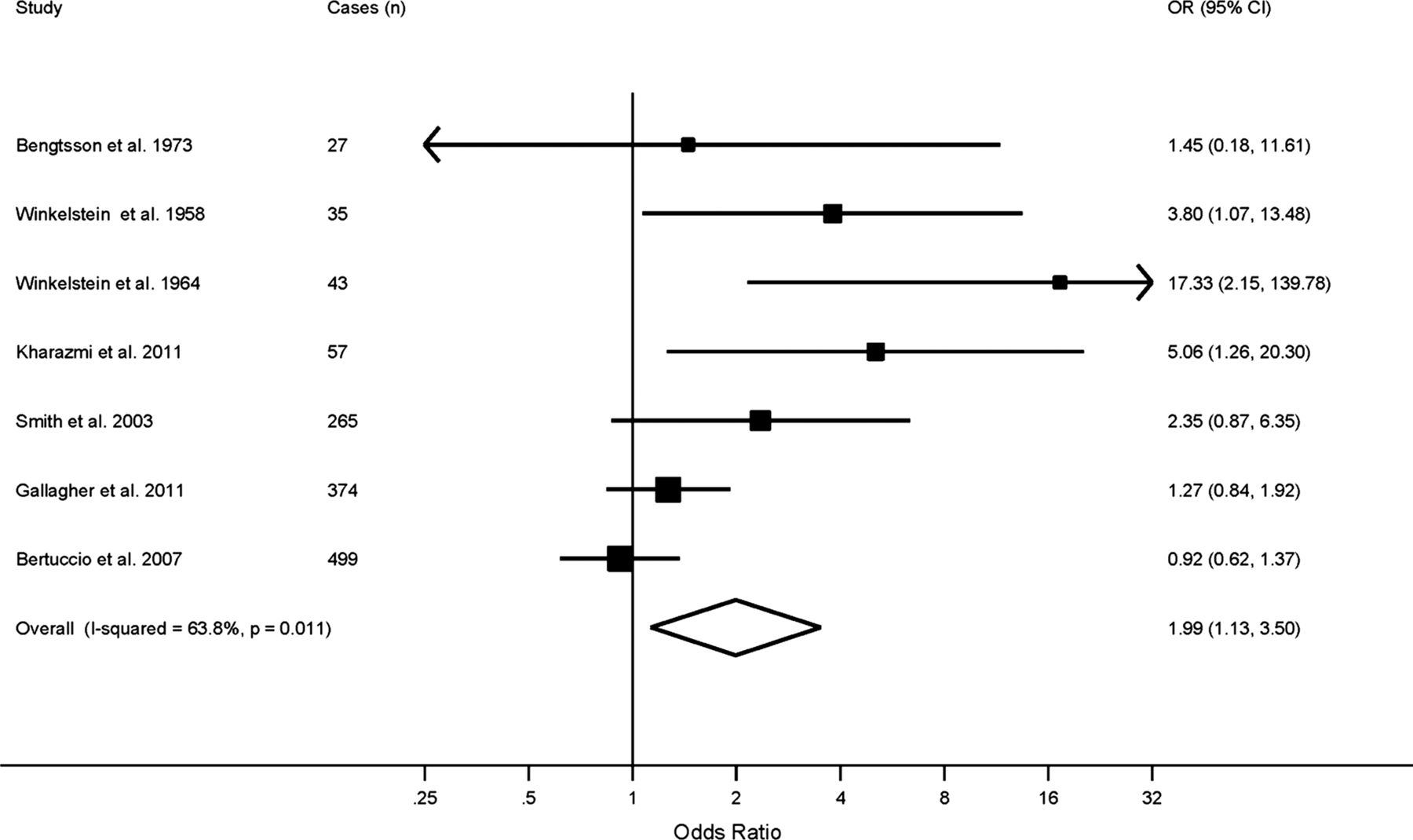
Forest plot showing the ORs and 95% CIs for studies investigating the association between recurrent miscarriage and coronary heart disease. Both the I2 statistic and the Cochrane χ2 statistic indicated between-study heterogeneity, I2=63.8% (18%, 84%), χ2: p=0.011.
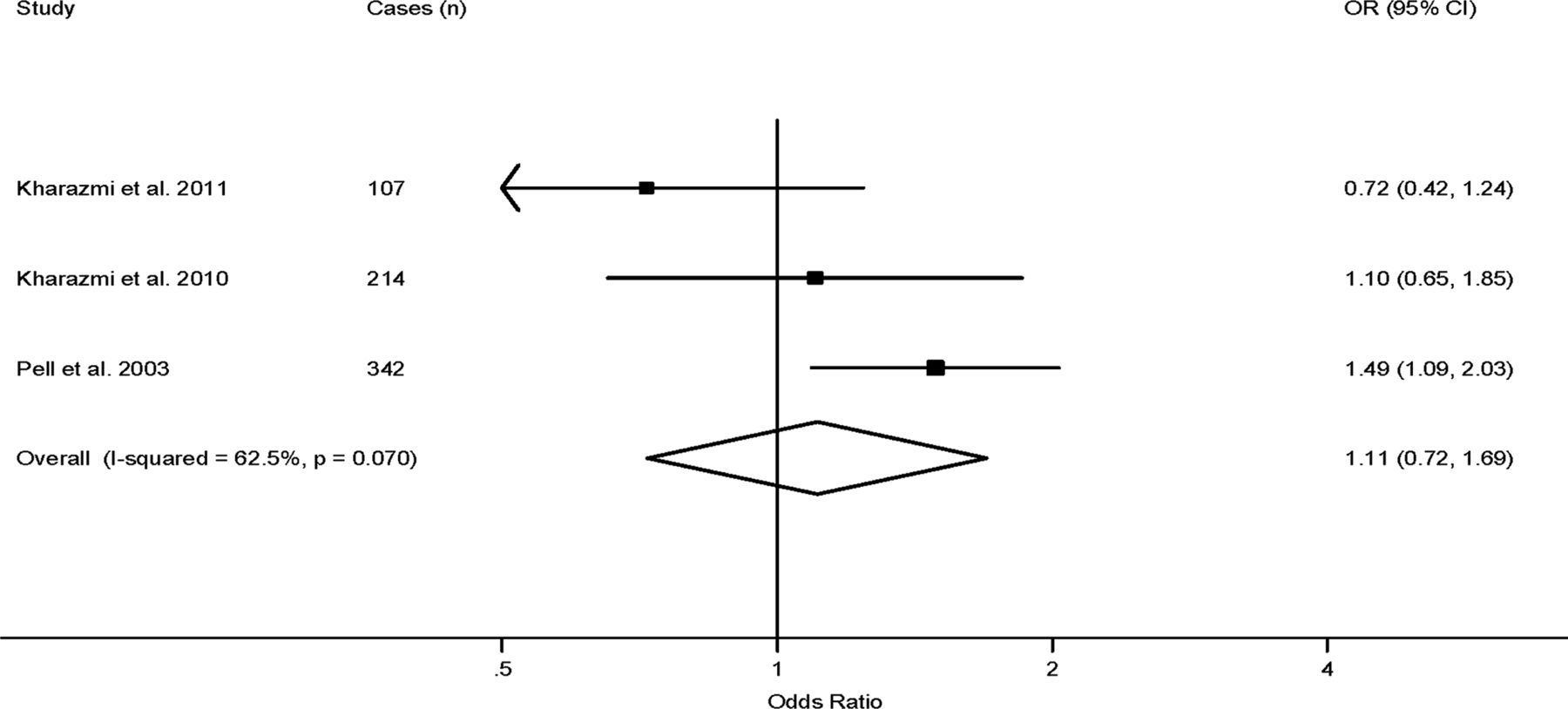
No association was found between miscarriage and cerebrovascular outcomes (figure 4), OR=1.11 (0.72 to 1.69). The I2 statistic indicated between-study heterogeneity (I2=62.5% (0%, 89%)), but the χ2 test was not significant (χ2: p=0.070), although the accuracy of this test will have been impaired by the small number of studies. It was not possible to analyse the association between recurrent miscarriage and cerebrovascular disease, as only two studies assessed this association.

Forest plot showing the ORs and 95% CIs for studies investigating the association between a history of miscarriage and cerebrovascular disease. The I2 statistic indicated between-study heterogeneity (I2=62.5% (0%, 89%)), but the χ2 test was not significant (χ2: p=0.070).
Publication bias
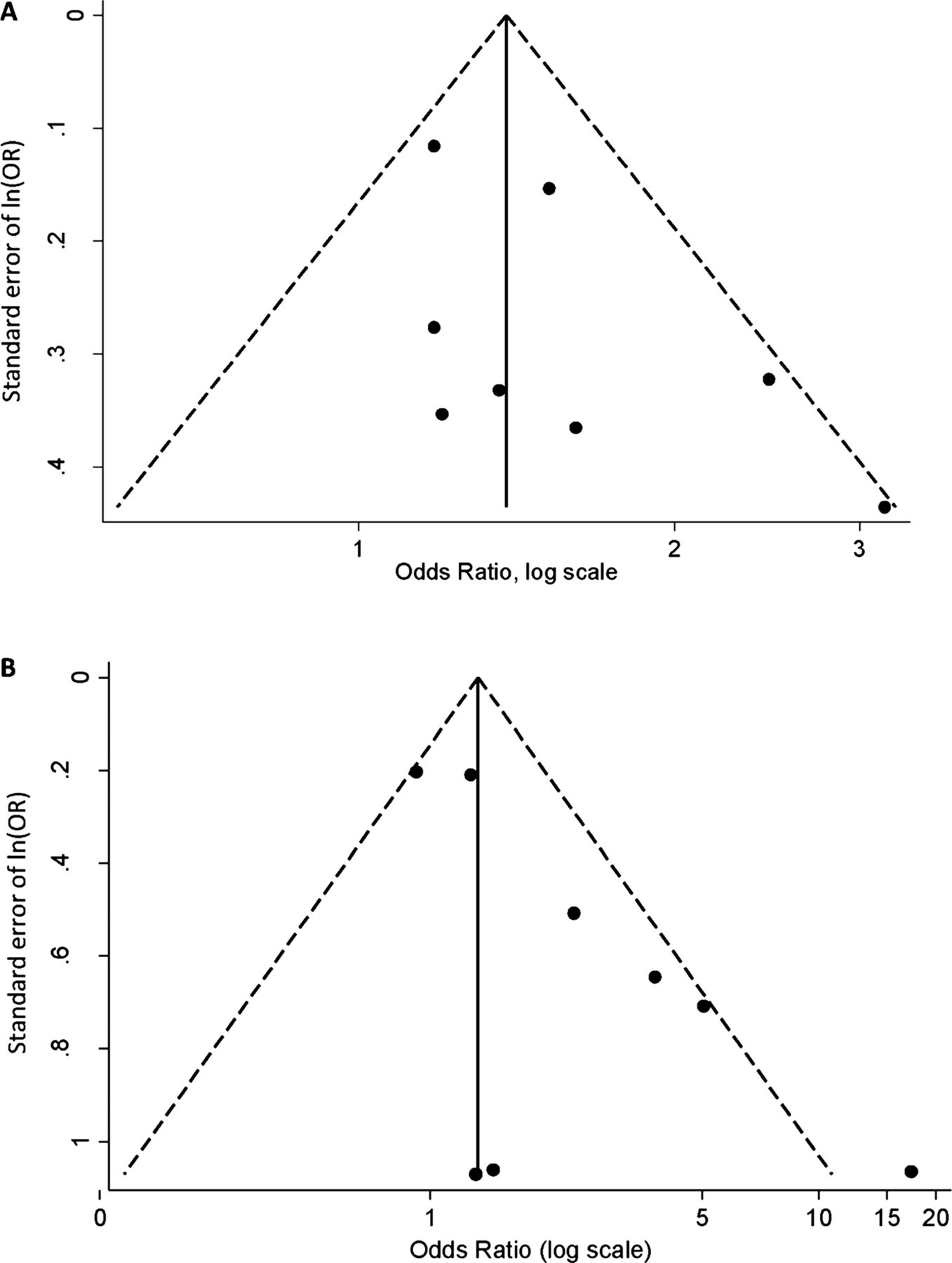
Investigative results for publication bias in the history of miscarriage meta-analysis were inconclusive. Visual examination of the Begg's funnel plots (figure 5A) suggested some small studies with negative effect sizes may be missing, although this was not strongly supported by Egger's test (p=0.213). Greater evidence for publication bias was found in the recurrent miscarriage analysis; Egger's test was significant (p=0.028) and Begg's funnel plot (figure 5B) was asymmetrical, suggesting smaller studies with negative associations were missing,
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Funnel plot of the association between a history of miscarriage and coronary heart disease (CHD). (B) Funnel plot of the association between recurrent miscarriage and CHD.
Due to the limited number of studies, it was not possible to evaluate publication bias in the cerebrovascular disease meta-analysis.
Sensitivity analysis
Additional analyses assessed robustness to confounder adjustment. After exclusion of six studies with little or no adjustment for confounders, which also coincided with a Newcastle–Ottawa Scale of less than 6, there was minimal change in the point estimate of the associations between CHD and a history of miscarriage, OR=1.40 (1.10 to 1.79), or recurrent miscarriage, OR=1.89 (0.69 to 5.13). There was no evidence of heterogeneity for a history of miscarriage (χ2: p=0.650, I2=0.0% (0%, 90%)), although greater heterogeneity was found between the three studies that remained in the recurrent miscarriage analysis (χ2: p=0.023, I2=73.5% (11%, 92%)).
Discussion
This is, to our knowledge, the first meta-analysis investigating the association between miscarriage and future CVD in women. We found that women with a history of miscarriage or recurrent miscarriage are at a higher risk of CHD than women who have not experienced miscarriage(s). On average, women with a history of miscarriage are at a 45% higher risk of CHD, and recurrent miscarriage was associated with a twofold risk of CHD. No association was found between a history of miscarriage and future cerebrovascular events, but due to the small number of studies, it was not possible to analyse the association between recurrent miscarriage and cerebrovascular events.
Several aetiological arguments have been proposed to support a common mechanistic pathway for CVD and miscarriage. Recent evidence suggests that the determinants of the association may aggregate in families, as women with a history of recurrent miscarriage were more likely to have parents who experience CHD.28 This would be supportive of a genetic or epigenetic cause, although behavioural and environmental risk factors will also aggregate in families.
Immune disorders
The association between miscarriage and antiphospholipid syndrome is well established. Antiphospholipid antibodies are directed against phospholipids found in cell membranes, which results in the formation of blood clots. Consequently, women with antiphospholipid syndrome have a greater risk of CHD, intracardiac thrombi, pulmonary embolism, pulmonary hypertension and cardiomyopathy,29 most likely resulting from injury to the cell membranes of endothelial cells.30 Women with antiphospholipid syndrome also have a greater risk of miscarriages, recurrent miscarriage being an indication for testing for antiphospholipids in some cases.31 The greater occurrence of miscarriages may be the result of activation of complement by antiphospholipid antibodies that bind to placental trophoblast cells.30 Other immune disorders including Lupus, which often co-occurs with antiphospholipid syndrome,32 have also been implicated in both CVD33 and miscarriage risk.32
Chronic maternal disease
A number of chronic maternal diseases may mediate the association, including the metabolic syndrome. The metabolic syndrome is a spectrum of metabolic abnormalities associated with insulin resistance, which is manifest as relative hyperglycaemia, hyperlipidaemia and disturbance of coagulation. It is a key factor underlying CVD, and in particular CHD. Several components of this are associated with an increased risk of miscarriage, including coagulation dysfunction,34 ,35 hyperglycaemia36 and insulin resistance.37 ,38 Likewise, uncontrolled diabetes increases the risk of miscarriage39 and CVD, with CVD being the leading cause of death for women with type 2 diabetes.40
Other chronic medical conditions implicated in the association include severe kidney disease, a risk factor for CVD41 and, as diseased kidneys are less capable of making the adaptations necessary for a healthy pregnancy, also a risk factors for miscarriage.42 Endocrinological diseases, such as thyroid disorders43 ,44 and polycystic ovarian syndrome,44 ,45 may also be involved and, finally, heart conditions themselves, which lead to a greater risk of miscarrying as the heart cannot cope with the additional volume load.46
Endothelial dysfunction
Changes in the endothelium, including endothelial dysfunction, are essential for the initiation and progression of atherosclerosis.47 Maternal endothelial dysfunction prior to pregnancy has been suggested to impair the invasion of trophoblasts into the uterine wall, which is necessary for a successful pregnancy. Women with a history of recurrent miscarriages have been found to have higher rates of endothelial dysfunction relative to women who experienced uncomplicated pregnancies,48 and women who have endothelial dysfunction corrected prior to, or early in, pregnancy have improved outcomes.49
There are some limitations to our study. First, we cannot eliminate publication bias, despite a non-significant Egger's test result in the history of miscarriage analysis. Second, moderate between-study heterogeneity was observed which may have arisen from several factors including: (i) different inclusion criteria for premenopausal women, who are still susceptible to miscarriage; (ii) differing selection of hospital or community-based controls in case-control studies; (iii) different exposure definitions: Bengtsson et al17 combined therapeutic abortions and miscarriages as an exposure (exclusion of this study had little impact on the analyses, results not shown), but other studies did not validate self-reported exposure; (iv) differing case ascertainment including use of medical records, death records, self-reports and proxy-reports; (v) differing case definitions for both CHD and cerebrovascular disease; and (vi) varied level of adjustment, although exclusion of unadjusted measures had little impact on the association measures.
Finally, residual confounding may have impacted the results, as indicated by the Newcastle–Ottawa Scale, where mainly case-control studies failed to score well on comparability. Even well-adjusted studies did not adjust for all known confounders, such as smoking15 ,25 or maternal age.15 ,25 ,20 Smoking history was adjusted for in three studies.3 ,33 ,34 The results from these studies were inconsistent, making it unclear how residual confounding may have affected the pooled estimate. One study found a positive association with recurrent miscarriage and CHD;33 another did not.3 The two studies that evaluated a history of miscarriage and CHD while adjusting for smoking found positive, but non-significant results.33 ,34
Previous pregnancy complications have also been suggested as potential confounders, recurrent miscarriage being associated with pregnancy complications that are known to increase the risk of CHD.50 ,51 However, there is evidence that adjustment for pregnancy complications has little impact on the association.15 In contrast, several of the studies that did not adjust for chronic maternal diseases found a significant association between a history of miscarriage and CVD,15 ,26 while the studies which did adjust for them, found a null association,20 ,21 suggesting some residual confounding.
Given the need for better methods of assessing the risk of CHD in women, as up to 20% of CHD events in women occur in the absence of conventional risk factors,52 the utility of reproductive history as a marker of risk is very attractive. There is now an extensive body of work which demonstrates a clinically useful predictive association between complications of late pregnancy and the risk of subsequent CHD. In particular, pre-eclampsia is recognised as an independent risk factor, with a meta-analysis of the association between pre-eclampsia and later CHD showing a 2.16 risk.5 The association we observed between recurrent miscarriage and later CHD was an OR of 1.99. Hence, recurrent miscarriage may be a highly informative marker for CHD.
Given this, it is essential that further studies address whether this association is truly independent of potential confounders, especially chronic medical conditions, which may already be used in the American Heart Association recommendations for women. The true association, independent of chronic medical conditions, may be reflected by an increased risk with recurrent miscarriage alone. This issue could be clarified by calculation of a dose–response relationship; however, only two studies15 ,18 included in this paper reported one.
Additionally, the association needs to be evaluated in other ethnicities. Most studies have come from European and North American populations, with predominately Caucasian participants. Given that CVD rates differ by ethnicity, it is possible that the strength or existence of the association also varies by ethnicity.
These limitations notwithstanding, this meta-analysis indicates that women who experience recurrent miscarriages are at more than twice the risk of CHD relative to women who have not had any miscarriages. Furthermore, women with any history of miscarriage may also have an increased risk of CHD.
References
Footnotes
-
Contributors CTO-W, AMW and GCSS designed the study. CTO-W and EEH performed the systematic literature review and constructed the database. CTO-W analysed the data with the help of AMW and GCSS. CTO-W drafted the first version of the manuscript together with AMW and GCSS. All authors took part in the interpretation of the results and prepared the final version. CTO-W is responsible for the overall content as guarantor.
-
Funding This work was supported by a Medical Research Council (MRC) PhD Studentship.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.