Article Text

Abstract
Objective Studies on the association between short-term exposure to ambient air pollution and heart rate variability (HRV) suggest that particulate matter (PM) exposure is associated with reductions in measures of HRV, but there is heterogeneity in the nature and magnitude of this association between studies. The authors performed a meta-analysis to determine how consistent this association is.
Data source The authors searched the Pubmed citation database and Web of Knowledge to identify studies on HRV and PM.
Study selection Of the epidemiologic studies reviewed, 29 provided sufficient details to be considered. The meta-analysis included 18667 subjects recruited from the population in surveys, studies from patient groups, and from occupationally exposed groups.
Data extraction Two investigators read all papers and computerised all relevant information.
Results The authors computed pooled estimates from a random-effects model. In the combined studies, an increase of 10 μg/m3 in PM2.5 was associated with significant reductions in the time-domain measurements, including low frequency (−1.66%, 95% CI −2.58% to −0.74%) and high frequency (−2.44%, 95% CI −3.76% to −1.12%) and in frequency-domain measurements, for SDNN (−0.12%, 95% CI −0.22% to −0.03%) and for rMSSD (−2.18%, 95% CI −3.33% to −1.03%). Funnel plots suggested that no publication bias was present and a sensitivity analysis confirmed the robustness of our combined estimates.
Conclusion The meta-analysis supports an inverse relationship between HRV, a marker for a worse cardiovascular prognosis, and particulate air pollution.
- Heart rate variability
- air pollution
- meta-analysis
- cardiac function
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Introduction
A recent scientific report from the American Heart Association concluded that particulate matter (PM) is a modifiable risk factor contributing to cardiovascular morbidity and mortality.1 We provided a novel insight that particulate air pollution is a relevant trigger for myocardial infarction at the community level.2–4 Altered cardiac autonomic function as measured by heart rate variability (HRV) is considered to be one of the pathophysiological pathways through which PM air pollution influences the cardiovascular system.5 ,6 Reduced HRV has been associated with an increased risk of myocardial infarction among the population7 and has been considered as a predictor of increased risk of mortality in patients with heart failure.8 The importance of this pathway is still under debate.9 ,10 Here we determine whether all the available observational data up to February 2012 support a positive association and how strong such a relationship between HRV and particulate air pollution may be.
Methods
Data collection
We followed published guidelines for the reporting of this meta-analysis.11 A systematic literature search of PubMed and Web of Knowledge, last accessed on 15 February 2012, was conducted to identify studies of HRV and air pollution published in English. In addition, we screened the reference list of all identified relevant publications and review articles found during our literature search. Two search terms were combined using the Boolean operator AND. The first term, air pollution, combined exploded versions of the Medical Subject Headings air pollution, particulate matter and air pollutants. The second term was heart rate variability.
Study selection
Two investigators (NP and MP) read all papers and extracted and computerised the relevant information independently (table 1). Reviews, case-reports, pilot studies, animal studies, manuscripts not written in English and studies that reported another association were excluded. Out of 509 initially selected articles, 98 studies reported an association between HRV and air pollution. If a group published two or more papers based on the same study population (n=31), only that publication providing the most detailed information was included. We selected only studies that used particulate matter with aerodynamic diameter of 10 μm or less (PM10) or 2.5 μm or less (PM2.5) as indicators of air pollution. Studies were also excluded when a controlled exposure was used. Where applicable, preference was given to results adjusted for age and heart rate and additional factors of proven importance.40 Quality assessment of the selected studies was performed with consideration of the following aspects: study design, response rate, information about responders versus non-responders, sample size, statistical methods, correction for meteorological conditions and personal or local PM assessment (supplementary data).
Characteristics of the studies included in the meta-analysis
Statistical analysis
HRV was evaluated using different time-domain and frequency-domain measures, according to the measurements presented in the included studies. The time-domain measures include rMSSD, the square root of the mean squared difference of successive normal to normal intervals, and SDNN, the SD of the normal to normal intervals. Two spectral components were distinguished in the frequency-domain measurements: low frequency (LF) power and high frequency (HF) power. Many time- and frequency-domain variables measured over a 24-h ECG recording are strongly correlated with each other.41 We obtained a meta-analytical effect estimate using random-effects models, because the Cochran Q-statistics showed evidence of heterogeneity greater than expected by the sampling variance alone (p<0.1). An effect estimate was derived from the point estimate of each separate study weighted by the inverse of the variance (1/SE2). When we had independent subgroups within a study, each subgroup was treated as a separate study. The effect size was calculated as a per cent change for an exposure increment of 10 μg/m3 in PM2.5. The per cent change was calculated as (10^β−1)×100% with 95% CIs ((10^(β±1.96×SE))−1)×100%, where 10x is the antilog, β is the estimated regression coefficient and SE is the SE of β, when HRV was log-transformed. The formula (1−(Average-β)/Average)×100% was used when there was no transformation. When data for only PM10 were available,6 ,13 ,30 ,32 we converted the per cent change with the assumption that PM10 consists of 70% of PM2.5.2 ,42 However, other conversions were considered in sensitivity analysis to determine what the effect would be on the overall estimate, supposing PM10 consists of 60% or 80% of PM2.5.2 All calculations were independently performed by two researchers (NP and MP).
Sensitivity of the findings was examined by performing the analysis both with and without the occupational studies.16 ,20 ,37 The analysis was repeated separately for long-term (more than 18 h of analysable ECG recordings) and short-term (<1 h of analysable ECG recordings) ECG recordings. Three studies26 ,27 ,37 could not be classified according to this distinction and were excluded from the short- and long-term analyses. We determined whether there was a difference in the combined effect size when only studies with a high quality score were included. We also tested the difference between a 24-h exposure and 48-h exposure on the HRV. Since both 24 h and 48 h measurements were used in some of these studies13 ,21 ,25 ,28 ,30, the effect size for the 48 h exposure, used in the sensitivity analysis, differed from the data given in table 1, figures 1 and 2. Further, we evaluated the influence of individual studies on pooled effect sizes by excluding one study at the time. If the point estimate of the combined effect size with one study omitted lies outside the CI of the overall estimate, the study in question has an excessive influence. We plotted the association size against the SE of the study. If there is no publication bias, such a plot must produce a funnel shape (funnel plot), because the points scatter around the true pooled value with the scattering narrowing as the sample size increases. All p values are two-sided tests.
A meta-regression was performed to investigate the effect of study design (longitudinal vs cross-sectional), mean age, mean PM2.5 concentration, scale of HRV (log vs linear), percentage of men, year of publication and length of analysed ECG recordings on the combined effect of PM2.5 on HRV.
Results
Selection of studies
Of the studies reviewed 480 reports were excluded; 128 were duplicates, 174 were excluded based on screening the abstract, 24 studies were reviews, 57 studies reported on animal data, one study was a pilot-study, four publications were not written in English, one study was a case report, 20 studies reported another association than PM and HRV, 19 studies with an estimated exposure from other measurements than the particulate air pollution (PM10 or PM2.5), two did not provide sufficient information to compute the association size, 17 were experimental studies, 31 used the same study population as reports included in the analysis and two studies used PM measurements longer than 24 h (supplementary data). As a result, we identified 29 studies, comprising 18 667 persons, which investigated the association between HRV and PM. This selection includes 25 longitudinal studies,6 ,12–17 19–29 31–33 35–39 including one exploratory study15 and three occupational studies16 ,20 ,37 and four cross-sectional designs.18 ,21 ,30 ,34 These are listed in chronological order in table 1.
Characteristics of studies
All studies had a time window of PM measurements ranging from 2 h up to 1 day before HRV measurements. The length of ECG recordings varied from 10 s to 24 h. Whenever possible, preference was given to long-term ECG recordings (more than 18 h of analysable ECG recordings). The HRV measurements were expressed on a logarithmic scale in 23 studies6 ,12 ,16–19 21–30 32–37 ,39 and on a linear scale in five studies.13–15 ,20 ,31 One publication used both a linear and logarithmic scale.38
Only one study calculated the association between PM exposure and HRV without reporting possible confounders.15 One study included potential confounders but did not report them.20 In all but four reports19 ,25 ,31 ,35 the results were adjusted for age. Eleven publications did not adjust for sex.16 ,21 ,32 ,35 However, in four16 ,21 ,32 ,35 of these 11 reports, all subjects had the same sex. Most studies also considered additional confounding variables, such as heart rate,13 ,16–19 ,22 ,33 ,37 ,39 BMI,14 ,18 ,21 ,26 ,28 ,29 ,32 ,34–36 ,39 outdoor temperature,14 ,18 ,19 ,21–34 36–39 relative humidity,14 ,18–21 23–31 ,33 ,34 ,36–39 ethnicity14 ,18 ,24 ,32–34 ,38 and (past) smoking.16 ,18 ,21 ,30–35
Summary statistics
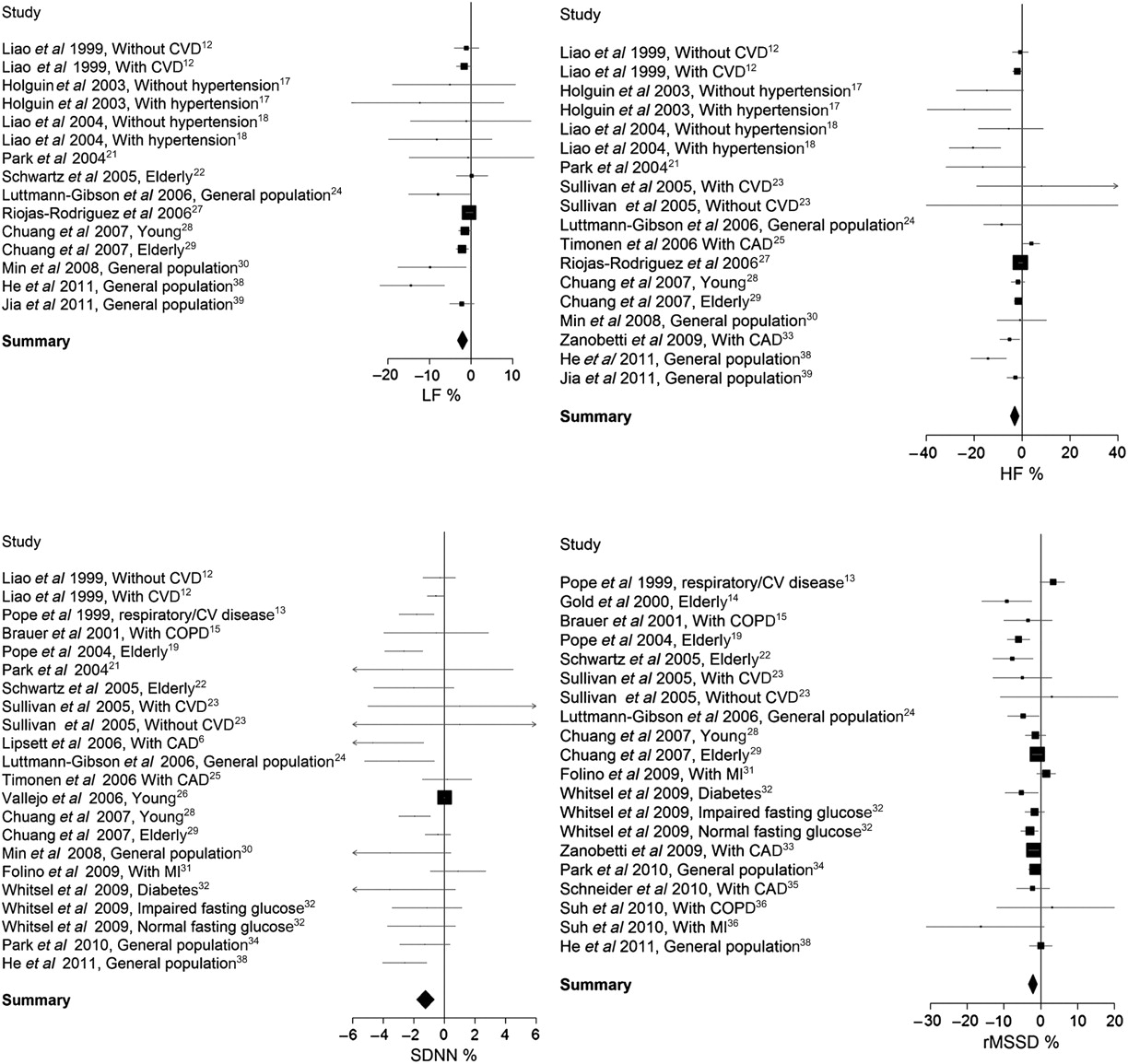
We evaluated HRV using both frequency- and time-domain measurements. The combined estimates calculated for a 10 μg/m3 increase in PM2.5 showed a decrease of 1.66% (95% CI −2.58% to −0.74%) and 2.44% (95% CI −3.76% to −1.12%) for LF and HF, respectively. The corresponding estimates for the time-domain measurements were −0.12% (95% CI −0.22% to −0.03%) for SDNN and −2.18% (95% CI −3.33% to −1.03%) in rMSSD (figure 1).

Forests plots of change in parameter (95% CI) of heart rate variability associated with a 10 μg/m3 increase in PM2.5 with inclusion of occupational studies. Squares represent individual groups. The area of each square is proportional to the inverse of the variance. HF, high frequency; LF, low frequency; PM2.5, particulate matter with aerodynamic diameter of 2.5 μm or less; rMSSD, square root of the mean squared difference of successive normal to normal intervals; SDNN, SD of normal to normal intervals.
Sensitivity analysis
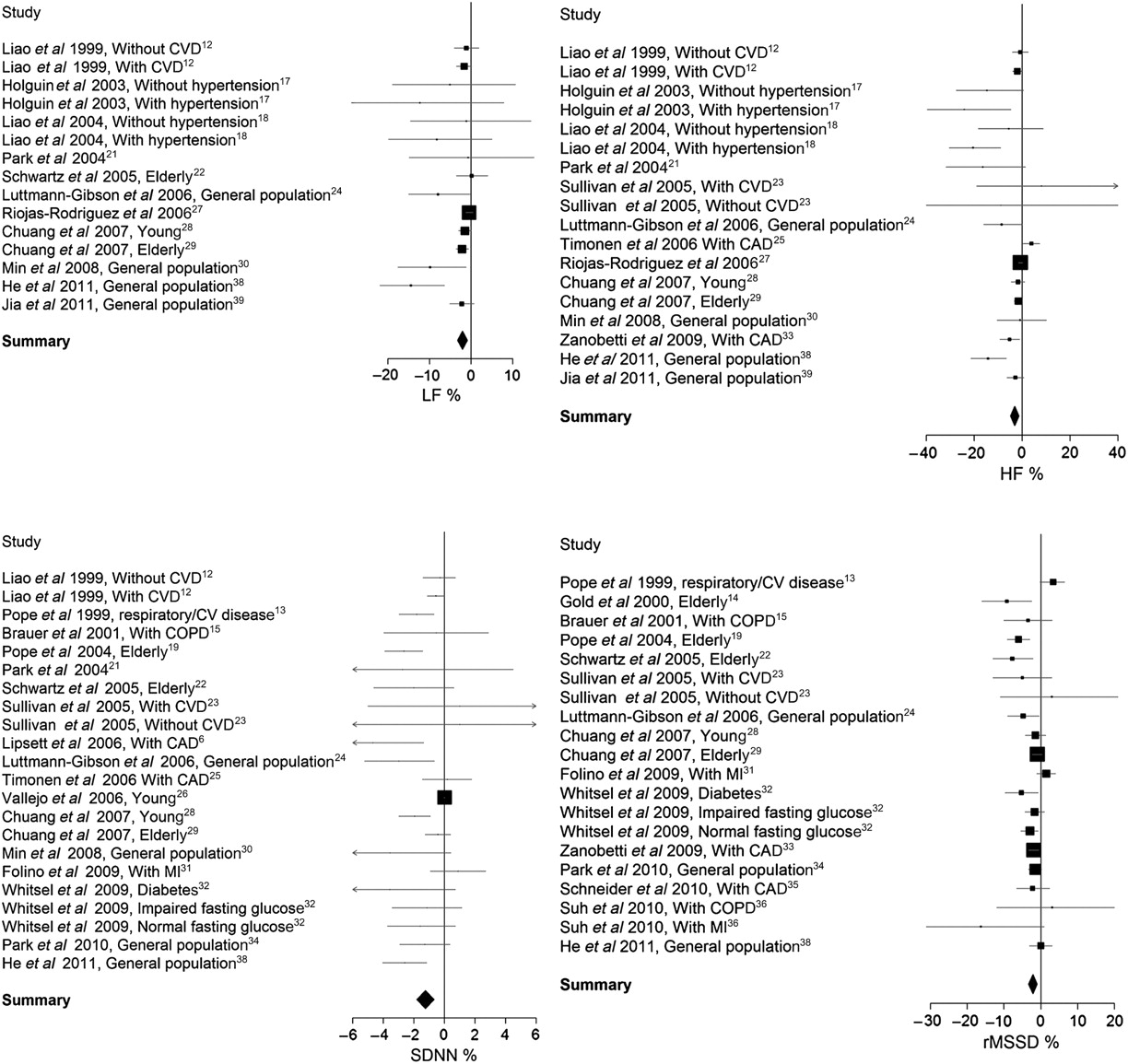
When the analysis was repeated without three occupational studies,16 ,20 ,37 we found a minor difference in LF, −2.05% (95% CI −3.21% to −0.88%) and HF, −3.17% (95% CI −4.92% to −1.41%) for a 10 μg/m3 increase in PM2.5 (figure 2). However, the effect of exclusion of these three studies was much larger for SDNN, which results in a combined effect of −1.25% (95% CI −1.81% to −0.68%).
{kind=link}
{kind=link}
Change in parameter (95% CI) of heart rate variability associated with a 10 μg/m3 increase in PM2.5 without inclusion of occupational studies. Squares represent individual groups. The area of each square is proportional to the inverse of the variance. HF, high frequency; LF, low frequency; PM2.5, particulate matter with aerodynamic diameter of 2.5 μm or less; rMSSD, square root of the mean squared difference of successive normal to normal intervals; SDNN, SD of normal to normal intervals.
For LF and HF the majority of studies, 75% and 71% respectively, used short-term ECG recordings. When removing the studies with long-term ECG recordings,29 ,33 ,38 ,39 we found a decrease of 1.73% (95% CI −2% to −0.4%) and 1.75% (95% CI −3.2% to −0.29%) for LF and HF, respectively. When repeating the analysis separately for short-term12 ,20–25 ,28 ,30 ,32 ,34 and long-term6 ,13 ,15 ,16 ,19 ,29 ,31 ,38 recordings for SDNN, we observed a decrease in short-term and long-term recordings of −0.73% (95% CI −1.17% to −0.29%) and −1.39% (95% CI −2.37% to −0.41%), respectively. When including only short-term14 ,22–24 ,28 ,32 ,34 ,36 recordings for rMSSD, we still found a decrease of 3.21 (95% CI −4.66% to −1.76%) for a 10 μg/m3 increase PM2.5. However, when including only the long-term13 ,15 ,19 ,31 ,33 ,35 ,38 recordings of seven studies, no statistically significant association was found (p=21) between rMSSD and PM2.5. Excluding specific groups of patients suffering from cardiovascular diseases6 ,12 ,13 ,23 ,25 ,31 ,33 ,35 ,36 from the analysis resulted in a similar combined effect estimate (table 2). The sensitivity analysis was also performed with only studies with a high quality score (more than the median score). The decrease was more pronounced for LF (−2.49%, 95% CI −4.32% to −0.36%) and HF (−5.74%, 95% CI −8.82% to −2.66%), similar for rMSSD (−1.89%, 95% CI −3.08 to −0.71%) but was no longer significant for SDNN (−0.05%, 95% CI −0.13% to 0.02%). When determining the effect of a 48-h exposure, we found a similar decrease in LF, HF and SDNN.
Sensitivity analysis
Also, when four studies18 ,21 ,30 ,34 with a cross-sectional design were excluded the combined effect estimate was comparable (table 2). When studies with PM10 measurements were excluded from the analysis, the results were similar for all HRV parameters (table 2). The sensitivity of the findings was further examined by removing one study at a time from the analysis and recalculating the combined effect (supplementary data). For SDNN, we identified two studies16 ,26 that moved the point estimate outside the CI for the overall estimate with all available studies, including the occupational studies. Recalculating the per cent change, supposing that PM10 consists of 60% or 80% of PM2.5, to determine what the effect would be on the overall estimate did not have a significant influence on the overall estimate (data not shown).
Publication bias
The funnel plots searching for publication bias (supplementary data) did not reveal a deficit of small studies with negative results. Meta-regression revealed that study design (longitudinal vs cross-sectional), mean age, mean PM2.5 concentration, scale of HRV (log vs linear), percentage of men, year of publication and length of analysed ECG did not have a significant influence on the combined estimates; with exception for LF domain, the effects tended to be less strong in logarithmic studies (p=0.05) and stronger in studies with more men (p=0.04). For HF, the effects tended to be less strong for younger persons (p=0.03).
Discussion
The key finding of the present meta-analysis was that HRV by means of SDNN, rMSSD, HF and LF was decreased after an elevation in exposure to particulate air pollution (PM2.5) of 10 μg/m3. These effects were calculated using 29 studies that met the inclusion criteria comprising 18 667 study participants. We did not observe statistical evidence that the combined effect estimates were largely driven by the three occupational studies.
A reduced HRV is a powerful and independent predictor of adverse prognosis in patients with heart disease43–45 and in the general population.46 ,47 It is a marker of cardiac autonomic dysfunction and a predictor of sudden cardiac death and arrhythmias.8 A reduction of HRV has been reported in several cardiological and non-cardiological diseases such as myocardial infarction, diabetic neuropathy, cardiac transplantation, myocardial dysfunction and tetraplegia.8 HRV measurements are also promising as risk markers for fatigue,48 ageing49 and stress-situations.50 Despite the important prognostic power of HRV, it is still not a widely used tool in diagnostic settings, and agreed normative values for HRV remain missing.51 In terms of clinical significance the association between decreasing HRV with increasing air pollution is still under debate as the decrease in HRV can be a marker of cardiac disease or the cause of increased risk. The underlying mechanisms responsible for the association between fine PM exposure and impaired HRV are not yet fully understood. Substantial epidemiological literature links cardiovascular mortality and morbidity to exposures of ambient air pollution.52 ,53 Two main candidate mechanisms are release of pro-thrombotic and inflammatory cytokines from the lung, and effects on the electrical activity and autonomic function of the heart.54 HRV is indicative for the physiological responses of the autonomic nervous system, of the combined sympathetic and parasympathetic activity. Alterations in autonomic control of the heart, as represented by HRV, may represent a major pathophysiological mechanism by which air pollution leads to cardiac mortality.55 Two possible pathways can lead to changes in neural control of the heart affecting HRV by exposure to PM.55 Inhaled particles can promote a systemic sympathetic stress response that leads to decreased HRV measurements and may cumulate in ventricular tachyarrhythmia. On the other hand, the inhaled particles can stimulate irritant receptors in the lung parenchyma and respiratory airways, which leads to the opposite, an increased parasympathetic vagal response and increased HRV.55 Our combined estimate showed a decrease in all HRV parameters, which suggests an overall sympathetic response. The combined effect was most pronounced for HF, which is highly correlated with rMSSD.13 They both reflect parasympathetic cardial vagal tone. A decrease in SDNN, an overall measure of changes in autonomic tone, also implies an increased risk of cardiac morbidity and mortality.
Dietrich et al56 measured the effect of ETS on HRV through 24-h ECG recordings in 1218 non-smokers aged ≥50 years. Individuals who were passively exposed to environmental tobacco smoke at home or at work for more than 2 h/day had a decrease of 3.5% in SDNN, 0.14% in HF and 15.35% in LF. Compared with our meta-analytical estimates on HRV and PM2.5, the effects of passive smoking were more pronounced for SDNN and LF as these effects were −0.12% and −1.66% for a 10 μg/m3 increase in PM2.5. For HF, the effect for PM was more pronounced; we found an effect of −2.44%. We should be aware that PM exposure is a continuous variable and the expression for a 10 μg/m3 increase is a relatively small increase, as a difference of 30 μg/m3 in acute exposure is still within the range of daily variation in many parts of the world.2
Since air particulates can provoke oxidative stress and an inflammatory response in the lung and heart,57 oxidative stress is a potentially important cellular mechanism. A study by Schwartz et al58 concluded that the effects of PM2.5 on HF seemed to be mediated by reactive oxygen. The Normative Aging Study has shown a strong effect modification of the PM and HRV relationship by obesity and genes that modulate endogenous oxidative stress or xenobiotic metabolism, such as glutathione S-transferase M1, methylenetetrahydrofolate reductase and the haemochromatosis gene.58–60 Additional findings suggest protective effects of statins, dietary antioxidants and B vitamins, as well as ω-3 polyunsaturated fatty acids.58 ,59 ,61 ,62 These findings imply that pathways that decrease endogenous oxidative stress have a protective effect that alleviates reductions in HRV due to exposure of particulate air pollution. An alternative potential mechanism is provided by Schulz et al63 who found that an altered ion-channel function triggered by air pollution in myocardial cells can lead to cardiac malfunction.
Observational studies as included in our meta-analysis do not prove causation. However, repeated observation of an association in different populations and different subgroups showing the same or similar results suggest that the results of a single study are not due to coincidence. Our forest plots showed that the majority of studies showed a decrease in parameters of HRV in association with particulate air pollution. We showed consistent results between different study designs including cross-sectional studies, panel and repeated measure studies, which support a causal association. Furthermore, we observed heterogeneity between studies but our estimates were robust. Although in general the average concentration of occupational PM2.5 exposure was much higher than environmental exposure, exclusion of three occupational studies16 ,20 ,37 did not alter the combined estimate.
Although most studies report negative associations between time- or frequency-domain parameters of HRV and particulate air pollution, the magnitudes of the effect differ among these studies. We addressed the issue of heterogeneity between studies by computing pooled estimates from a random-effects model. Differences in magnitude between studies may be due to variation in the composition of PM or length of ECG recordings but also by including subgroups of populations on anti-inflammatory drugs or lacking anti-inflammatory defence (GSTM null58). The effects of PM2.5 likely vary depending on pollution sources and particulate constituents; indeed, a multicentre study by Timonen et al25 found that the effects of PM on HRV were dependent on local sources of PM. Increases in PM2.5 concentration were associated with decreases in HF in Helsinki, but a similar increase in PM2.5 was associated with an increase in HF in Ertfurt. Although a 5-min measurement is recommended and highly reproducible,8 ,30 the 24-h measurement includes the nocturnal period during which people in general have a very different autonomic regulation and which is mainly driven by the parasympathetic component.64 However, when we performed a separate analysis for long-term and short-term recordings, we found a decrease for SDNN and rMSSD in both short-term and long-term recordings, although the decrease in long-term recording for rMSSD was statistically not significant (p=0.21). Differences between studies in the HRV particulate air pollution association might also be explained by differences in the disease status of the subjects. Various disease processes (myocardial infarction, diabetes, chronic obstructive pulmonary disease) as well as physiological conditions, including ageing,65 and drugs (β-blockers) alter autonomic control, and therefore change the HRV. However, when the study groups with subjects suffering from cardiovascular diseases were excluded, the combined estimate did not differ significantly from the effect found when these groups were included. Hence, the association between HRV and PM exposure is not only seen in susceptible subgroups. Contrary to our meta-analysis, a recent experimental study9 found no effects of dilute diesel exhaust inhalation for 1 h on heart rhythm and HRV in healthy volunteers or in an ‘at-risk’ population of patients with stable coronary heart disease. Explanations for the discrepancy between these epidemiological data and negative results in controlled conditions may include too short exposure and difference pollution mixture. Indeed, most of the observational studies included an exposure window of 24 h. On the other hand, in the observational studies confounding or residual confounding by ambient temperature cannot be excluded. Of the included studies in our meta-analysis, 20 (69%) adjusted for meteorological conditions (see supplementary table 1).
To determine whether the combined effect is influenced by a particular publication, a sensitivity analysis was performed. HRV parameters were not strongly determined by one study.
Our main analysis included only studies which used a lag of ≤24 h of PM2.5 or PM10 exposure. However, we conducted a separate meta-analysis with studies reporting the effect of a 48-h exposure.13 ,21 ,25 ,28 ,30 The combined effect estimate for 48 h was similar to the effect found for 24 h when occupational studies were excluded for LF, HF and SDNN. The effect of a 48-h exposure could not be calculated for rMSSD due to the lack of studies reporting rMSSD.
The present results should be interpreted within the context of their limitations. First, the analysis was not adjusted for variation in length of ECG recordings. On the other hand, a sensitivity analysis with the different lengths of the ECGs did not reveal differences in combined effect sizes according to length for LF, HF and SDNN. For rMSSD, the analysis stratified for short- and long-term recordings showed only significant results for short-term recordings. Third, if there was heterogeneity in the reporting strategy between studies, we had to address this issue by calculating the β-coefficients to percentages and calculated PM2.5 from PM10 by using the formulae as given in the Methods section. Also, different study designs were used in the combined estimate. Nevertheless, in the sensitivity analysis, we confirmed the robustness of the overall estimate by including only panel studies. In other words, the overall estimate was not strongly influenced by the included studies with a cross-sectional nature. And last, generally accountable for meta-analysis is a publication bias in that studies with a positive result are more likely to be published than negative results. The funnel plots searching for publication bias did not reveal a deficit of small studies with negative results, suggesting that overall there was no publication bias.
The present meta-analysis shows an overall statistically significant inverse association between parameters of HRV and exposure to particulate air pollution, which might be relevant in biological terms. Indeed, the putative mechanisms of the acute effects of PM include sympathetic activation/parasympathetic withdrawal leading to haemostatic and haemodynamic changes that are recognised to increase the risk of cardiovascular events.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online Supplementary 1
- Data supplement 2 - Online Supplementary 2
- Data supplement 3 - Online Supplementary 3
- Data supplement 4 - Online Supplementary 4
Footnotes
Funding The research on air pollution and health at Hasselt University is supported by a grant from the Flemish Scientific Fund (FWO/G.0873.11), tUL-impuls financing and Hasselt University Bijzonder OnderzoeksFonds (BOF). MK has a PhD fellowship of the Research Foundation—Flanders (FWO).
Competing interests None.
Provenance and peer review Not commissioned; internally peer reviewed.