Article Text

Abstract
Objective To evaluate the predictive value of seven biomarkers, which individually have been shown to be independent predictors, for use in a combined multimarker model for long-term cardiovascular outcome after non-ST-segment elevation acute coronary syndrome (NSTEACS).
Design and Setting Levels of high-sensitivity C-reactive protein (hsCRP), myeloperoxidase, pregnancy-associated plasma protein A, placental growth factor (PlGF), soluble CD40 ligand (sCD40L), interleukin 10 (IL-10) and troponin-T (TnT) were determined in patients enrolled in the CAPTURE trial. Cox proportional hazard regression analyses were applied to evaluate the relation between biomarkers and the occurrence of all-cause mortality or non-fatal myocardial infarction (MI).
Patients 1090 patients with NSTEACS.
Main outcome measure All-cause mortality and non-fatal MI during a median follow-up of 4 years.
Results The composite endpoint was reached by 15.3% of patients. Admission levels of TnT >0.01 μg/l (adjusted HR 1.8), IL-10 <3.5 ng/l (1.7), myeloperoxidase >350 μg/l (1.5) and PlGF >27 ng/l (1.9) remained significant predictors for the incidence of all-cause mortality or non-fatal MI after multivariable adjustment for other biomarkers and clinical characteristics, whereas hsCRP, pregnancy-associated plasma protein A and sCD40L were only associated with the endpoint in univariate analysis. A multimarker model consisting of TnT, IL-10, myeloperoxidase and PlGF predicted 4-year event rates that varied between 6.0% (all markers normal) and 35.8% (three or more biomarkers abnormal).
Conclusion In patients with NSTEACS, biomarkers characterising distinct aspects of the underlying atherosclerotic process and myocardial damage of the initial cardiac event can assist in predicting long-term adverse cardiac outcomes. The use of combinations of selected biomarkers adds incremental predictive value to further risk stratification in an otherwise seemingly homogeneous NSTEACS population.
- Acute coronary syndrome
- biomarker
- inflammation
- multimarker risk prediction model
- risk stratification
Statistics from Altmetric.com
Atherosclerosis and plaque destabilisation leading to coronary thrombosis and an acute coronary syndrome (ACS) are the result of a very heterogeneous process, involving vascular inflammation, endothelial dysfunction and hypercoagulability.1 Several novel serum biomarkers are thought to reflect these pathophysiological constituents of coronary artery disease (CAD) and have also proved to be independent predictors of future coronary events. C-reactive protein is the most extensively studied biomarker in this respect. It has been shown to be useful not only as a prognostic tool in patients with ACS,2 but also in predicting the future risk of CAD in apparently healthy men and women.3 Myeloperoxidase, a leucocytic enzyme that appears as part of the host defence in inflammatory disorders, and also present in soft plaque, was associated with an increased risk of major adverse cardiac events in patients with documented ACS,2 as well as in those presenting with chest pain without evidence of myocardial necrosis.4 Also expressed in ruptured and eroded plaques, but not in stable plaques, is the metalloproteinase pregnancy-associated plasma protein A (PAPP-A).5 6 Placental growth factor (PlGF), a member of the vascular endothelial growth factor family, is considered a primary inflammatory instigator in atherosclerotic lesions,7 and has prognostic value in patients with ACS.8 In contrast, elevated levels of the anti-inflammatory cytokine interleukin 10 (IL-10) were associated with a lower risk of coronary events in patients with ACS and elevated high-sensitivity C-reactive protein (hsCRP) levels,9 emphasising the importance of an inflammatory balance in the vascular wall. Finally, elevated levels of soluble CD40 ligand (sCD40L), which is primarily released from activated platelets,10 were associated with an increased cardiovascular risk during 6 months of follow-up of ACS-patients.11
The prognostic value of these and other biomarkers for the risk of future cardiovascular events in ACS patients has previously been studied. These analyses typically assess each marker individually with adjustment for clinical patient characteristics.
In certain cases, two markers are combined in one model.12 There are only two reports, however, in which the specific combination of three biomarkers provided incremental value for risk prediction after ACS.13 14 Furthermore, the follow-up duration of previous multimarker studies in ACS patients was often limited to periods consisting of several months up to a maximum of 1 year after admission.2 5 8 9 11 13–15 Nevertheless, coronary pathophysiology is sustained after acute interventional or pharmacological treatment and continuously triggers cardiovascular events during long-term follow-up. We therefore studied the relation between baseline levels of seven biomarkers, including troponin-T (TnT) as a marker of myocardial necrosis, both independently and in a combined multimarker risk model, and the incidence of all-cause mortality or non-fatal myocardial infarction (MI) during an extended 4-year follow-up period in ACS patients who were enrolled in the CAPTURE trial.
Methods
Patients and treatment
Patients admitted with unstable angina pectoris or non ST-elevation MI were eligible for CAPTURE if they had refractory unstable angina defined as: chest pain at rest with concomitant ECG abnormalities compatible with myocardial ischaemia (ST-segment depression, ST-segment elevation, or abnormal T waves) and one or more episodes of typical chest pain, ECG abnormalities, or both, compatible with myocardial ischaemia during therapy with intravenous heparin and nitrates, started at least 2 h previously. The latest episode of ischaemia should have occurred within the 48 h before enrolment, corresponding to Braunwald class III unstable angina. All patients had undergone angiography and had significant CAD, with a culprit lesion suitable for percutaneous coronary intervention (PCI). Patients were enrolled within 24 h of coronary angiography and were randomly assigned to abciximab (ReoPro, Centocor BV, Leiden, The Netherlands; 0.25 mg/kg bolus plus 10 μg/min continuous infusion) or placebo after providing written informed consent. PCI was scheduled 18–24 h after the start of study medication. Study medication was started within 2 h of randomisation and continued until 1 h after the procedure. All patients received aspirin, heparin and nitrates, whereas β-blockers, calcium channel antagonists and other cardiovascular drugs were given at the discretion of the investigator.
Analytical techniques
Blood samples were drawn 8.7±4.9 h after the last episode of angina, but before PCI and before the incidence of adverse events. Serum and heparin plasma samples were available for the measurement of TnT, hsCRP, sCD40L, IL-10, myeloperoxidase, PAPP-A and PlGF levels. Biomarker measurements were performed blinded to the patients' histories. Levels of sCD40L, high-sensitivity IL-10, myeloperoxidase and PlGF were measured by ELISA (sCD40L, IL-10 and PlGF from R&D Systems, Wiesbaden, Germany and myeloperoxidase from Calbiochem, Merck KGaA, Darmstadt, Germany). Diagnostic thresholds were 5.0 μg/l for sCD40L, 3.5 ng/l for IL-10, 350 μg/l for myeloperoxidase and 27 ng/l for PlGF. Levels of TnT and PAPP-A were determined using a electrochemiluminescence immunoassay (Elecsys, Roche Diagnostics, Mannheim, Germany). A diagnostic threshold value of 0.01 μg/l for TnT and 12.6 mIU/l for PAPP-A was used. Levels of hsCRP were measured using the Behring BN II Nephelometer (Dade Behring, Deerfield, Illinois, USA). A diagnostic threshold value of 10 mg/l was used. All cut-off values were consistent with previous biomarker publications within this cohort in which the markers were described independently.2 5 8 9 11 15
Study endpoints
The endpoint of the present analysis was a composite of all-cause mortality and non-fatal MI during 4-year (median) follow-up. Follow-up at 6 months was part of the initial study protocol, and a clinical endpoint committee adjudicated these events.
MI during the index hospital stay was defined as values of creatine kinase or its myocardial type (MB) isoenzyme more than three times the upper limit of normal in at least two samples, with an increase by 50% over the previous value, or an ECG with new significant Q waves in two or more contiguous leads. MI after discharge was defined as concentrations of creatine kinase or its myocardial type isoenzyme above two times the upper limit of normal, or new significant Q waves in two or more contiguous ECG leads. Survival status and information on MI during extended follow-up (ie, after 6 months after randomisation) were obtained from the treating physician, the general practitioner, through self-reporting or municipal registries. These events were not adjudicated.
Data analysis
Continuous variables were summarised by median values with corresponding 25th and 75th percentiles. Discrete variables were summarised in terms of frequencies and percentages. Kaplan–Meier analyses were performed to evaluate the incidence of events over time. Univariable and multivariable Cox proportional hazards regression analyses were applied to evaluate the relation between all biomarkers and long-term outcome. In the multivariate model we adjusted variables known to be important predictors of outcome including age, gender, smoking, diabetes mellitus, hypertension, hypercholesterolaemia, left ventricular ejection fraction, ST-depression, ST-elevation or T-wave changes on the admittance ECG and history of MI, peripheral vascular disease, chronic heart failure or previous PCI. Crude and adjusted HR are presented with 95% CI. p Values were two-sided, with p≤0.05 being considered significant.
In case patients had more than one event (MI or death), the first was counted. In previous analyses of the CAPTURE study, significant interactions were observed between certain biomarkers (TnT and sCD40L) and allocated treatment with respect to the incidence of cardiovascular events during 6-month follow-up.11 15 Formal statistical tests demonstrated that these interactions were no longer present with respect to the incidence of such events during long-term follow-up. Therefore, we decided to conduct all analyses on the patients allocated to placebo (N=544), as well as on the entire study population (placebo and abciximab combined; N=1090). The results of both sets of analyses are presented.
Results
One thousand two hundred and sixty-five patients were enrolled in the CAPTURE trial. Multiple biomarker analysis proved feasible in 1090 patients. Baseline characteristics and clinical variables of these 1090 patients (546 abciximab, 544 placebo) who were included in our analyses are provided in table 1. The median follow-up duration was 47 months (25th and 75th percentile: 38, 55). The composite endpoint was reached in 167 (15.3%) patients (58 deaths and 109 non-fatal MIs).
Baseline characteristics
Patients with elevated levels of most of the studied biomarkers had a higher risk of death or non-fatal MI than those with levels below the threshold (figure 1 and table 2), whereas elevated levels of IL-10 were associated with a better prognosis. For example, in the entire study population, those with TnT levels greater than 0.01 μg/l had a 20.3% incidence of death or non-fatal MI at 4 years of follow-up versus 11.1% in those with low TnT levels (unadjusted HR 2.1 and 95% CI 1.4 to 3.0). In patients receiving placebo, 4-year event rates were 23.5% and 11.6% in those with and without elevated TnT, respectively (unadjusted HR 2.2 and 95% CI 1.3 to 3.6; table 2). The results for all (other) biomarkers are given in table 2.

Kaplan–Meier curves for each independent biomarker. Kaplan–Meier curves of the composite endpoint of all-cause mortality or non-fatal myocardial infarction during 4-year follow-up according to levels of different markers for placebo patients (left panels) and the entire study population (right panels). TnT, troponin-T (bold line indicates TnT >0.01 μg/l); hsCRP, high-sensitivity CRP (bold line is >10.0 mg/l); IL-10, interleukin 10 (bold line is ≥3.5 ng/l); MPO, myeloperoxidase (bold line is >350 μg/l); PAPP-A, pregnancy associated plasma protein A (bold line is >12.6 mIU/l); PlGF, placental growth factor (bold line is >27 ng/l); sCD40L, soluble CD40 ligand (bold line is >5.0 μg/l). The x-axis are days of follow-up.
Relation between biomarkers of vascular inflammation, myocardial necrosis, platelet activation and a composite of all-cause mortality and non-fatal MI during 4-year follow-up
TnT, IL-10, myeloperoxidase and PlGF remained significant predictors for the incidence of all-cause mortality or non-fatal MI in the entire study population as well as in patients receiving placebo (table 2) after multivariable adjustment for clinical characteristics and all other biomarkers, whereas hsCRP, sCD40L and PAPP-A did not. Only two of the baseline clinical variables remained significant: age and ejection fraction (HR 1.03; 95% CI 1.01 to 1.04 per year and HR 0.98; 95% CI 0.96 to 0.99 per percentage point increase in ejection fraction, respectively; not given in table 2) in a multivariate model that included all biomarkers and baseline clinical variables.
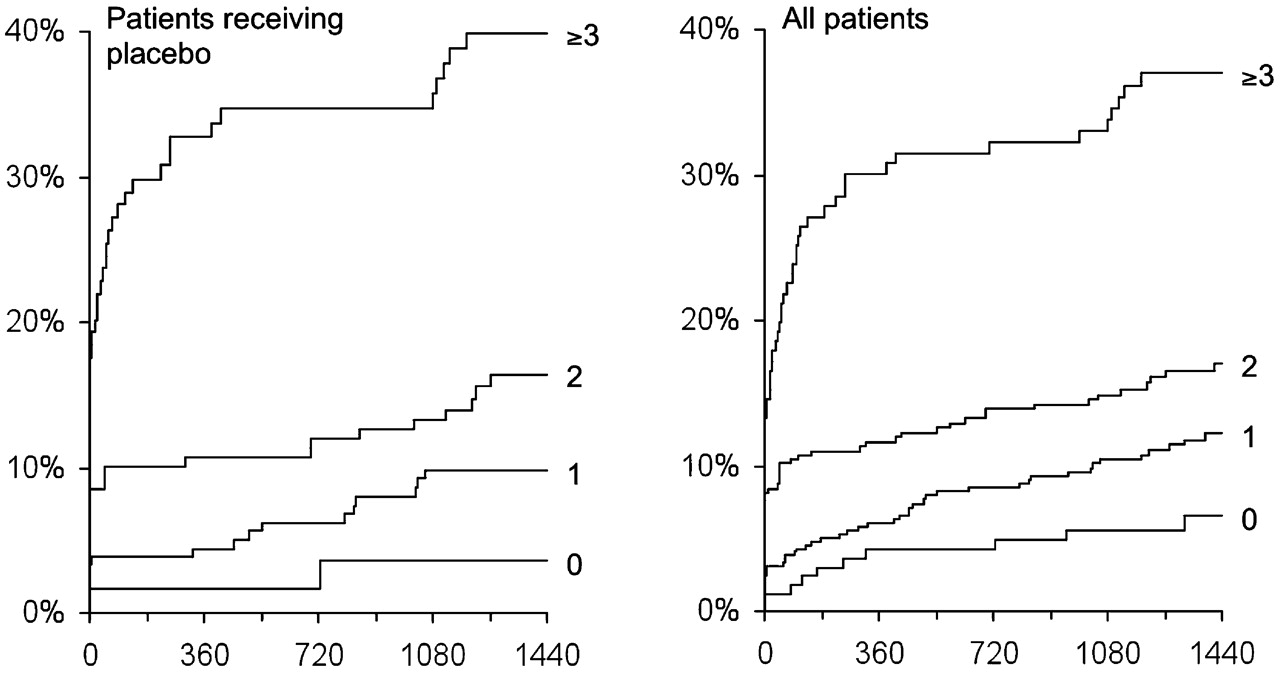
We created a simple risk model for 4-year mortality and non-fatal MI by counting the presence or absence of an abnormal biomarker value that significantly predicted risk for an event. The percentages of patients with none, one, two or three or more abnormal biomarker levels were 5.2%, 22.1%, 43.5% and 29.2%, respectively. Four-year event rates varied between 6.0% (all markers normal) and 35.8% (three or more biomarkers abnormal) in all patients, and between 3.3% and 38.6% in those receiving placebo (figures 2 and 3).

Multimarker risk score. Multimarker risk score with separate risks for all-cause mortality (black squares) and non-fatal myocardial infarction (white squares) in patients treated with placebo (left panel) and in the entire study population (right panel) at 4 years of follow-up after counting the absence or presence of one, two, or three or more biomarkers above the threshold levels. The markers used are: troponin-T (TnT), interleukin 10 (IL-10), myeloperoxidase (MPO), placental growth factor (PlGF).

{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier analysis for the multimarker model. Kaplan–Meier curves of all-cause mortality or non-fatal myocardial infarction during 4-year follow-up for patients treated with placebo (left panel) and the entire study population (right panel) with none, one, two, or three or more biomarkers above the threshold levels. The markers used here are: troponin-T, interleukin 10, myeloperoxidase and placental growth factor.
Discussion
The present study is the first to report a long-term post-ACS multimarker risk prediction model for which biomarkers are selected on the basis of adjustment for baseline clinical patient characteristics as well as adjustment for all other analysed biomarkers. The results add to the growing body of evidence that novel biomarkers reflecting atherosclerotic burden or disease activity independently predict the long-term risk of death and non-fatal infarction in patients with an ACS. Elevated baseline levels of placental growth factor, myeloperoxidase and low levels of the anti-inflammatory cytokine IL-10 were independently associated with adverse long-term outcomes in patients with non-ST-segment elevation acute coronary syndrome (NSTEACS). These findings support the pathophysiological concept of a chronic (vascular) inflammatory basis of atherosclerosis,16–18 with an acute superimposed process in the setting of an ACS.1 The present data indirectly suggest that elevated biomarkers at baseline reflect a chronic inflammatory process in the coronary vessel wall that may indeed result in repetitive occurrences of cardiovascular events during long-term follow-up. The predictive value of the selected inflammatory markers was independent of baseline clinical patient characteristics and index diagnosis experienced during the initial incident (correction for unstable angina or non ST-elevation MI took place by adding TnT as a covariate in all our multivariate analysis). Moreover, multivariate analysis in a model including all biomarkers and baseline clinical patient characteristics proved that four out of seven biomarkers, but only two out of 14 baseline clinical patient characteristics (as described in table 2) remained significantly associated with the endpoint. The incremental value of novel biomarkers as risk predictors over traditional patient characteristics was previously described in another large cohort of non ST-elevation ACS patients in the GUSTO IV trial.12 Our data might suggest that biomarkers improve risk prediction through their proposed capability to reflect disease biology, instead of mere patient characteristics. Accordingly, a combination of multiple biomarkers, which reflect different pathophysiological components of CAD, might aggregate risk prediction properties. The risk of death or non-fatal MI was calculated in this same line of thought using a simple risk stratification model by counting the number of markers outside the normal range. We investigated the role of myocardial necrosis (TnT) together with oxidative stress (myeloperoxidase), and chronic background vascular inflammation (PlGF and IL-10) for the development of a future cardiovascular event. As there was indeed an important increase in risk if patients showed an increasing number of abnormal biomarker values (figures 2 and 3), this simple stratification might aid to adjust and intensify treatment in such patients with a detrimental biomarker profile. A more aggressive therapeutic strategy, for instance, might prove to be useful not only in treating the current acute event, but also to prevent later events. In the future, this strategy might even include a more specific anti-inflammatory treatment such as blocking of the PlGF receptor or reducing the activity of circulating PlGF levels by the administration of soluble vascular endothelial growth factor receptor 1.19
Multimarker strategies also provide a window of opportunity for the selection of candidate biomarkers for risk stratification. Previous studies of the same patient cohort reported that, after multivariate adjustment only for baseline clinical patient variables, hsCRP,2 sCD40L11 and PAPP-A5 remained independent risk predictors of adverse cardiac events at 6 months follow-up. In this 4-year analysis, however, we observed that hsCRP, sCD40L and PAPP-A were significant predictors in univariate analysis, but lost significance after correction for other biomarkers, suggesting that the remaining biomarkers might be better post-ACS predictors for long-term risk. This is remarkable, particularly for hsCRP as this marker has been the focus of extensive research and has been suggested as the most likely candidate for clinical application.20 21 Obviously, the selection of valuable candidate biomarkers for risk prediction of future coronary events on the basis of a single biomarker as well as in the setting of a multimarker model requires further elucidation. Preferably, future research will also clarify the appropriate cut-off values and the actual prediction windows of novel biomarkers across different patient groups.
Previous studies have shown an interaction between allocated treatment and levels of biomarkers for short-term follow-up.11–15 Although formal testing did not show a significant interaction between the biomarkers and treatment with abciximab with respect to long-term event rates, we performed separate analyses for the placebo group and the entire study population. As the obtained data consistently indicate that TnT, IL-10, myeloperoxidase and PlGF are independent predictors for long-term outcome, we conclude that our findings have general applicability if confirmed in other trials including more heterogeneous study populations of patients with atherosclerosis and ischaemic coronary syndromes.
We acknowledge that this investigation has some limitations. First, the long-term follow-up data that were obtained from multiple sources were not adjudicated by an independent clinical event committee. The applied criteria for MI might thus have differed between investigators, and some events may actually have been missed. Second, no information is available on long-term medical treatment such as statin therapy or ACE inhibition22 23 with their suggested anti-inflammatory effects, which might have influenced patient outcomes. However, it is unlikely that this has resulted in a differential bias between patients with or without elevated biomarker levels. In this respect, it should be emphasised that the investigators who collected long-term follow-up data (EB, TL) were blinded for any information on baseline data (including biomarker levels).
When using such a simple risk model with dichotomised biomarker data, quantitative information might be lost as higher levels for one or another biomarker could correspond with different individual risk. However, by using simple cut-off values, physicians might be able to calculate the patients' risk more easily. With the help of this model in conjunction with the careful selection of other biomarkers and clinical variables, we might be able to provide tailored treatment for the individual patient not only at the time of hospitalisation but also following discharge. The threshold levels of the markers are based on exploratory analyses illustrated in previous publications. Naturally, if possible, prospective validation should be performed. Finally, it remains to be determined whether assessment of these biomarkers at discharge, or at even later time points in stabilised patients, might demonstrate an even closer relationship between abnormal biomarker levels and the risk of future cardiovascular events.
Certain biomarkers have specific evolutionary patterns during admission for ACS24 and thus the role of the exact timing of the biomarker measurements should be emphasised. In our study, blood samples were drawn at admission, on average 9 h after the last episode of angina. Its results should therefore not be extrapolated to biomarker measurements at other time points, for example, at discharge, when the same biomarkers (at the same cut-off levels) theoretically might demonstrate a different predictive value. Although new troponin elevations are seldom found after the first 6–9 h,25 the possibility exists that some patients who were classified ‘troponin-negative’ in fact would prove to have elevated levels of circulating troponin in case of measurement at later time points. As troponin elevations are related to a worse prognosis, this type of potential unidirectional misclassification might have led to an underestimation of the relation between troponin elevation and adverse outcomes in our analyses.
Conclusion
In patients with NSTEACS, biomarkers reflecting distinct aspects of the underlying atherosclerotic process, and myocardial damage of the initial cardiac event can assist in predicting long-term adverse cardiac outcomes. The use of combinations of selected biomarkers adds incremental predictive value to further risk stratification in an otherwise seemingly homogeneous NSTEACS population.
References
Footnotes
Funding RMO is supported by a non-commercial grant from The Netherlands Heart Foundation (NHS2007B012) and the Interuniversity Cardiology Institute Netherlands (07101), both of which have been received by EB. The funding source of the CAPTURE trial, Centocor (Leiden, The Netherlands) had no participating role in any form in the current biomarker analyses.
Competing interests None.
Ethics approval This is a biomarker analysis in samples that derive from a multicentre randomised controlled trial for which ethics committee approval was obtained at both the national and local hospital levels.
Provenance and peer review Not commissioned; externally peer reviewed.