Article Text

Abstract
Objective The role of high sensitivity troponin T (hs-TnT) in the convalescence phase after an acute coronary syndrome (ACS) is unknown. The authors aim to assess the prognostic utility of a single hs-TnT level at 7-week post-ACS. Second, the authors evaluated whether any serial changes in hs-TnT between the index admission and 7 weeks post-ACS had any link with the prognosis. Third, the authors assessed whether the prognostic utility of hs-TnT is independent of various echocardiographic abnormalities.
Methods The authors measured hs-TnT levels in 326 consecutive patients at 7 weeks after an ACS event. The composite end point of death from any cause or acute myocardial infarction was evaluated over a median duration of 30 months.
Results A high 7-week hs-TnT (>14 ng/l) predicted adverse clinical outcomes independent of conventional risk factors, left ventricular dysfunction and left ventricular hypertrophy on echocardiography (adjusted RR: 2.69 (95% CI 1.45 to 5.00)). Patients with persistent hs-TnT elevation at 7 weeks were also at an increased risk of cardiovascular events compared with those with an initial high hs-TnT which then normalised (unadjusted RR 3.39 (95% CI 2.02 to 5.68)).
Conclusion The authors have demonstrated the prognostic utility of a single 7-week hs-TnT measurement in routine ACS patients and that it could be used to assist medium term risk stratification in this patient cohort. In addition, the authors also showed that hs-TnT predicted long-term adverse prognosis independent of various echo parameters. Future studies should evaluate whether tailoring specific treatment interventions to higher risk individuals as identified by an elevated hs-TnT during the convalescence phase of ACS would improve clinical outcomes.
- High sensitivity troponin T
- 7 weeks post-ACS
- prognosis
- echocardiographic abnormalities
- coronary artery disease
- atherosclerosis
- risk stratification
- EBM
- clinical proof of concept studies
- regional blood flow
- coronary haemodynamics
- chronic heart failure
- aorta
- great vessels and trauma
- arrhythmias
- sudden cardiac death
- ventricular fibrillation
- cardiac function
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
- High sensitivity troponin T
- 7 weeks post-ACS
- prognosis
- echocardiographic abnormalities
- coronary artery disease
- atherosclerosis
- risk stratification
- EBM
- clinical proof of concept studies
- regional blood flow
- coronary haemodynamics
- chronic heart failure
- aorta
- great vessels and trauma
- arrhythmias
- sudden cardiac death
- ventricular fibrillation
- cardiac function
Background and objective
The role of high sensitivity troponin T (hs-TnT) in the risk stratification of patients with acute coronary syndrome (ACS) is now well established and widely practised in many hospitals. hs-TnT improves on the early diagnosis of acute myocardial infarction (AMI) and aids in the identification of patients who are at a higher risk of future adverse events when compared with the conventional troponin assay.1–3 This prognostic role for hs-TnT has also now been extended to include patients with stable chronic coronary artery disease.4 In this study, we evaluated the role of hs-TnT in the convalescence phase after an ACS event. This is potentially important as it could further guide medium term treatment options in this patient cohort. We therefore sought to assess the prognostic utility of a single hs-TnT level at 7-week post-ACS. We also aimed to evaluate whether upward and downward trends of hs-TnT between the index admission and 7 weeks post-ACS had any link with prognosis. We also sought to assess the correlation between a 7-week hs-TnT and various adverse echo parameters and whether its prognostic value is independent of these echo abnormalities or not, with particular focus on the presence/absence of left ventricular systolic dysfunction (LVSD). We also compared a 7-week hs-TnT with a 7-week B-type natriuretic peptide (BNP) in terms of which better predicts prognosis after ACS.
Methods
Study population
Three hundred and twenty-six White patients within 7 weeks of diagnosis of ACS (between August 2004 and January 2007) were consecutively recruited from Ninewells Hospital, Dundee. Ethical approval was obtained from the Tayside Committee of Medical Research Ethics and all participating subjects gave written, informed consent. Patients were included if they were diagnosed with an ACS event the preceding 7 weeks. They were assessed by a clinical research fellow during a clinic visit (at 7 weeks post-ACS) and underwent the following investigations:
Clinical history: age, sex, cardiac risk factors, history of ischaemic heart disease or myocardial infarction (MI) and smoking status.
ECG: presence or absence of ST deviation (>0.5 mm).
Hs-TnT at 7 weeks follow-up. The value of hs-TnT on initial ACS admission refers to the peak hs-TnT level.
Bedside BNP assay.
Laboratory tests: haemoglobin and estimated glomerular filtration rate (eGFR). We used the modified Jaffe method to measure creatinine and then used the MDRD to estimate eGFR. Our creatinine assay method has previously been calibrated against the reference procedure of LC MS. Our overall method is exactly what is used in every National Health Service (NHS) hospital to estimate eGFR in clinical practice.
Echocardiography: LVSD defined as LV ejection fraction <45% (Simpson's biplane method), calculation of left ventricular mass index (LVMI) and assessment of long axis function.
Calculation of the Global Registry of Acute Coronary Events (GRACE) score based on clinical history, ECG and laboratory values upon first arrival to the Coronary Care Unit or the Acute Medical Admissions Unit.5
The above assessments had all been done also during the index ACS admission, as reported before.6
Laboratory tests
BNP measurement
All samples were collected by venepuncture into EDTA tubes. The blood samples were kept at room temperature and analysed within 4 h of the draw time. Before analysis, each tube was inverted several times to ensure homogeneity. The whole blood was then analysed with the triage BNP assay (Biosite). The inter-assay per cent CV was 8.8% at 71.3 pg/ml, 11.0% at 629.9 pg/ml and 11.6% at 4088 pg/ml. The detection limit was 5 pg/ml and upper measuring limit was 5000 pg/ml. A BNP cut-off of >80 pg/ml has been widely shown to correlate in adverse prognosis in patient with ACS.7
Hs-TnT measurement
Hs-TnT was analysed using the Roche hs-TnT assay using the Elecsys 2010 system. This assay was introduced to routine clinical practice in NHS Tayside in August 2010; prior to its introduction, NHS laboratory evaluation showed the assay to perform as described by the manufacturers and as described in the literature.8 The manufacturer's 99th centile for healthy subjects4 ,9 (13 ng/l) was utilised clinically such that higher values indicate a degree of myocardial damage. The CV at the 99th centile was 9%; internal quality control samples (Randox) with a target value range of 12–20 ng/l were measured with each batch and gave CVs of 4%–5.3% depending on which of the two identical analysers was in use. It is generally recommended in international guidelines that in diagnosing MIs the assay should have a CV of <10%. The manufacturers of the troponin assay we used have data that the CV is <10% when used at levels below the 99th percentile cut-off of 14 ng/l.
Echocardiography
Transthoracic echocardiography was performed by one trained operator (DA) using an Acuson (Sequia 512) imaging system with a 3V2C transducer. The scan was performed with the patient lying in the left lateral position at approximately 45%. The intraobserver correlation for LVMI was r=0.95 (mean difference 1.0 g/m2, SD 8 g/m2).
Left ventricular hypertrophy assessment
Patients were studied with 2D guided M-mode echocardiography in standard views. All measurements were made according to the American Society of Echocardiography (ASE) recommendation at end diastole, taken as the onset of QRS complex. The leading edge to leading edge convention was used to measure interventricular septal thickness, left ventricular internal diameter and left ventricular posterior wall thickness. Measurements were made over at least three separate cardiac cycles and the average taken. Left ventricular mass was calculated according to the formula of Devereux et al 0.80 (ASE left ventricular mass) +0.610 and indexed to body surface area to give an LVMI. Left ventricular hypertrophy was defined as LVMI >110 g/m2 in female subjects and >134 g/m2 in male subjects in accordance with the latest ASE guidelines.11
Assessment of M-mode left ventricular long axis function
2D-targeted M-mode beam was directed from the apex along the hinge points of the mitral valve apparatus and lateral, septal, inferior and anterior LV walls in four- and two-chamber views. The regional displacement was calculated after 60 ms from the beginning of the QRS complex to the first peak of the mitral annular waveform with these points corresponding to mitral and aortic valve closure, respectively.12 Impaired long axis function was defined as atrioventricular plane displacement of <1.0 cm.
Left ventricular systolic function assessment
Quantitative assessment of left ventricular systolic function was made using the modified biplane Simpson's method to calculate a left ventricular ejection fraction.11 Three measurements from successive cardiac cycles were made in the two- and four-chamber views. LVSD was defined as an LVEF <45%.
End points
The composite end point of death from any cause or AMI was evaluated over a median duration of 30 months. AMI was defined as an admission to the hospital with ischaemic chest pain and a positive troponin T level.13 The number of end points achieved in this study referred to the time taken for the occurrence of the first major event. Information on end points was collected from telephone interviews with patients or patient relatives, hospital database and patients case notes. The researcher who was responsible for the collection of the individual end points was blinded to the hs-TnT levels. No patients were lost to follow-up.
Statistical analyses
The mean values and proportion of baseline variables were compared with ANOVA for continuous variables and χ2 test for categorical variables. As hs-TnT is not a normally distributed variable, we presented it in tertiles under baseline characteristics of the study population. Equally, we performed logarithmic transformation10 when presenting the prognostic utility of hs-TnT as a continuous variable. Univariate Cox regression analysis was carried out to look at predictors of cardiovascular events. Multivariate Cox regression analysis using the backward stepwise method was used to look at the independent predictors of cardiovascular end points. Event rates for clinical outcomes were also determined using the Kaplan–Meier method and compared using Log-rank test. All statistical analyses were performed using SPSS for windows (V.16.0). A value of p<0.05 was considered to be statistically significant.
Results
The study population consisted of 326 patients at 7 weeks post-ACS. Index presentation was STEMI in 106 patients, NSTEMI in 156 patients and unstable angina in 64 patients. hs-TnT levels ranged from 3 ng/l to 2070 ng/l. Baseline characteristics of the study population based on their respective hs-TnT tertiles are presented in table 1. hs-TnT levels were significantly correlated with increasing age and the presence of major cardiovascular risk factors. The presence of anaemia and impaired renal function (defined as CKD stages III, IV and V) were also strongly correlated with hs-TnT levels. Higher levels of hs-TnT were also significantly associated with the higher prevalence of echo abnormalities in the form of left ventricular hypertrophy, LVSD and impaired long axis function.
Baseline characteristics of post-ACS patients based on tertiles of 7-week high sensitivity (hs) troponin T levels
Association between hs-TnT and clinical outcomes
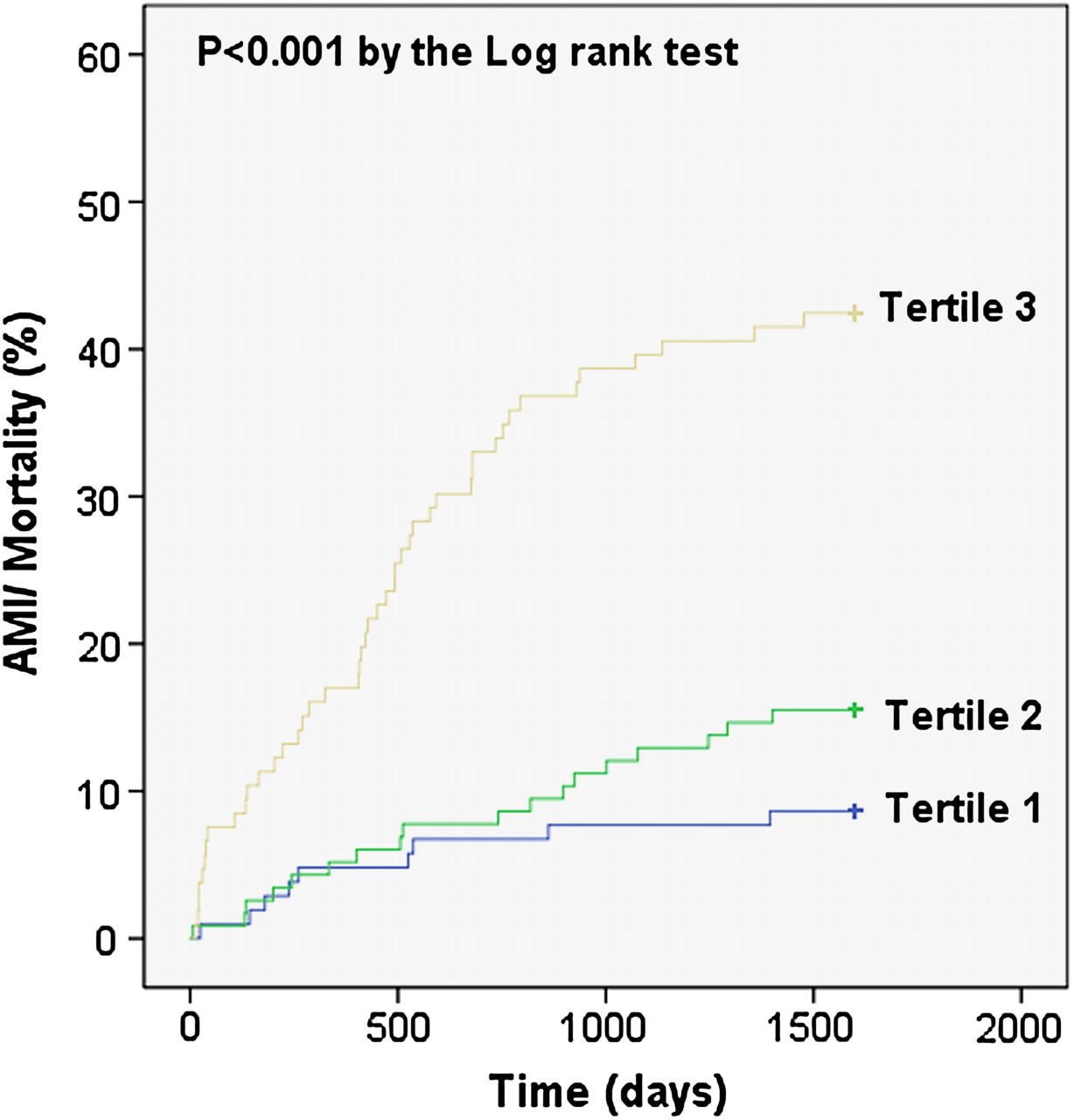
Over a median follow-up of 30 months (IQR 12–40 months), there were 49 readmissions with AMI and 36 deaths, corresponding with 26% event rate. Patients in the third hs-TnT tertile were six times more likely to sustain a cardiovascular event compared with those in the first tertile (unadjusted RR 6.11 (95% CI 2.98 to 12.50)) (figure 1). The univariate predictors of AMI/death at 30 months are shown in table 2. hs-TnT is presented both as a categorical variable, using a cut-off of 14 ng/l and as a continuous variable (natural logarithm transformation). Significant univariate predictors were entered into a multivariate model, yielding two independent predictors in the form of impaired renal function and elevated hs-TnT (table 3).
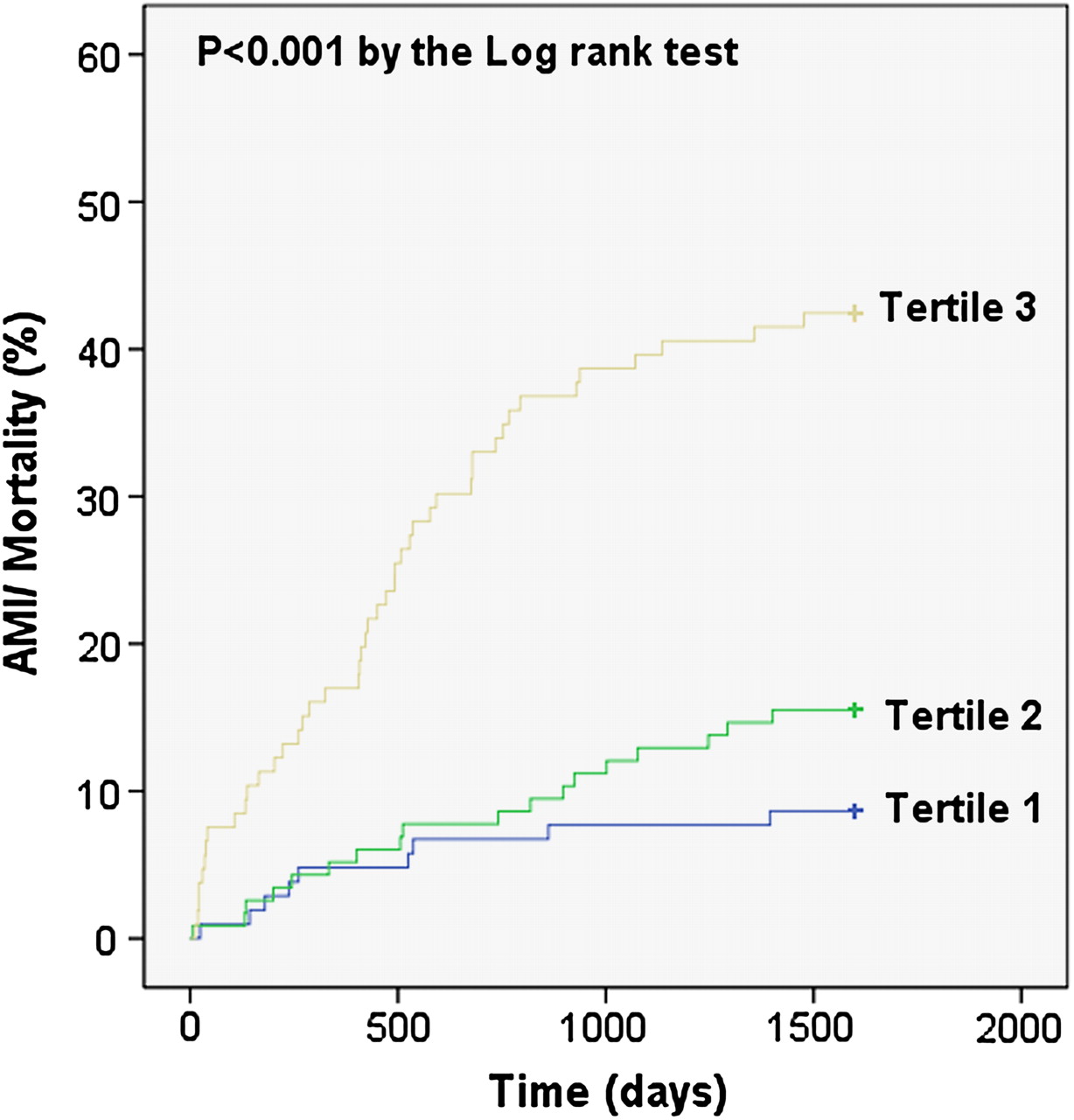
Kaplan–Meier curves showing the cumulative incidence of death/acute myocardial infarction (AMI) at median 30 months, according to the high sensitivity troponin T tertiles at 7 weeks postacute coronary syndrome (p<0.001 by the Log-rank test).
Univariate Cox proportional hazard analyses for the composite outcome of death or acute myocardial infarction at median of 30 months follow-up (based on 7-week variables)
Independent predictors of clinical end points from multivariate Cox regression analyses
Value of hs-TnT trend
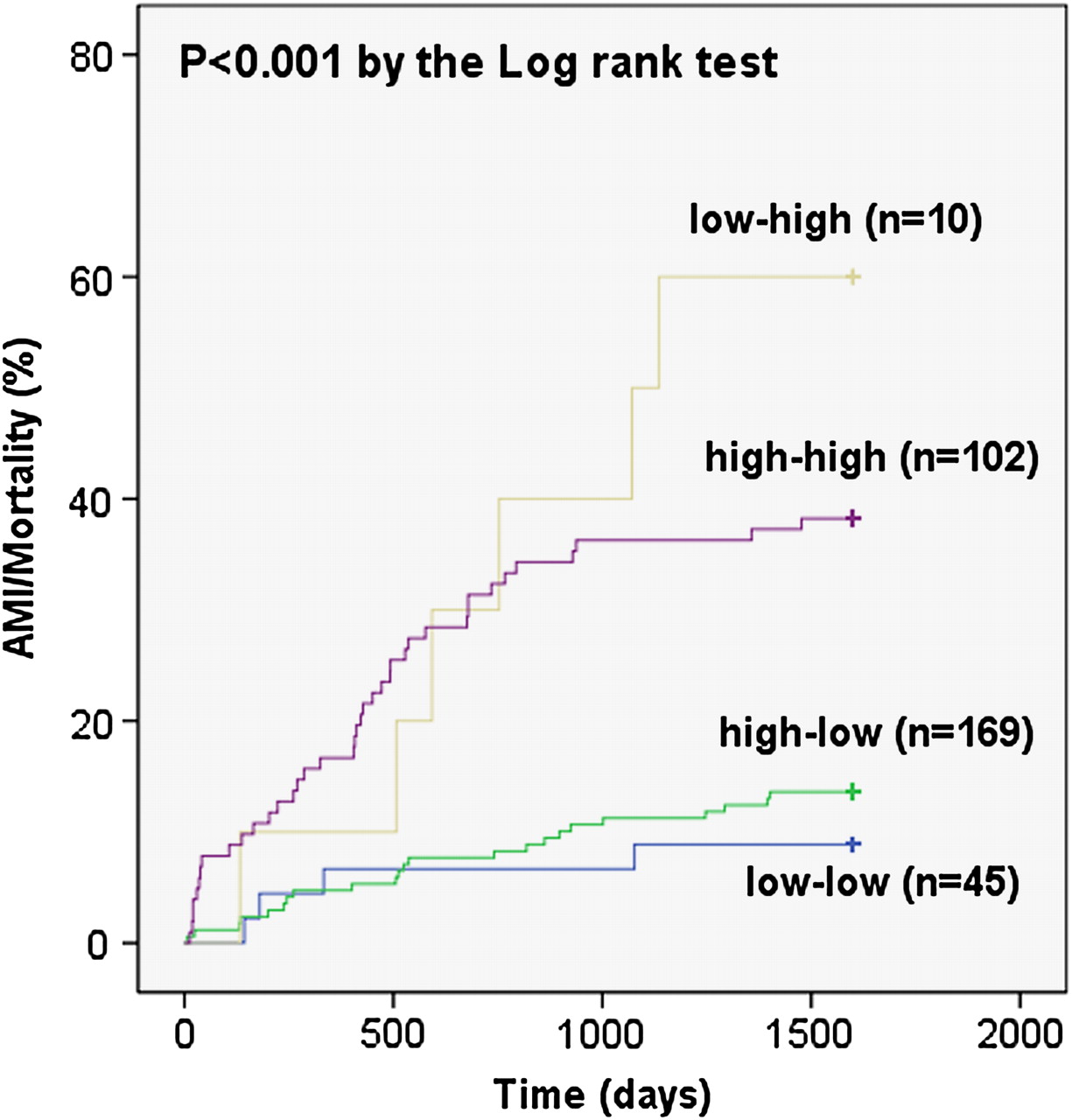
We evaluated the correlation between clinical end points and the hs-TnT trends between index admission and 7-week post-ACS. Based on a cut-off level of 14 ng/l, 45 patients had persistently low hs-TnT levels, 169 patients had high hs-TnT levels which subsequently normalised at 7 weeks follow-up. Only 10 patients developed new hs-TnT elevation at 7 weeks and 102 patients were found to have persistent hs-TnT elevation. Figure 1 shows the Kaplan–Meier survival curves for these respective four groups of patients. Patients with persistent hs-TnT elevation were threefold more likely to sustain a cardiovascular event as compared with those with initial hs-TnT elevation on index admission which subsequently normalised at 7 weeks post-ACS (unadjusted RR 3.39 (95% CI 2.02 to 5.68)). Table 4 demonstrates the relationship between clinical/echo parameters at 7 weeks post-ACS and the four groups of patients divided according to different hs-TnT trends. As expected, patients with persistent hs-TnT elevation presented with higher admission GRACE score and were found to have significantly higher rates of echo abnormalities at 7 weeks post-ACS.
Univariate association between 7-week follow-up clinical variables and the respective high sensitivity (hs) troponin T trends between baseline and 7 weeks
Association among hs-TnT, LVSD and clinical outcomes
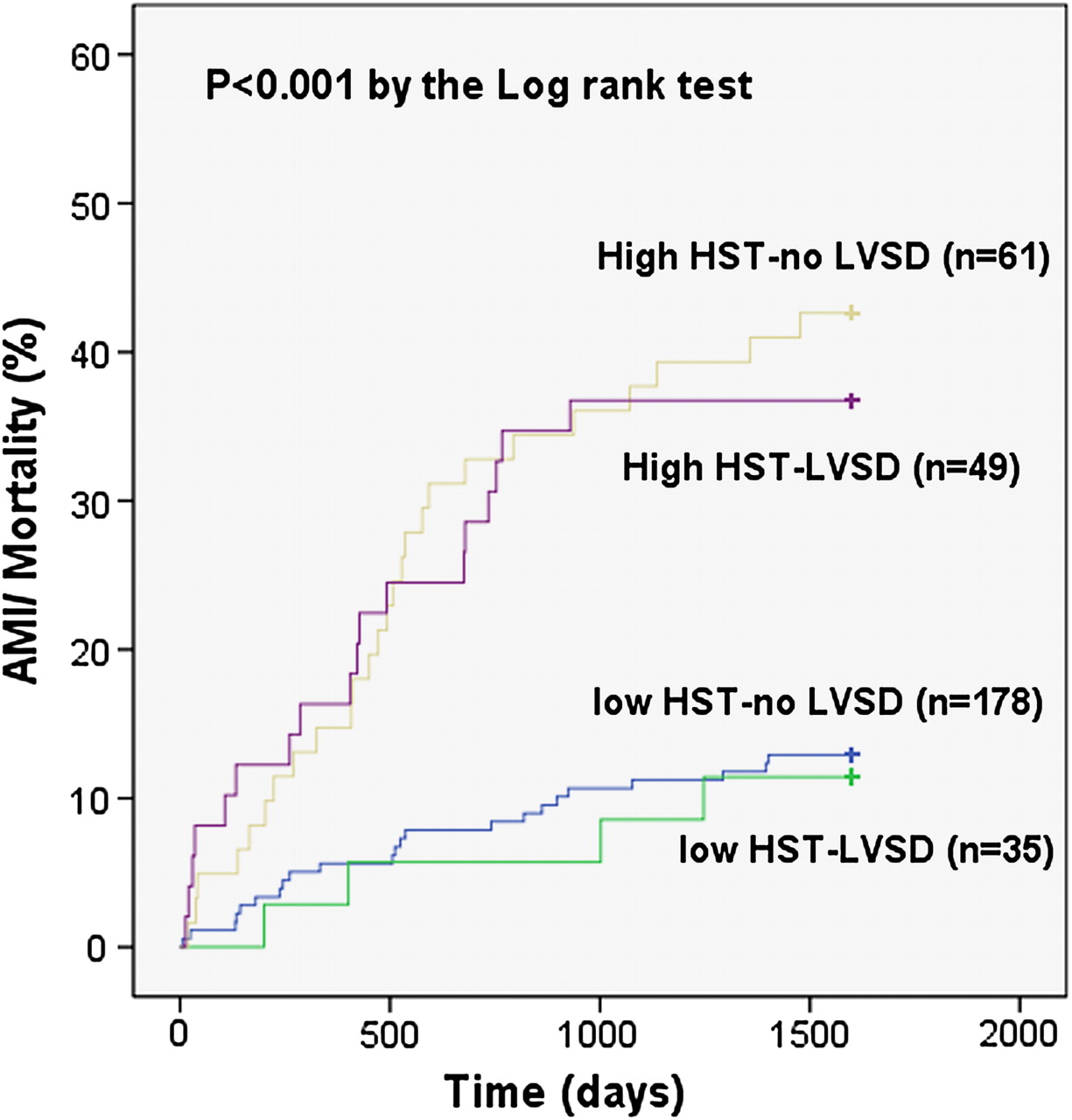
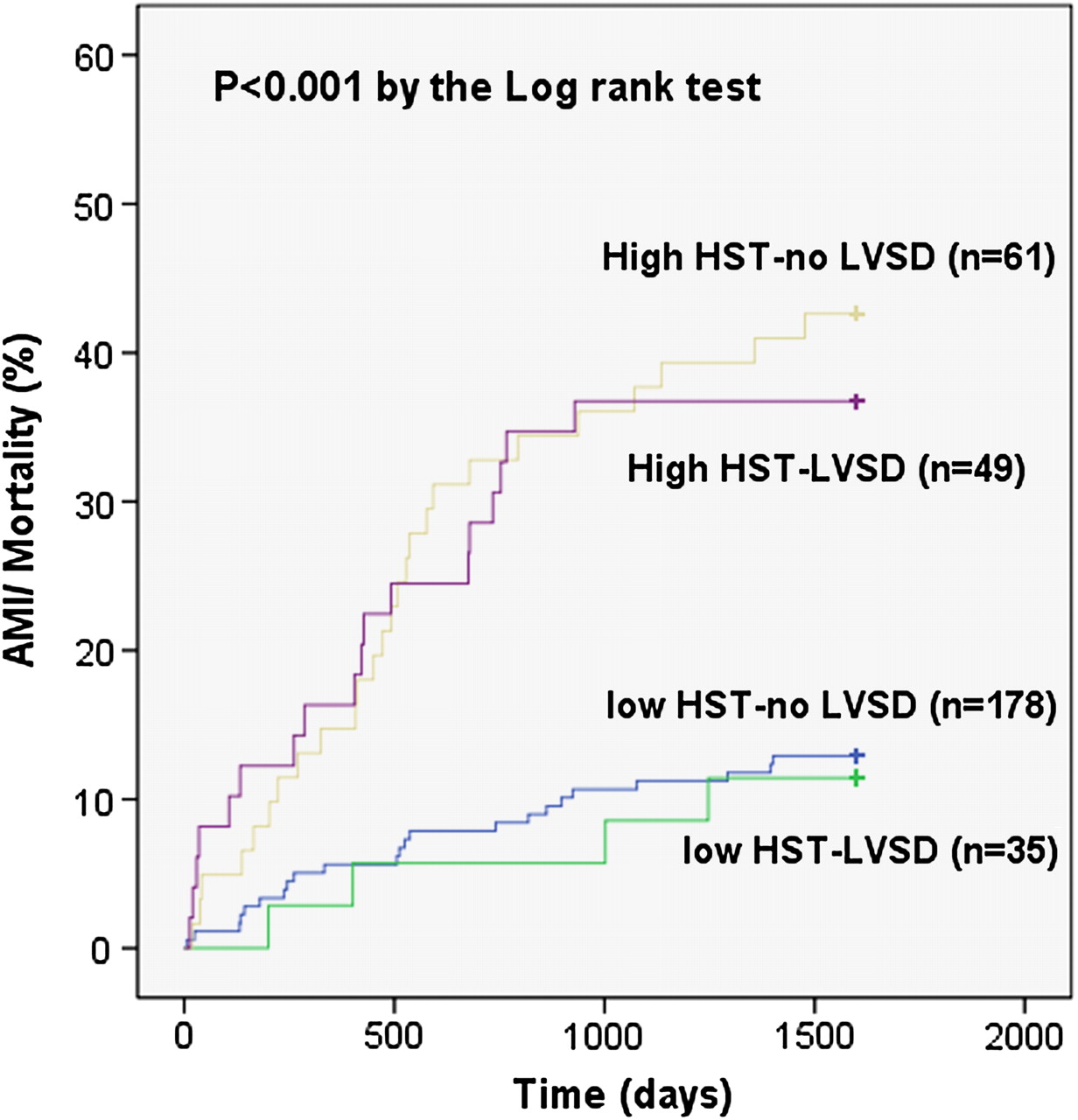
The association between hs-TnT and LVSD on admission and at 7 weeks post-ACS follow-up is shown in figures 2 and 3. hs-TnT predicted all adverse long-term outcomes (MI or death) regardless of the presence or absence of LVSD (p<0.001 by the Log-rank test). Similar significant trends were observed when the end points of MI and death were analysed separately (p<0.001 by the Log-rank test).

Kaplan-Meier curves showing the cumulative incidence of death/acute myocardial infarction (AMI) at median 30 months, according to the trends of high sensitivity troponin T. Each group is labelled by the high sensitivity troponin T levels on admission and at 7 weeks follow-up (p<0.001 by the Log-rank test).

Kaplan–Meier curves showing the cumulative incidence of acute myocardial infarction (AMI)/mortality at median 30 months, according to the trends of 7-week high sensitivity (hs) troponin and the presence/absence of 7-week left ventricular systolic dysfunction (LVSD) (p<0.001 by the Log-rank test). HST, high sensitivity troponin T.
Discussion
The main findings of this study can be summarised as follows: First, during the convalescence phase (7 weeks) after an ACS event, hs-TnT further risk stratifies patients who are at risk of long-term cardiovascular events. Second, the prognostic utility of hs-TnT is independent of conventional cardiovascular factors and surpasses that of both BNP and echo LVSD. Third, we have demonstrated that patients who have persistent hs-TnT elevation at 7 weeks post-ACS were at a higher risk (threefold increase) of long-term cardiovascular events when compared with those in whom hs-TnT levels normalised at 7-weeks follow-up.
Two recent studies demonstrated the prognostic utility of an acute hs-TnT sample in patients presenting with ACS.2 ,14 In both studies, elevated hs-TnT sampled at the time of presentation predicted 1- and 4-year all-cause mortality. Our study extends this observation to establish the prognostic role of hs-TnT at 7 weeks post-ACS. Importantly, this is the first study to address the role of serial hs-TnT measurements in ACS patients. We found that patients who develop new hs-TnT elevation and those who have persistent hs-TnT levels at 7 weeks are at a very high risk of adverse clinical outcomes (figure 4). The former group was however too small in our study to attach much significance to. Conversely, patients with hs-TnT elevation during index admission which subsequently normalised at 7 weeks post-ACS had a low cardiovascular event rate on long-term follow-up. This latter group was quite substantial and represented 52% of our ACS cohort. These findings have important clinical implications for the care of patients with ACS. It demonstrates that hs-TnT has potential clinical application both during the acute phase and at 7 weeks in order to assess the longitudinal course after ACS, that is, a 7-week hs-TnT could redefine risk in those who had an elevated hs-TnT at the baseline ACS event. Our study is also consistent with the findings of deFilippi et al who found in a cohort of older community dwelling adults that changes in hs-TnT over time accurately predicted new onset HF and cardiovascular death.15

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan–Meier curves showing the cumulative incidence of death/acute myocardial infarction (AMI) at median 30 months, according to the trends of high sensitivity (hs) troponin T. Each group is labelled by the hs troponin T levels on admission and at 7 weeks follow-up (p<0.001 by the Log-rank test). HST, high sensitivity troponin T; LVSD, left ventricular systolic dysfunction.
As well as the trends discussed above, we performed multivariate analyses and the 7-week hs-TnT level emerged as a significant and independent predictor of long-term outcomes on multivariate analyses in post-ACS patients (table 3). This is certainly consistent with studies where troponin samples were taken either acutely in ACS or in chronic stable patients.2 ,4 ,14 A novel additional finding in our study is that the prognostic power of hs-TnT was found to be superior to that of BNP as evidenced on both univariate and multivariate analyses. The role of BNP as a prognostic marker in ACS is well established from previous trials.16 ,17 Indeed, we previously found that serial measures of BNP predicted prognosis after ACS independent of echo abnormalities.18 We found the same here for hs-TnT except that hs-TnT was better than BNP.
We also focused on the relationship between echo LVSD and hs-TnT. Intriguingly, we found that hs-TnT predicted all adverse long-term outcomes (MI or death) regardless of the presence or absence of LVSD. Figures 2 and 3 clearly illustrate this observation. Indeed, the prognostic significance of hs-TnT appeared to overwhelm the prognostic role of LVSD. Since this is a key finding, we report our findings on this in great detail, that is, we report results for both baseline LVSD and 7-week LVSD and we also report separately for the end points of MI, mortality and their combination. Intriguingly, the results are essentially the same for all six analyses which confirms the robustness of this new finding of ours.
A major and unique strength of our study is that hs-TnT measurements were complemented by the availability of echo data both at baseline and at 7 weeks. In a group of patients with moderate to severe aortic stenosis, Rosjo et al19 demonstrated that echocardiography indices of structure and function, most notably LVM, were independently predictive and closely correlated with hs-TnT levels. These findings are consistent with our present study in that the prevalence of left ventricular hypertrophy, LVSD and impaired long axis function were significantly higher with increasing tertiles of hs-TnT (table 1). However, despite the above, this study clearly demonstrates that hs-TnT predicts long-term outcomes independent of these important echocardiographic abnormalities.
The mechanism for persistent or new hs-TnT elevation in the post-ACS phase remains unknown. Our study does suggest age, anaemia and a higher composite cardiovascular risk disease burden (ie, history of hypertension, diabetes and echo abnormalities) could be the main factors associated with continued troponin release (table 4). In addition, the strong correlation between renal dysfunction and hs-TnT levels might indicate some form of impedance to hs-TnT clearance from the circulation. In fact, the presence of higher troponin T fragments in haemodialysis patients has been previously been attributed to impaired renal clearance.20 Overall, the most likely explanation of our results is that hs-TnT reflects a composite of both CV risk factors and cardiac target organ damage (echo abnormalities) and that as a prognostic indicator, it eclipses individual risk factors and individual measures of target organ damage because it is a composite of all of them. In this respect, hs-TnT could be easier to use to reclassify risk at 7 weeks than reassessing all individual risk factors as this would include having to perform another echo at 7 weeks.
There are two limitations worth mentioning in this study. First, due to the modest number of patients, we cannot deduce much about the subgroup of patients (n=10) with new hs-TnT elevation at 7 weeks. The main implications of our study relate to those with either persistent hs-TnT elevation or a high/low pattern. Second, this study was conducted in the era when STEMI patients were thrombolysed and, therefore, revascularisation rates in the form of percutaneous coronary intervention are substantially lower than nowadays in Western countries. Nevertheless, this study reflects the real world and routine ACS patients rather than a clinical trial population.
In summary, we have demonstrated for the first time the prognostic utility of a single 7-week hs-TnT measurement in routine ACS patients which helps refine medium term risk stratification and medium term treatment strategies in this patient cohort. Future studies should evaluate whether tailoring specific treatment interventions to higher risk individuals as identified by an elevated hs-TnT during the convalescence phase of ACS would improve clinical outcomes.
Key messages
During the convalescence phase (7 weeks) after an ACS event, hs-TnT further risk stratifies patients who are at risk of long-term cardiovascular events.
The prognostic utility of hs-TnT is independent of conventional cardiovascular factors and surpasses that of both BNP and echo left ventricular systolic dysfunction.
We have demonstrated that patients who have persistent hs-TnT elevation at 7 weeks post ACS were at a higher risk (threefold increase) of long-term cardiovascular events when compared to those where hs-TnT levels normalised at 7-weeks follow-up.
Acknowledgments
The authors would like to thank the British Heart Foundation for generously funding this project.
References
Footnotes
Funding British Heart Foundation.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The ethics approval was provided by the Tayside Committee of Medical Research Ethics.
Provenance and peer review Not commissioned; externally peer reviewed.