Article Text

Abstract
Objective: To investigate the usefulness of N-terminal pro-brain natriuretic peptide (NT-proBNP) as a predictive marker for angiographically significant coronary artery disease (CAD) and CAD severity compared with other newer biochemical risk markers and classic risk factors in patients with clinically suspected CAD.
Design: Cross-sectional evaluation of NT-proBNP in a large consecutive series of patients without a history of myocardial infarction referred for elective coronary angiography (CAG) between March 2004 and January 2005. The value of NT-proBNP for predicting CAD was assessed and compared with high sensitivity C-reactive protein (hs-CRP), γ-glutamyltransferase (GGT) and traditional risk factors.
Setting: Tertiary care centre, Department of Cardiology, Innsbruck Medical University, Austria.
Patients: 561 men and 287 women aged between 20–86 years (median 65 years).
Interventions: None.
Main outcome measures: Association of NT-proBNP with the severity of CAD, left ventricular dysfunction and comparison of predictive values of NT-proBNP, hs-CRP, GGT and traditional CAD risk factors.
Results: Of all tested newer biochemical risk markers NT-proBNP performed best. In a multinomial logistic regression model NT-proBNP but not hs-CRP or GGT was significantly associated with three-vessel CAD adjusted for age, sex, ventricular, renal function and classic risk factors (odds ratio = 1.667; 95% CI 1.003 to 2.772; p = 0.049). However, NT-proBNP had no additive predictive value to traditional cardiovascular risk factors for the prediction of angiographically significant CAD in a binary logistic regression model.
Conclusions: The predictive value of NT-proBNP for CAD severity is better than that of hs-CRP or GGT. However, NT-proBNP is also of limited value compared with traditional risk factors for predicting significant CAD.
Statistics from Altmetric.com
There is growing clinical interest in the use of newer biomarkers to identify individuals who are at risk for the development of myocardial infarction and who could benefit from preventive measures. B-type natriuretic peptide (BNP) and the N-terminal fragment (NT-proBNP) of its pro-hormone are already well established as diagnostic markers of heart failure and as risk markers in heart failure and acute coronary syndromes.1 2 The predominant stimulus for the synthesis of BNP is an increase in ventricular wall stretch.3 4 However, recent evidence suggests that ischaemia may be an additional stimulus for synthesis and BNP release.5–7 Myocardial ischaemia can induce a reversible increase in regional wall stress that may lead to augmented natriuretic peptide release. The observations that natriuretic peptide levels are increased in patients with stable coronary artery disease (CAD) after episodes of ischaemia and the association between BNP and inducible myocardial ischaemia 8–11 are in agreement with these experimental and previous clinical findings.5–7
In addition, several clinical studies have investigated the relation between vascular inflammation and atherosclerosis.12 High sensitivity C-reactive protein (hs-CRP) emerged as the most predictive inflammatory marker for CAD, which is suitable for routine measurement.13 CRP is an acute phase reactant that is synthesised in the liver. It is a sensitive marker for inflammatory response and already clinically used for cardiovascular risk stratification.13 Further, γ-glutamyltransferase (GGT), a commonly used diagnostic marker for liver function,13 has recently gained interest as a marker for cardiovascular risk stratification as well.14 Several recent studies showed that it is also associated with morbidity and mortality from causes other than liver disease, including cardiovascular disease.14 15
The available data on the comparative values of NT-proBNP, hs-CRP, GGT and traditional risk factors as a screening tool for the prediction of angiographically significant stenoses in patients without a history of previous myocardial infarction and with suspected CAD is limited. Therefore we conducted the present study with the aim of investigating the association of NT-proBNP concentrations with the severity of CAD in patients without previous myocardial infarction, and to test its usefulness as a predictor of significant CAD and the severity of CAD at coronary angiography (CAG) compared with the above mentioned other newer biochemical risk markers (hs-CRP, GGT) and with the traditional clinical risk factors for the presence of CAD.
METHODS
Study population
This cross-sectional diagnostic test evaluation was performed according to the Declaration of Helsinki. We screened 1315 consecutive patients (885 men and 430 women referred for elective CAG to the Department of Cardiology at Innsbruck Medical University between March 2004 and January 2005. All patients with a history of a previous myocardial infarction, with heart valve disease or after heart transplantation were excluded, leaving a total of 848 patients (561 men and 287 women) aged between 20 and 86 years (median 65 years) as a final study population. Cardiovascular risk factors were assessed by standardised questionnaire and blood chemistry.
Coronary angiography
CAG was performed using the standard Judkins technique by experienced invasive cardiologists who were blinded to NT-proBNP and hs-CRP test results. Angiographically significant CAD was defined as at least 70% lumen diameter reduction of major epicardial coronary arteries at visual estimation. Patients were classified as having one-vessel, two-vessel or three-vessel disease, as having non-significant diffuse CAD (defined as lumen irregularities <70% lumen diameter reduction) or no CAD (no lumen irregularities). A stenosis >50% of the left main artery was also defined as significant CAD.
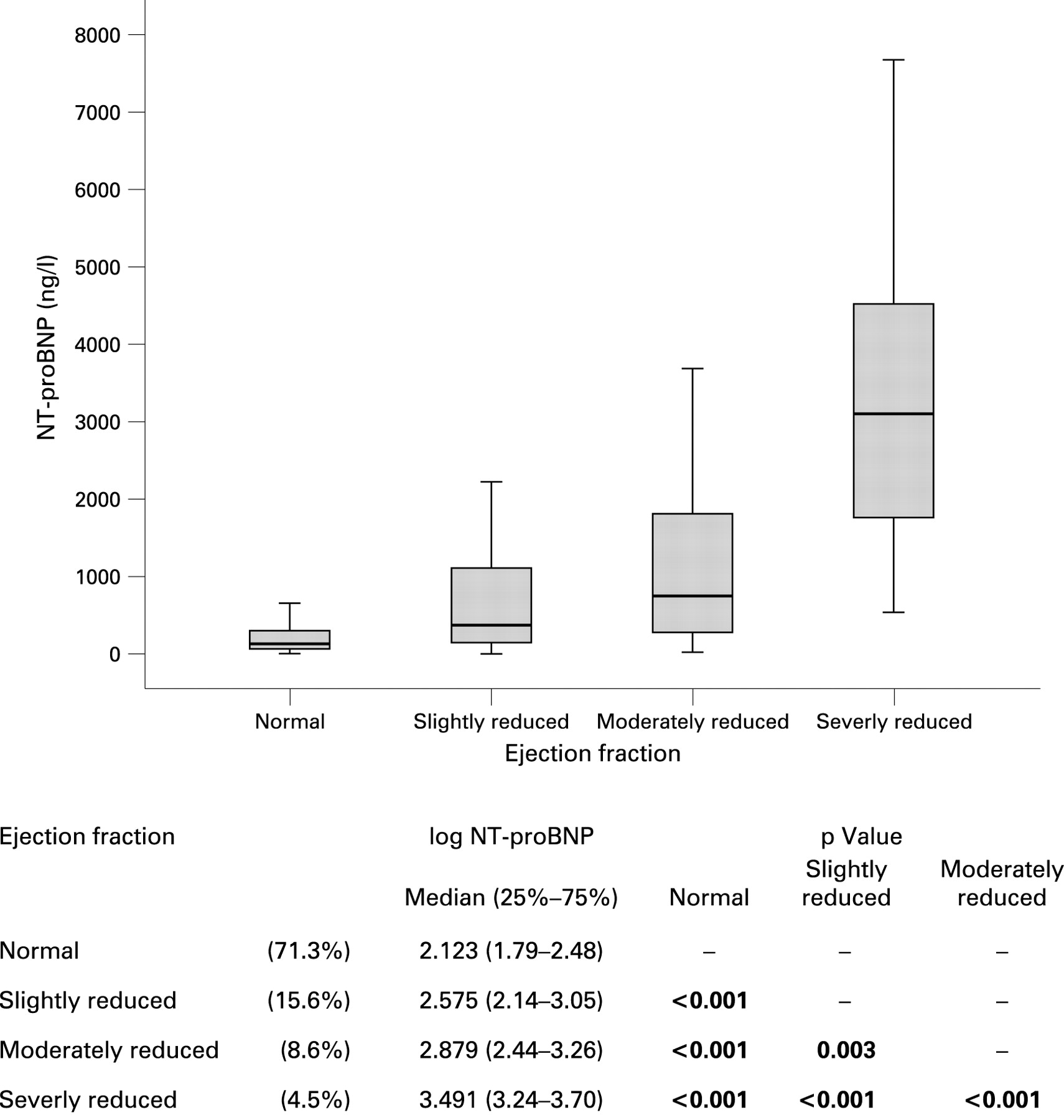
Left ventricular ejection fraction (LVEF) was calculated from the right anterior oblique view using the area-length method. For statistical analysis patients were divided into four groups: normal (LVEF >60%), slightly (LVEF 45–60%), moderately (LVEF 30–45%), and severely reduced LVEF (LVEF <30%).
In patients with significantly reduced kidney function the LVEF was determined by echocardiography using the modified Simpson rule. For statistical analysis patients were divided into four groups: normal (LVEF >50%), slightly (LVEF 40–50%), moderately (LVEF 30–40%) and severely reduced LVEF (LVEF <30%).
Biochemical parameters
Blood samples were drawn routinely the day before CAG was performed. Routine methods from Roche Diagnostics were used to determine serum concentrations of standard biochemical parameters, such as glucose, GGT and other liver enzymes, creatinine, urea, uric acid, triglycerides, total cholesterol, high-density lipoprotein (HDL), and low-density lipoprotein (LDL)-cholesterol. NT-proBNP was measured in heparinised plasma sample remnants by a commercially available immunoassay on an E170 Analyzer (Elcsys proBNP, Roche Diagnostics, D-68298 Mannheim, Germany) as previously described.16 hs-CRP concentration was determined by an immunoturbidimetric test (Tina-quant CRPLX, Roche Diagnostics, D-68298 Mannheim, Germany). GGT was measured with a liquid test from Roche Diagnostics (D-68298 Mannheim, Germany). LDL and HDL concentrations were also measured directly with enzymatic colorimetric assays from Roche Diagnostics (HDL-C plus second generation/LDL-c plus second generation, Roche Diagnostics, D-68298 Mannheim, Germany).
The glomerular filtration rate (eGFR) in millilitres per minute per 1.73 m2 was calculated by using the “modification of diet in renal disease” (MDRD) equation: (186 × (serum creatinine)−1.154 × (age)−0.203) multiplied by a constant of 0.742 if the patient is female.17
Statistical analysis
NT-proBNP and other non-normally distributed variables (GGT, aspartate aminotransferase, hs-CRP, creatine kinase, eGFR and triglycerides) were log-transformed. Analysis of variance (ANOVA) with post hoc Bonferroni correction, t tests or the Mann-Whitney U test and the χ2 test were used for comparison of groups. Pearson or, when appropriate, Spearman rank correlation coefficients were calculated. To identify significant associations of NT-proBNP we calculated a multiple linear regression model. Subjects were also divided into different groups: patients with and without angiographically significant CAD for a binary logistic regression analysis to identify significant predictors of angiographically significant CAD, and into patients with no, diffuse one-vessel, two-vessel and three-vessel CAD for a multinomial logistic regression model for the prediction of CAD severity with the reference catagory no CAD. All tests were two-sided and p values of <0.05 or lower according to the Bonferroni correction were considered as statistically significant. We used the software package SPSS V12.01G for all statistical analysis.
RESULTS
Table 1 lists all demographic and clinical characteristics as well as fundamental measurements according to CAD status. Patients with significant CAD had significantly (p = 0.01) and markedly higher NT-proBNP concentrations than patients with exclusion of CAD angiographically.
The values of NT-proBNP concentrations in relation to the extent of CAD are shown in figure 1. ANOVA revealed significant differences between groups (p<0.001). Patients with three-vessel disease had significantly higher NT-proBNP concentrations (p<0.012) than all other groups exept for two-vessel disease after Bonferroni correction. The relation of NT-proBNP concentrations with LVEF and eGFR are shown in figures 2 and 3. There were clear inverse and significant relations between LVEF and eGFR with NT-proBNP. More than 70% of the patients had a normal LVEF (see fig 2), and ANOVA revealed significant differences between LVEF groups (p<0.001). All LVEF groups differed significantly from each other after Bonferroni correction (p<0.003). The frequencies of significant CAD, hypertension without significant CAD and of dilated cardiomyopathy in the different LVEF groups are listed in table 2.


ANOVA revealed significant differences between eGFR groups (p<0.001) as well. All eGFR groups differed significantly from each other after Bonferroni correction (p<0.001) except for stage 1 v 2 (p = 0.123).
The predictive value of NT-proBNP for the severity of CAD with the reference category no CAD is shown in figure 4. This multinomial logistic regression demonstrated that in contrast to hs-CRP and GGT an increasing NT-proBNP concentration is a statistically significant independent predictor for three-vessel disease (odds ratio 1.667, 95% CI, p = 0.049). This model was adjusted for age, sex, ventricular function, renal function and classic risk factors and confirms the association of NT-proBNP with CAD severity, which is also shown in figure 1, after adjustment for possible confounding variables.

Parameters independently associated with plasma NT-proBNP
Parameters which are independently associated with plasma NT-proBNP concentration by multiple linear regression analysis are listed in table 3. Significant predictors of increased NT-proBNP concentrations were increasing age, reduced LVEF, high concentration of hs-CRP, pathological resting ECG and an eGFR <60 ml/min/1.73 m2. Decreased NT-proBNP concentrations were associated with high haemoglobin. This model predicted 50.6% of the variability of NT-proBNP.
Predictors of angiographically significant coronary artery disease
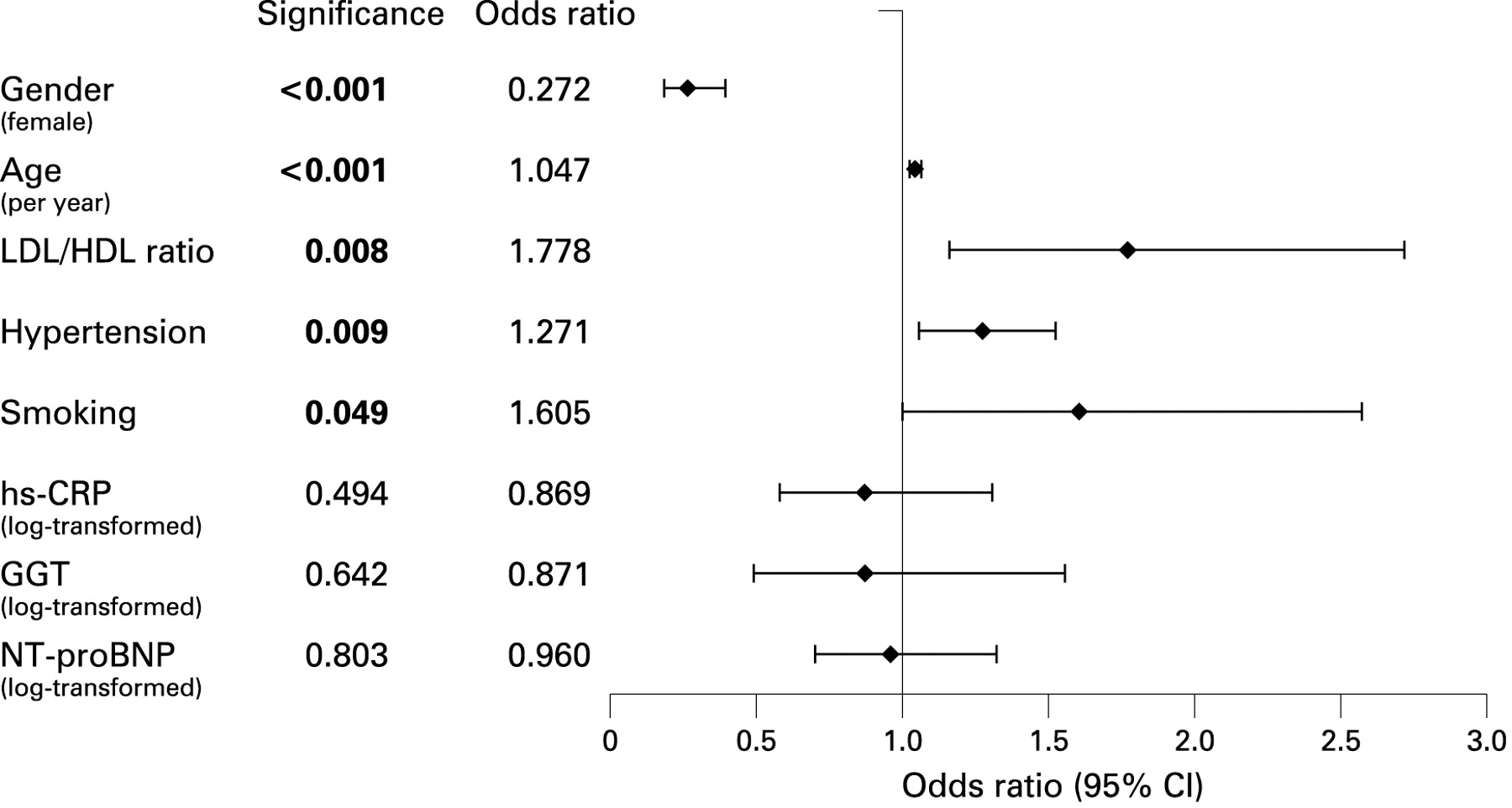
The parameters which are independently associated with significant CAD at angiography by binary logistic regression analysis are shown in figure 5. Statistically significant predictors for angiographically significant CAD are increasing age, smoking, hypertension and high LDL/HDL ratio. Female gender is a parameter which decreased the risk for CAD. All biochemical markers were not independent predictors of angiographically significant CAD in this model. Thus, NT-proBNP is only a significant, independent predictor for the most severe form of CAD—that is, three-vessel disease (see fig 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
DISCUSSION
The novelty of our study is the comparison between NT-proBNP, hs-CRP and GGT as markers for CAD severity. We found that of these biomarkers NT-proBNP performed best in this context, but NT-proBNP had no additive predictive value to traditional risk factors for the prediction of angiographically significant CAD either. We confirm the associations of NT-proBNP with age, the degree of left ventricular and renal dysfunction in a large study population. In contrast to previous results in the general population18 gender had no significant influence on NT-proBNP concentrations in our study population of patients with suspected CAD, which is in accordance with a recently published similar study in patients with comparable average age.19 The median NT-proBNP concentration of our study population without CAD was also higher than the frequently used cut-off value of 125 ng/l. This is attributed to the clinical preselection of patients and the high average age of our study population. We found a weak, independent association of NT-proBNP with three-vessel CAD, which confirms previously published reports10 19 20 and supports the hypothesis of recurrent episodes of myocardial ischaemia as a stimulus of BNP synthesis and release independently of LVEF and eGFR. An association of BNP baseline values adjusted for ventricular function with inducible myocardial ischaemia has been reported in patients with a history of myocardial infarction and stable CAD.10 11 This is in accordance with the independent association of NT-proBNP with three-vessel CAD with a high probability of recurrent episodes of myocardial ischaemia, which we found in patients without previous myocardial infarction, and NT-proBNP concentrations were significantly increased also in angiographically significant CAD compared with patients without CAD. However, the severity of CAD was no statistically independent determinant of NT-proBNP concentrations in a multiple linear regression model. Thus, it is unlikely that this marker will gain clinical importance for selecting patients who need coronary interventions. A possible limitation of our study is that the severity of CAD was based on visual examination of angiograms by experienced invasive cardiologists without data from fractional flow reserve measurements. Although there are several studies on the incremental prognostic value of NT-proBNP in patients with myocardial infarction, unstable and stable CAD, acute chest pain and also in the general population21–23 the available data on the independent association of NT-proBNP concentrations with angiographically assessed severity of stable CAD are limited. The authors of a recent similar study20 in which NT-proBNP was investigated in 781 patients with normal LVEF referred for CAG concluded that NT-proBNP may improve non-invasive prediction of CAD. However, the final study population of the latter study was highly preselected by excluding diseases which may increase NT-proBNP (LVEF <60%, heart failure, acute coronary syndromes, pulmonary diseases, arrhythmias, valvular heart disease, renal insufficiency). It is not likely that their conclusions are valid in a more heterogeneous population in “real world” conditions as the reported area under receiver operating characteristic curves was only 0.72, which indicates moderate diagnostic accuracy at best. Thus, the latter study results and our conclusion that NT-proBNP measured at rest does not provide incremental information for non-invasive prediction of significant CAD in a routine setting are not conflicting. Our study confirms the results of Kragelund et al who reported a poor performance of NT-proBNP as a screening test for CAD.19 In contrast to our study patients with known CAD (history of acute myocardial infarction) were also included in the latter study.
In contrast to previously published studies we also compared NT-proBNP with other newer biochemical markers suggested for risk stratification (hs-CRP, GGT) in CAD and thus extend earlier studies. We found that among these newer recently proposed prognostic markers NT-proBNP was the best predictive biochemical marker in a “real world” scenario for the presence of angiographically assessed significant CAD in patients without a history of previous myocardial infarction. hs-CRP showed no significant association with CAD severity assessed by CAG despite its repeatedly confirmed prognostic value13 and its recently reported value for predicting all-cause mortality in a large urban population.24 This confirms previous considerable smaller studies in patients with stable angina pectoris25 and patients admitted with acute chest pain.26 The present study is to the best of our knowledge the first investigation of the relation of GGT with the angiographically assessed severity of CAD. Although GGT activities were significantly higher in patients with significant CAD than in patients with angiographically exclusion of CAD, the absolute difference was small and is most probably too small to be of clinical relevance considering also the imprecision of enzymatic assays for GGT determination and the unspecificity of this enzyme. Moreover, GGT was not an independent predictor of significant CAD or CAD severity.
Compared with the classic risk factors all newer biochemical markers were weak predictors of significant CAD and had no additive predictive value to traditional risk factors of CAD in a binary logistic regression model for the prediction of angiographically significant CAD. This model confirmed the role of classic risk factors. Increasing age, hypertension, smoking and a high LDL/HDL ratio were confirmed as risk factors for CAD as well as female gender as a protective factor against CAD as generally accepted from several large previously published studies, such as the recent INTERHEART study.27 Our results also agree with the report of Wang et al that 10 contemporary biomarkers, including BNP and hs-CRP added only moderately to standard risk factors for assessing risk in individuals in a general population to develop major cardiovascular events and death.21
In conclusion, our results demonstrate that NT-proBNP is independently but only weakly associated with three-vessel CAD at angiography. In the clinical routine setting of our cross-sectional study NT-proBNP was of limited value as a screening test for predicting significant angiographic lesions. However, of all tested newer biochemical markers (NT-proBNP, hs-CRP, GGT) only NT-proBNP is a statistically significant independent predictor of CAD severity. Its predictive value as the most informative biochemical marker tested, however, is small compared with traditional risk factors and it is unlikely to become clinically important in this context as well.
REFERENCES
Footnotes
Funding: None.
Competing interests: None.