Article Text

Abstract
Introduction Timing of surgery for patients with mitral valve prolapse and severe mitral regurgitation (MR) remains problematic. In the absence of symptoms, current guidelines emphasise the importance of left ventricular (LV) size and function, pulmonary artery pressures and the development of AF in helping to determine the need for intervention in these individuals. Little is known regarding the impact of chronic mitral regurgitation on atrial physiology, nor has the association between atrial function and the timing of mitral valve surgery been investigated.
Methods We included consecutive patients reviewed in our specialist valve service. All underwent clinical and echocardiographic assessment. We divided patients according to the severity of MR and whether they had accepted indications for surgery. Echo data recorded included: LV dimensions, LV function, pulmonary artery pressure, and MR severity using the PISA method. Additionally, we measured maximal and minimal left atrial volume (LAV) using the Simpsons biplane method, from which we derived the atrial volume change (AVC), defined as:
Finally, using 2D speckle imaging from the apical 2- and 4-chamber views, we recorded the three components of atrial strain: peak negative (contractile), peak positive (conduit), and total (reservoir).
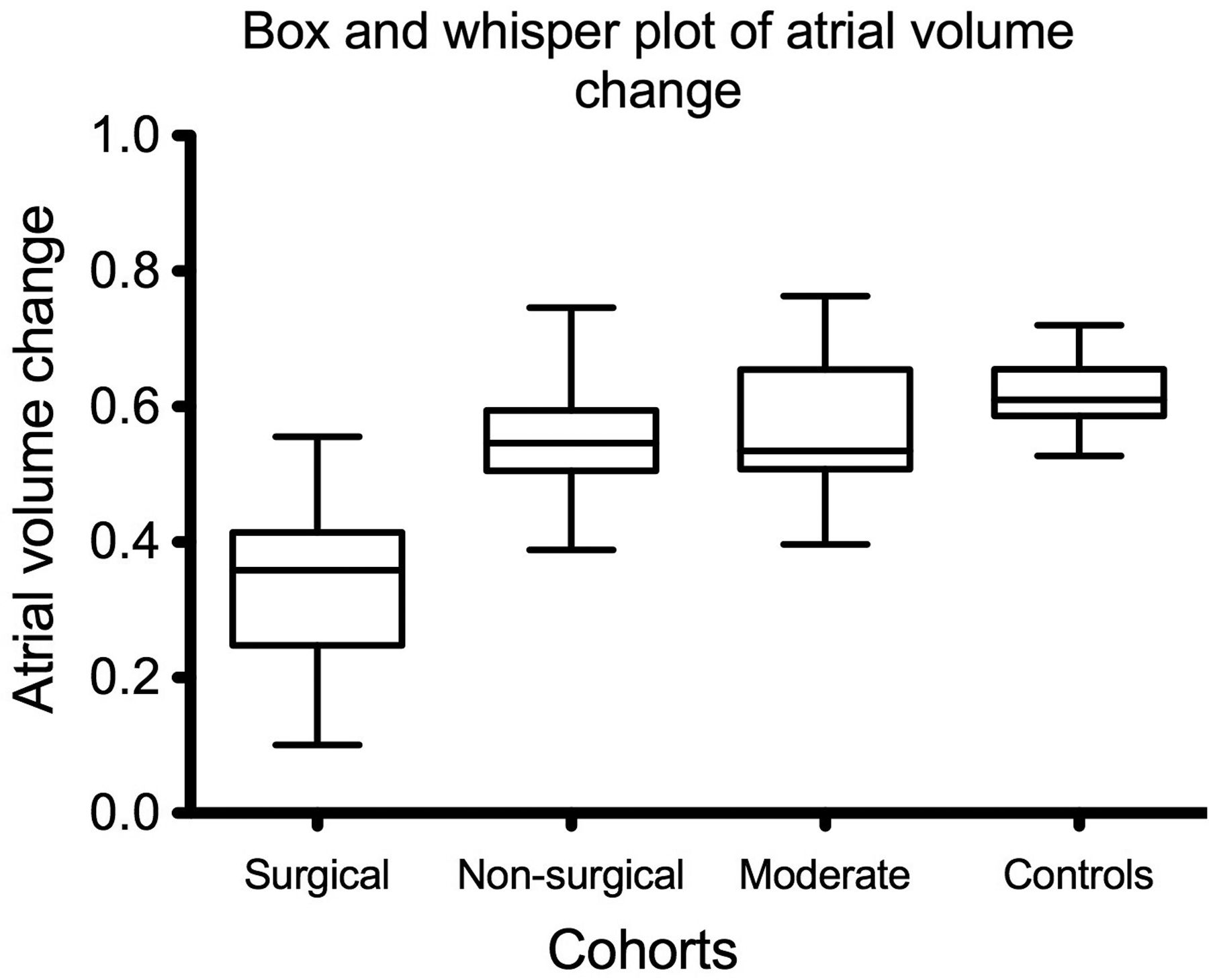
Results We included 160 patients, divided into 4 groups: severe MR with an indication for surgery (surgical; n=77); severe MR with no surgical indication (non-surgical; n=26); patients with moderate or less MR (moderate; n=32) and 25 controls. AVC correlated strongly to total atrial strain (r=0.86; p<0.0001). AVC was similar in the control, moderate and non-surgical groups, but was significantly lower in the surgical cohort (see Graph 1: AVC surgical 34±10%; non-surgical 55±9%; moderate 57±11%; controls 62±6%; p<0.001 surgical vs other groups), with a similar pattern seen for total atrial strain. The contractile component of atrial function was highest in controls, was reduced similarly in moderate and non-surgical patients, and was reduced further in the surgical group (Graph 2: negative strain surgical −4.5±5.2; non-surgical −14.8±8.0; moderate −14.6±9.3; controls −20.8±5.6). Receiver-operator curve analysis demonstrated that an AVC of <50% is 97% sensitive and 87% specific for severe MR requiring surgical intervention.
Conclusions The atrium adapts to chronic mitral regurgitation by increasing conduit function at the expense of the contractile component of atrial strain. With ongoing MR the atrium loses overall reservoir capacity and develops a reduced AVC. Loss of normal atrial volume change accurately predicts the need for surgical intervention in these patients and may be useful in guiding surgery in asymptomatic individuals.⇓ ⇓


{kind=link}
{kind=link}