Article Text

Abstract
Objective We examined cognitive function in older hospitalised patients with chronic atrial fibrillation (AF).
Design A prospective substudy of a multicentre randomised trial of an AF-specific disease management intervention (the Standard versus Atrial Fibrillation spEcific managmenT studY; SAFETY).
Setting Three tertiary referral hospitals within Australia.
Patients A total of 260 patients with chronic AF: mean age 72±11 years, 53% men, mean CHA2DS2-VASc score 4±2.
Interventions Cognitive function was assessed at baseline (during inpatient stay) using the Montreal Cognitive Assessment (MoCA).
Main Outcome Measures The extent of mild cognitive impairment (MCI—defined as a MoCA score <26) in AF patients and identification of independent predictors of MCI.
Results Overall, 169 patients (65%, 95% CI 59% to 71%) were found to have MCI at baseline (mean MoCA score 21±3). Multiple deficits in cognitive domains were identified, most notably in executive functioning, visuospatial abilities and short-term memory. Predictors of MCI (age and sex-adjusted) were lower education level (technical/trade school level OR 6.00, 95% CI 2.07 to 17.42; <8 years school education OR 5.29, 95% CI 1.95 to 14.36 vs 8–13 years), higher CHA2DS2-VASc score (OR 1.46, 95% CI 1.23 to 1.74) and prescribed digoxin (OR 2.19, 95% CI 1.17 to 4.10).
Conclusions MCI is highly prevalent amongst typically older high-risk patients hospitalised with AF. Routine assessment of cognitive function with adjustment of clinical management is indicated for this patient group.
- Quality Of Care And Outcomes
Statistics from Altmetric.com
Background
With a reported population prevalence of 1–2%, atrial fibrillation (AF) is the most common sustained cardiac arrhythmia seen in clinical practice.1 The numbers of cases are predicted at least to double by 20501 as the key pathways to AF (including advancing age, chronic forms of cardiovascular disease, hypertension and obesity/metabolic disorders) reach historically high levels. From an individual perspective, AF (in all its forms) confers an independent 1.5–2-fold probability of death in the longer term2 with close links to ischaemic stroke (3–5-fold risk3), heart failure (up to 50% develop AF)4 and acute coronary syndromes (AF (usually paroxysmal) is documented in almost 25% of patients who present to hospital during ischaemic/postischaemic episodes).5 As such, there is a challenge to improve clinical management and subsequent health outcomes.
Despite a growing body of literature, an often forgotten component of the burden of AF, with important clinical implications, is cognitive impairment and vascular dementia. In fact, the prevalence and influence of cognitive impairment is considerable across a wide spectrum of cardiac diseases, with deficits most notably identified in executive functioning.6 A number of studies (predominantly using the mini-mental state examination; MMSE) have identified AF as an independent predictor of cognitive impairment.7–9 Moreover, the prevalence of cognitive impairment in both community dwelling and hospitalised individuals with AF is reported to be approximately 26–51%.8 ,9 Although the pathways to cognitive impairment in AF are not fully understood, in those individuals with AF suffering from concurrent stroke or transient ischaemic attack (TIA), 15–26% have signs of one or more silent cerebral infarcts on computed tomography.10 ,11 Furthermore, AF is regarded as a common cause of white matter low attenuation, most likely due to cerebral hypoperfusion.12 In comparison, population-based studies of ‘healthy’ individuals aged 60–64 years suggest the underlying prevalence of cognitive impairment is a far lower figure of approximately 4%.13 In healthy individuals older than 65 years of age, equivalent prevalence estimates rise to 10–20%.14
Due to the clinical heterogeneity and treatment complexities of AF, careful and balanced management is required to prevent known adverse effects. Individuals with AF and even forms of mild cognitive impairment (MCI) should be considered at higher risk of poorer health outcomes due to the potentially complex requirements of self-managing therapies with narrow therapeutic margins. As such, strict and effective adherence to clinical routines and required treatments is influenced by MCI, potentially impairing a patient's capacity to plan, sequence and carry out tasks associated with AF management/self-care, diminishing a patient's ability to participate in decisions surrounding their medical care and/or determine if they are at high risk of a serious clinical event (eg, a haemorrhagic stroke).
Study objective
We sought to determine the extent of MCI in a cohort of typically older and non-demented patients hospitalised with a diagnosis of chronic AF. We hypothesised that the prevalence of MCI would be high in this cohort.
Methods
Study setting
As part of a systematic approach to risk delineation and optimising the management of hospitalised patients with chronic forms of AF, we are undertaking the Standard versus Atrial Fibrillation spEcific managemenT studY (SAFETY).15 The overall purpose and design of SAFETY has been described in greater detail previously.15 In brief, 335 non-demented patients with chronic forms of AF (see table 1) were randomly assigned into this study and all were subject to comprehensive baseline profiling. Patients were randomly assigned to either usual post-discharge care or a home-based, multidisciplinary, AF-specific intervention designed to reduce morbidity and mortality.
Summary of cognitive function in SAFETY participants at baseline (in hospital)
Wherever feasible, we prospectively measured cognitive function using the Montreal Cognitive Assessment (MoCA) tool that was designed to be more sensitive and specific to MCI.16 The MoCA was applied at the point of recruitment in hospital to all eligible patients. Ethics approval was obtained from the Central Northern Adelaide Health Service Ethics of Human Research Committee, Metro South Health Service District Human Research Ethics Committee, Melbourne Health Human Research Ethics Committee, Western Health Office for Research and the ACT Health Directorate Human Research Ethics Committee. Written informed consent was obtained from each study participant before study procedures were conducted.
Participants
A systematic screening programme to identify eligible inpatients was conducted at each participating hospital. Patients were approached for recruitment if they had a documented diagnosis of recurrent paroxysmal (ie, recurrent episodes by history as documented on ECG), persistent or permanent AF; were living independently in the community or their own home post-hospitalisation; and were able and willing to provide written informed consent to participate. Patients were excluded if they were aged less than 45 years, had a primary diagnosis of valvular heart disease, were scheduled for catheter ablation, had pre-existing chronic heart failure (CHF) as evidenced by the combination of symptoms indicative of New York Heart Association class III–IV with a documented left ventricular ejection fraction less than 45%, or had a transient form of AF. Patients determined to be demented, as assessed on routine evaluations conducted by hospital clinical teams, were also excluded.
Data collection
Baseline profiling
A comprehensive range of sociodemographic and clinical data were collected at baseline. This included basic demographic characteristics (age and sex), education (level of education completed and number of years), subtype of AF, comorbid conditions and CHA2DS2-VASc score to identify those at very high thromboembolic risk (with a score ≥3).17 The CHA2DS2-VASc score is a validated risk stratification tool used to assess the thomboembolic risk of individuals with AF and indicates antithombotic therapy requirements.17 The scoring of eight criteria contributes to the final score of 0–9. Each criterion accounts for one or two points: congestive heart failure or left ventricular dysfunction (one point); hypertension (one point); age 75 years or greater (two points); diabetes mellitus (one point); stroke/TIA/systemic embolism (two points); vascular disease (one point); age 65–74 years (one point); sex category (one point if a woman).17
Assessment of cognitive function
The MoCA is a validated screening tool for cognitive dysfunction that is administered during in-person interview in the clinical setting. The MoCA is designed to delineate MCI patients from those with normal cognition with a greater predictive value than the MMSE.16 Scoring ranges from 0 to 30 and a score of less than 26 is indicative of MCI. Six domains of cognitive function are assessed using the MoCA: executive functioning, visuospatial abilities, language abilities, short-term memory, sustained attention and orientation. Adjustment is made for obtaining a formal education of 12 years or less. Personnel conducting the MoCA were trained according to standardised criteria relating to questionnaire administration, question delivery and scoring.16 Given recent suggestions that a MoCA score less than 24 increases specificity for MCI without impacting on sensitivity (albeit in a younger cohort of individuals with a much lower prevalence of MCI than expected in the SAFETY cohort),18 we compared the two cut-off scores (<26 vs <24) to generate a more conservative prevalence estimate in this cohort.
From a total of 335 SAFETY participants, 260 (78%) were administered the MoCA at baseline (during inpatient stay) to assess cognitive function. For the purpose of this substudy, individuals whose primary language was not English (n=17, 5%) were excluded on the basis of language proficiency affecting MoCA responses,19 and those who were too unwell at the time when testing was attempted were also excluded (n=58, 17%).
Statistical analyses
Descriptive values are presented as mean (±SD) for continuous variables or a proportion for categorical variables. Unadjusted odds ratios (ORs) with 95% confidence intervals (CIs) compared education, AF subtype and comorbidities between patients with and without MCI. Multivariate analyses to determine independent correlates of MCI (referred to here as predictors) were examined with a stepwise linear regression model and adjusted for age, sex, AF subtype, high-risk alcohol use, comorbid conditions (hypertension, type 2 diabetes, cerebrovascular disease, coronary artery disease; CAD) and ‘new AF’ diagnosis (ie, first diagnosis of a chronic form of AF (recurrent paroxysmal, persistent or permanent) not related to a transient physiological state). Further categorisation and analysis of CHA2DS2-VASc scores was undertaken to understand which score(s) confers the independent association with MCI. Data were analysed using SPSS, V.20. A probability value of p<0.05 (two-sided) was considered statistically significant.
Results
Baseline profile
The baseline patient profile (n=260) is presented in table 1 according to the presence/absence of MCI (cut-off MoCA score <26). Overall, 137 (53%) participants were men with a mean age of 72±11 years (more patients with MCI were aged ≥75 years; p<0.01) and 80 (31%) had 12 years or less of formal education. The majority of participants assessed for MCI had persistent AF (n=224; 86%) with 185 (71%) recording a CHA2DS2-VASc score of 3 or greater, indicating a high inherent risk of stroke. The comorbid profile of these patients was extensive: 188 (72%), 84 (32%) and 67 (26%) had hypertension, CAD and type 2 diabetes, respectively. A previous history of stroke/systemic embolism/TIA was present in 41 (16%) patients. AF-specific therapies were prescribed in similar proportions. However, digoxin was significantly more likely to be prescribed to patients displaying MCI (p=0.01).
Baseline cognitive function
The overall mean MoCA score at baseline (prehospital discharge) in this cohort was 23±4; equivalent scores being 21±3 versus 27±1 in those with and without identified MCI, respectively. Overall, 169 patients (65%, 95% CI 59% to 71%), of which 53% were men, recorded a MoCA score less than 26. As shown in table 1, on an unadjusted basis, those with MCI were on average 6 years older than those without MCI (74±10 years vs 68±12 years, p<0.001). A higher proportion of individuals with MCI had less than 12 years of formal education (despite correction for education level). Those classified with MCI also had an increased likelihood of concurrent hypertension (OR 1.61, 95% CI 0.92 to 2.82), CAD (OR 1.67, 95% CI 0.95 to 2.95), type 2 diabetes (OR 1.83, 95% CI 0.98 to 3.41) and stroke/systemic embolism/TIA (OR 1.82, 95% CI 0.85 to 3.91). Consequently, those classified as having MCI also had a higher risk of thromboembolic events with a 2-fold increased likelihood of a higher CHA2DS2-VASc score of 3 or greater (OR 2.18, 95% CI 1.26 to 3.79).
MoCA sensitivity analyses
When applying a lower (more stringent) MoCA cut-off score of less than 24, the proportion of those classified as MCI fell from 65% (95% CI 59% to 71%; cut-off <26) to 49% (95% CI 43% to 55%). Patients classified with MCI on this basis had a mean age of 75±10 years (only slightly older than the original MCI group) and a mean MoCA score of 20±3 compared to 69±12 years and 27±2 for those without MCI, respectively. In both MCI groups, 53% were men.
Affected cognitive domains
Tables 2 and 3 outline the proportion of patients in each group (with or without MCI) demonstrating paired deficits in each affected cognitive domain at the time of testing, as measured by the MoCA. In both groups, high levels of dysfunction were identified in almost all cognitive domains (most notably in executive functioning, visuospatial and short-term memory domains); however, dysfunction in orientation was only seen in 25% and 2% of individuals with and without MCI, respectively. Overall, deficits were more extensive in those with MCI. In total, only 11 individuals obtained a ‘perfect’ MoCA score of 30.
Proportion of patients with MCI (n=169) demonstrating deficits within each cognitive domain
Proportion of patients without MCI (n=91) demonstrating deficits within each cognitive domain
Predictors of MCI
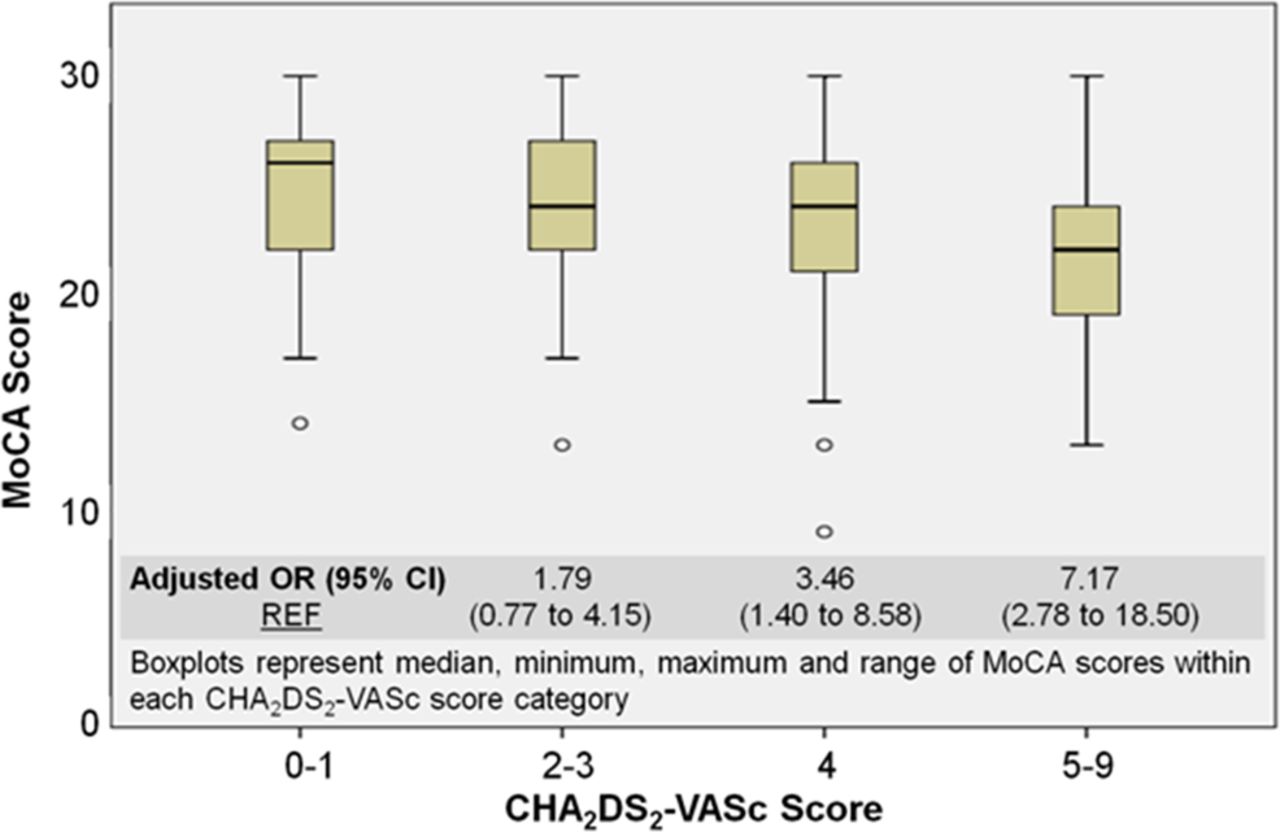
Table 4 shows the independent predictors of MCI. MCI was more likely in those reporting lower levels of education (including <8 years education or trade qualifications) and in those with a higher CHA2DS2-VASc score. The odds of MCI increased by 46% for every unit increase in the CHA2DS2-VASc score. In addition, those prescribed digoxin were more likely to demonstrate MCI. Further analysis of a subgroup of patients (n=32) who had digoxin levels tested at the time of MoCA administration revealed a (non-significant) trend towards those with MCI having, on average, a lower body mass index (28.5±6.6 kg/m2) but higher serum digoxin levels (0.96±0.34 µg/l) in contrast to those without MCI who had, on average, a higher body mass index (30.0±5.7 kg/m2) and lower serum digoxin levels (0.45±0.08 µg/l). Figure 1 shows a more detailed description of the relationship between the CHA2DS2-VASc score and MCI. An incremental decrease in the MoCA score (ie, an increased likelihood of demonstrating MCI) with higher CHA2DS2-VASc scores was shown.
Independent predictors of MCI (age and sex adjusted)

{kind=link}
Correlation between CHA2DS2-VASc and Montreal Cognitive Assessment (MoCA) scores. This figure is only reproduced in colour in the online version.
Discussion
Consistent with the high potential for cognitive decline and vascular dementia7 in a typical cohort of 260 older individuals hospitalised with chronic AF, we found that a high proportion of our study cohort (approximately two-thirds) displayed concurrent MCI. Even with a more stringent definition (ie, lowering the qualifying MoCA score to <24) the underlying prevalence of MCI was approximately half. Deficits in executive functioning, visuospatial abilities and short-term memory were common, as were overlapping deficits across multiple cognitive domains. Those found to have MCI were more likely to have lower education levels and the highest thromboembolic risk (primarily calculated on the basis of more advanced age and cardiovascular insults) while being most likely to be prescribed agents with the narrowest benefit-to-risk ratios.
As such, these data confirm previous studies suggesting high levels of cognitive dysfunction in those with AF.8 ,9 They also represent an important clinical warning, particularly given that the risk factors we identified are frequently seen in those being treated for AF. The role of digoxin, a commonly prescribed drug in the presence of AF, but with clear potential for toxicity and associated mental confusion in older individuals,20 ,21 in potentially contributing to MCI in this cohort is also an important finding. Low digoxin levels (0.5–0.8 µg/l) have been shown to be associated with better clinical outcomes (including cognitive functioning) and lower mortality.21 However, cognitive impairment has also been found to occur at levels of serum digoxin that are within the therapeutic range.20 ,22 In the current study, those with MCI and concurrent digoxin levels had lower body weight but greater digoxin levels, potentially reflecting higher tissue saturation and, thus, digoxin toxicity albeit at a therapeutic level. Recommendations have been made outlining the need for digoxin withdrawal in any patient displaying cognitive symptoms, even when the serum digoxin level is within the normal therapeutic range.20
Our findings are of obvious clinical concern in AF due to the heavy reliance on self-care behaviours crucial to managing this complex chronic disease successfully. Inadequate self-care has been identified as a major contributor to hospital readmission and to the poor outcomes associated with heart failure;23 the same can be assumed for AF. Cause and effect is difficult to delineate, however. Individuals with MCI may have problems performing complex tasks such as preparing meals or paying bills while still being able to perform activities of daily living (and thus maintain a sense of independence).24 The ability to learn and acquire knowledge is also influenced by MCI, and lack of knowledge about chronic disease and self-care has been shown to result in poor self-care maintenance and management behaviours.25 Intact executive functions have been identified as crucial for the management of chronic conditions.26 Impaired executive functioning limits an individual's ability to recognise symptoms and make decisions related to symptom management.27 These were all factors that influenced the subsequent management of those allocated to the intervention arm of SAFETY—with incremental surveillance and support applied according to a traffic-light classification system28 that ‘titrates’ post-discharge support in this context using more than just clinical parameters to determine an increased risk of suboptimal health outcomes. In this case, the presence of MCI signified a need to modify expectations of ‘self-care’ and increase the role of caregivers and other healthcare providers (eg, incremental community pharmacist support and/or use of medicine reminder tools). Whether this was sufficiently robust in terms of additional support will be a major factor in determining the overall success of the home-based, nurse-led intervention being compared to usual post-discharge care.15
Beyond the impact of the SAFETY intervention, these data have immediate clinical implications. Screening of MCI can and should be used as a risk delineation strategy to add to the suite of risk stratification tools available for the assessment of patients with AF. Pitfalls of therapy, clinical lability or adverse behaviours can be identified and highlighted, triggering increased patient surveillance for those at high risk of instability or events. Increased surveillance is often required to promote treatment adherence and self-care management. In addition, education focussed on addressing peripheral risk factors can be tailored according to individual needs. Furthermore, AF-specific interventions should be focused on strengthening the areas of cognition most commonly affected. In their recent systematic review, Eggermont et al6 suggested that MCI may be addressed simply by optimising cardiac treatment. The incorporation of physical activity programmes into interventions has also been suggested due to positive improvements in cognition observed in patients with CAD and chronic heart failure.6 ,29 In addition to the screening and detection of MCI, identifying associated independent predictors of lower education level, higher thromboembolic risk and the use of digoxin allows the potential to address or increase surveillance on these peripheral factors in an attempt to prevent the development of MCI and vascular dementia in those who present with AF.
There are a number of limitations that require comment. First, we applied only one clinical assessment tool to assess cognitive function. While the MoCA has been shown to be more sensitive and specific at discerning cognitive deficits than the MMSE, more extensive psychometric testing in addition to the testing of functional capacity would be required to confirm the presence of MCI.18 However, the MoCA could reasonably constitute an initial screening of MCI due to its short length (approximately 10 min) and ease of administration. It is also publicly available for use. The decision to use less than 26 as the cut-off score for defining MCI also influences this research, particularly when such a large decrease in the proportion of classified MCI within this population was observed in the sensitivity analysis. Whether a more stringent cut-off of less than 24 is required for more specific determination of the prevalence in these patients should be the subject of further research. The exclusion of non-English-speaking individuals may have introduced selection bias, although English competency is necessary for comprehensive understanding of the test questions. Furthermore, the often chaotic acute clinical setting under which the MoCA was conducted in addition to the patients’ altered health state may not represent an ideal testing situation. Moreover, the duration and cause of MCI is not known and cannot be distinguished in this cohort. Finally, despite the selection of a ‘real world’ cohort, we cannot discount the possibility of bias in study selection and these data may not readily apply to other hospitalised cohorts.
Despite these limitations, these data have important clinical implications for the post-discharge management of patients with chronic AF. We found that MCI is highly prevalent in typically older patients who have been hospitalised with chronic AF before discharge. Overall, cognitive deficits are abundant in this population. Beyond education levels, MCI correlated with increasing thromboembolic risk and the use of digoxin. In addition, residual levels of MCI remain high in these individuals post-discharge. Therefore, we would recommend that patients with AF should be routinely screened for MCI (as a potential source of risk delineation), and subsequent disease management programmes implemented in the setting of AF (as has been recommended in relation to heart failure management)30 should be modulated if MCI is detected.
Conclusion
MCI is common in high-risk patients hospitalised with chronic AF and is potentially related to poorer health outcomes. Assessment of patients with chronic AF should include MCI screening using the MoCA, an easily administered and effective tool that identifies patients for whom more intensive surveillance is required to maintain clinical stability and optimise management.
References
Footnotes
-
Contributors All authors contributed to the study design, data analysis, manuscript writing, reviewing and editing.
-
Funding The SAFETY study is funded by a National Health and Medical Research Council of Australia Programme Grant (519823). In addition, JB, MJC and SS are supported by the National Health and Medical Research Council of Australia. The study was supported in part by the Victorian government's operational infrastructure support programme. The National Health and Medical Research Council of Australia and the Victorian Government had no involvement in the study design; data collection, analysis and interpretation; or writing or preparation of this manuscript for publication.
-
Competing interests None.
-
Ethics approval This study was approved by the human research ethics committee(s) associated with each of the study sites (hospitals).
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; internally peer reviewed.