Article Text

Abstract
Objective Individuals with depression are at risk of heart failure. This study was designed to elucidate the relationship between depression and subclinical left ventricular (LV) changes in the general Korean population.
Design Cross-sectional cohort study.
Setting University hospital.
Patients A total of 2420 participants, aged 40–79 years, without known cardiovascular disease, were recruited from the Korean Genome Epidemiology Study.
Methods All individuals underwent conventional two-dimensional echocardiography and tissue Doppler imaging (TDI) to measure LV changes. In addition, subjects answered the Beck depression inventory I (BDI-I) questionnaire to assess depression levels. Participants were assigned to one of three groups based on the BDI-I score: no depression (0≤ BDI-I <10), mild depression (10≤ BDI-I <20), and moderate to severe depression (BDI-I ≥20).
Results LV diastolic function parameters, such as the transmitral A wave velocity and E/A ratio, TDI early diastolic velocity (Ea), and E/Ea ratio, were progressively altered across the levels of depression (all p<0.01). After multivariate adjustment, subjects with moderate to severe depression showed a significantly higher LV mass index (p=0.019) and lower TDI Ea velocity (p=0.006) compared with those without depression. In linear regression models, the presence of depression (BDI-I ≥10) was independently associated with a lower TDI Ea velocity (p=0.004).
Conclusions Individuals with moderate to severe depression showed subclinical alterations in LV structure and function. These findings support the hypothesis that clinical depression may be an independent risk factor for the development of cardiovascular disease.
- Depression
- diastole
- echocardiography
- left ventricle
- tissue Doppler imaging
- cardiac function
- hypertension
- metabolic medicine
- metabolic syndrome
- imaging and diagnostics
- allied specialities
Statistics from Altmetric.com
- Depression
- diastole
- echocardiography
- left ventricle
- tissue Doppler imaging
- cardiac function
- hypertension
- metabolic medicine
- metabolic syndrome
- imaging and diagnostics
- allied specialities
Introduction
Depression is common in patients with cardiovascular disease (CVD), and 14%–50% of patients with CVD have some degree of depression.1–6 Previous cohort studies have shown that individuals with depressive symptoms are at an increased risk of developing coronary artery disease (CAD).7–10 In addition, depression has been found to be a predictor of poor prognosis in patients with pre-existing heart disease, including congestive heart failure, atrial fibrillation, angina pectoris and myocardial infarction.11–16
Although the pathobiological mechanism linking depression with CVD has not been clearly elucidated, it seems likely that a variety of biobehavioural pathways are involved in the connections between these disease entities. In addition to biobehavioural pathways, it has been hypothesised that cardiac structural or functional changes might precede the development of clinical symptoms in patients with depression. Considering that left ventricular (LV) diastolic dysfunction is the first step in the ischaemic cascade and the earliest manifestation of diverse cardiomyopathy,17 it is possible that subclinical LV diastolic dysfunction may be observed in patients with depression. However, few studies have examined the relationship between LV systolic/diastolic function and depression using conventional two-dimensional (2D) echocardiography,18 and no previous study has reported a significant relationship between depression and cardiac disease severity.
Tissue Doppler imaging (TDI) has emerged as a useful tool for the early detection of myocardial systolic and diastolic dysfunction in addition to its use as a prognosticator for CVD. Until recently, no epidemiologic data has explored the relationship between depression and LV functional changes using TDI.
Using a sensitive echocardiographic TDI technique in the general Korean population, we conducted a cross-sectional analysis to investigate the relationship between depression and subclinical LV changes.
Methods
Study cohort
The study cohort was part of the ongoing population-based Korean Genome Epidemiology Study previously called the Korean Health and Genome Study.19 A total of 5015 participants were assessed biennially with scheduled on-site follow-up visits from 2001. Detailed information on the cohort study design and the selection criteria for this ongoing prospective study are available in previous reports.20 Cohort members, aged 40–79, who participated in the 5th follow-up study from 26 May 2009 to 7 December 2010 were enrolled in this cross-sectional study. Among the 3262 enrolled participants, 2630 underwent a 2D echocardiography that included TDI. This study excluded participants ≥80 years of age, participants with established CVD, arrhythmia including atrial fibrillation, congenital heart disease, previous cardiac surgery, valvular heart disease, regional wall motion abnormality in either ventricle, LV ejection fraction <50%, serum creatinine ≥2.0 mg/dl or malignant neoplasm. Also excluded were participants who regularly took medications for insomnia, anxiety disorder or depression. After excluding a total of 210 subjects, 2420 remained eligible for this investigation. The Human Subjects Review Committee at the Korea University Ansan Hospital approved the protocol of the study, and each participant provided written informed consent.
Assessment of depression
Structured baseline interviews for each study participant were performed by a research assistant. Questions about social and demographic characteristics were asked, and depressive symptoms were evaluated using the Beck depression inventory I (BDI-I).21 Each item in the questionnaire included specific behavioural manifestations of depression and assessed current depressive symptomatology. Several self-evaluative statements in the questionnaires were graded to represent the severity of depressive symptoms, and the participants were asked to choose the statement that best represented him or her during the examination. The minimum and maximum scores were 0 and 63, respectively. Subjects with a BDI-I <10 were considered as not having depression, those with 10≤ BDI-I <20 were categorised as having mild depression, and those with a BDI-I ≥20 were categorised under moderate to severe depression.22
Assessment of cardiac structure and function
A resting conventional 2D echocardiography was performed using Vivid 7 system (GE Vingmed, Horton, Norway) with a 4-MHz transducer. Left atrial volume was obtained using the area-length method, and LV mass was obtained by the Devereux formula. Both values were indexed by body surface area. LV ejection fraction was measured using a modified biplane Simpson's method. Transmitral early (E) and late (A) diastolic blood flow velocities were evaluated by pulsed wave Doppler ultrasound examination, setting the sample volume at the tip of the mitral leaflet from an apical 4-chamber image. TDI was performed for measurements of systolic (Sa), early diastolic (Ea), and late diastolic (Aa) mitral annular velocities, with a 2 mm sample volume at the septal mitral annulus from an apical 4-chamber image. The ratio (E/Ea) of transmitral E and TDI Ea velocities was acquired as a known surrogate indicator of pulmonary capillary wedge pressure.23 All echocardiographic variables were measured and recorded during the examination by a single investigator who was blinded to the clinical data of each patient.
Blood pressure measurements and assessment of cardiovascular risk factors
Participants were seated quietly for at least 5 min before starting blood pressure (BP) measurement. Resting BP was measured twice by trained technicians after a 30 s interval, using a standard mercury sphygmomanometer. Systolic/diastolic BP was measured from the first and the fifth phases of Korotkoff sounds, respectively, and recorded to the nearest 2 mm Hg. Two BP readings were averaged for analysis, and mean arterial pressure was calculated as 2/3 diastolic BP+1/3 systolic BP.
Participants also completed interviewer-administered questionnaires regarding demographic information, medical history and health conditions, family disease history, dietary intake and lifestyle. All examinations were administered by health professionals trained to follow a standardised protocol.
Height (cm) and body weight (kg) were measured, and body mass index (kg/m2) was calculated. Collected blood samples were delivered to the Seoul Clinical Laboratories (Seoul, Korea) for measurement of serum total cholesterol, high-density lipoprotein cholesterol, triglycerides, fasting blood glucose, fasting insulin and high-sensitivity C reactive protein (hsCRP). Metabolic syndrome was defined based on a modified version of the National Cholesterol Education Program Adult Treatment Panel III.
Statistical analysis
Descriptive values were presented as mean (SD) for continuous variables or a proportion for categorical variables. Comparisons of demographic and echocardiographic variables were performed using a one-way analysis of variance, and χ2 tests for categorical variables, as appropriate. Multivariate analyses for the comparison of LV structure and function according to depression levels was performed by an analysis of covariance with two models applied separately to each of the measurements of cardiovascular structure and function: model 1, adjusted for age, sex and body mass index; and model 2, adjusted for model 1 plus heart rate, mean arterial pressure, fasting blood glucose, hsCRP, antihypertensive medication and antidiabetic medication. Pairwise comparisons based on the estimated marginal means were used with a Bonferroni adjustment for multiple comparisons. Covariates for the multivariate models were selected on the basis of clinical relevance and univariate correlation analysis. In addition, the independent relationship between TDI Ea velocity and the presence of depression (BDI-I ≥10) were examined with two multivariate stepwise linear regression models. Data were analysed using the SPSS statistical package (ver. 12.0; SPSS Inc.). A probability value of p<0.05 (two-sided) was considered statistically significant.
Results
There were 2420 middle-aged participants in the study, all of whom were free of overt CVD except hypertension or diabetes mellitus. Among them, 1732 participants had no depression, 547 had mild depression, and 141 had moderate to severe depression. Demographic and clinical characteristics of the study participants are described in table 1. Participants with moderate to severe depression were older, had lower diastolic BP, and included more women than the other groups. Although the proportion of established cases of diabetes mellitus did not differ among the groups, more participants with moderate to severe depression were on antidiabetic medication as compared with the other groups. Fasting serum insulin concentrations were also higher in participants with moderate to severe depression. There were no significant differences in hsCRP values and prevalence of metabolic syndrome, according to level of depression (table 1).
Demographic and clinical characteristics of 2420 study participants by BDI-I score
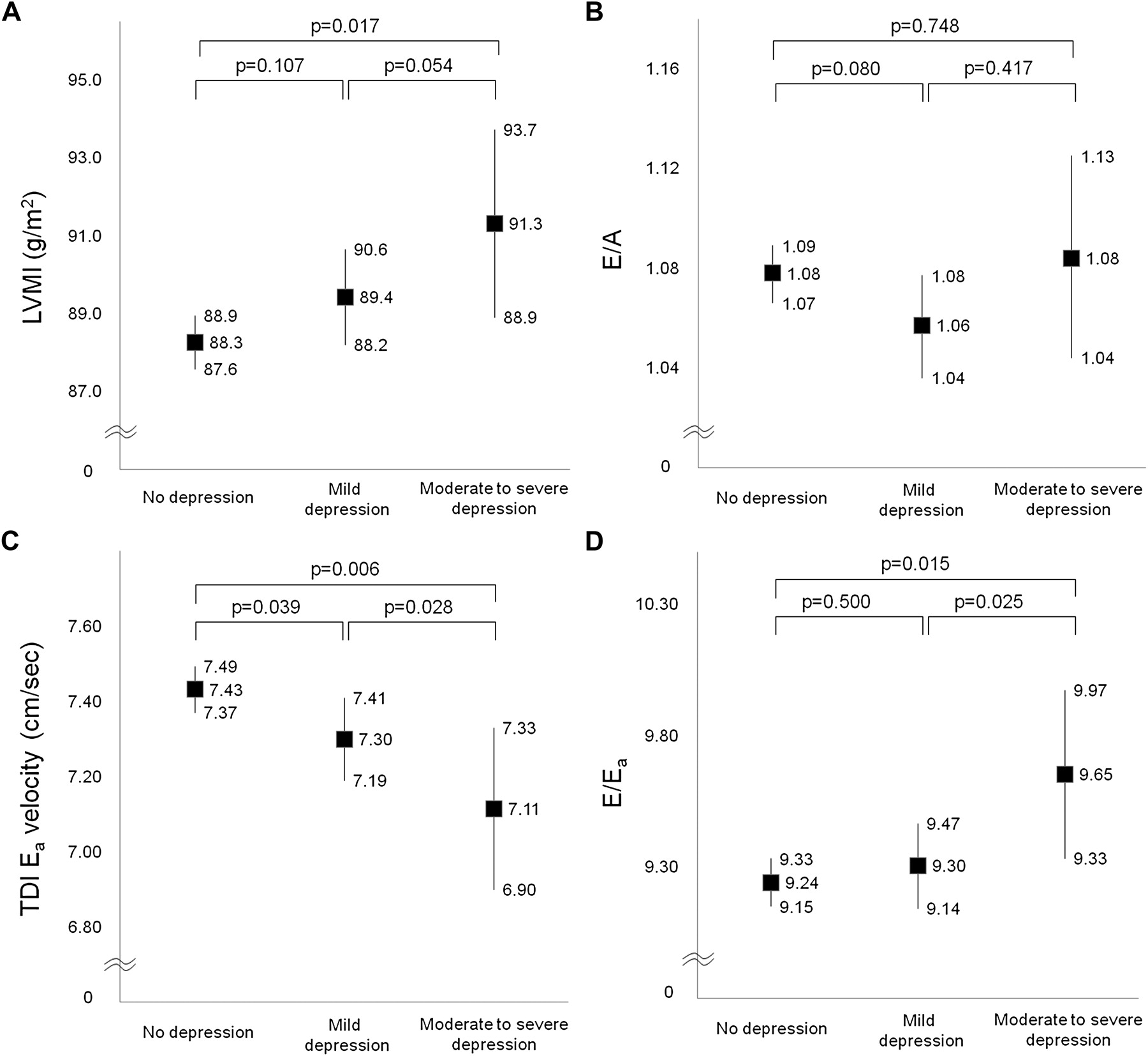
Participants with moderate to severe depression had a higher transmitral A wave velocity, lower E/A ratio, lower TDI Ea and higher Aa velocities, and higher E/Ea ratio (table 2). Table 3 presents the multivariate-adjusted echocardiographic data. There were no significant differences in transmitral A wave velocity, E/A ratio and TDI Aa velocity among the study groups. On the other hand, TDI Ea velocity consistently showed statistically significant differences across depression levels after adjusting for age, sex, body mass index, heart rate, mean arterial pressure, fasting blood glucose, hsCRP, antihypertensive medication and antidiabetic medication (p=0.006 vs no depression, p=0.028 vs mild depression) (figure 1). Participants with moderate to severe depression also had higher LV mass indices than participants without depression (p=0.017) (figure 1 and table 3).
Echocardiographic characteristics of 2420 study participants by BDI-I score
Comparison of cardiac structure and function according to level of depression: multivariate analysis
{kind=link}
Multivariate-adjusted mean values, and 95% CIs of LV structural and diastolic functional variables, by classification of depression after adjustment for age, sex, body mass index, heart rate, mean arterial pressure, fasting blood glucose, hsCRP, antihypertensive medication and antidiabetic medication. hsCRP, high-sensitivity C reactive protein; LVMI, left ventricular mass index; TDI, tissue Doppler imaging.
In the linear regression models, the presence of depression (BDI-I ≥10) was independently associated with TDI Ea velocity after adjusting for age, sex, body mass index, heart rate, mean arterial pressure, fasting blood glucose, hsCRP, antihypertensive medication and antidiabetic medication (table 4).
Association between the presence of depression (BDI-I ≥10) and TDI Ea velocity: multivariate analysis
Discussion
We investigated the relationship between depression and LV structure and function in CVD-free subjects from the general Korean population. In a total of 2420 participants, we found that moderate to severe depression is associated with subtle LV structural and functional changes. Interestingly, the presence of subclinical LV diastolic dysfunction was confirmed only by the TDI technique, not by conventional echocardiography. This is the first report demonstrating that clinical depression is related to LV diastolic functional impairments without overt manifestation of CVD.
Lett et al previously investigated the association between depression and LV diastolic function, as well as systolic function in patients with stable angina pectoris.18 However, a significant relationship between depression and LV function was not found after adjusting for conventional CVD risk factors. Although comprehensive measurements of systolic function, diastolic function, inducible ischaemia and regional wall motion abnormalities were obtained by Lett et al, their study was limited by the absence of TDI data, which is regarded as a more objective and sensitive myocardial parameter for early changes in LV function.18 In the present study, we also could not find any significant difference in LV diastolic function based on the multivariate analyses without TDI data.
Although depression is a known predictor of poor prognosis for patients with chronic heart failure, atrial fibrillation, angina pectoris and myocardial infarction,11–16 controversy exists as to whether depression is a cause or a consequence of poor cardiovascular outcomes because of diverse potential confounding factors. For example, the symptoms of severe CVD could impair patient quality of life and affect mood status, and patients with depression are more likely to report worse health status, such as symptoms burden, physical limitations or reduced quality of life, as compared with those without depression.3 Accordingly, studies examining the relationship between depression and the cardiovascular prognosis of patients who had been treated for various CVD must be interpreted carefully.2 ,24
Until recently, none of the randomised placebo-controlled studies evaluating the effects of treating depression using medication or cognitive-behavioural therapy in patients with myocardial infarction, or chronic heart failure, demonstrated clinical benefits in the cardiovascular hard end points.25–28 Based on these results, although improvements in depressive symptoms were small, and some of the trials were underpowered, it is likely that depression may not be the cause of a worse cardiovascular prognosis.29
On the other hand, several cohort studies and meta-analyses support the notion that depression can cause or worsen CVD. In these studies, depressed subjects who were free of clinically apparent CVD developed more cases of CAD during the follow-up period. The risk for first CAD in patients with depression was relatively lower, but higher than passive smoking.7–10 Our data provide additional evidence that depression may lead to the development of CVD because it does not appear that subclinical changes in LV without overt CVD symptoms could cause a depressed mood in a relatively healthy general population.
A variety of biobehavioural pathways have been under investigation to elucidate the connection between depressive symptoms and cardiac change. Treatment adherence, lifestyle factors, platelet reactivity, dysregulation of the autonomic nervous system, dysregulated hypothalamic-pituitary-adrenal axis activity, and altered immune/inflammation responses were suggested as possible biobehavioural links.30–35 Among these factors, altered immune/inflammation responses are considered a leading mechanism of worse cardiovascular outcomes associated with depression, and increased serum CRP concentration, an independent risk factor for CAD, was also demonstrated in subjects with depression.30 ,34 ,35 However, in our study, serum hsCRP concentration was comparable among study groups, and no interaction was identified between LV function and serum hsCRP concentration. Based on these findings, it is likely that other inflammatory cytokines, such as interleukin-6 and tumour necrosis factor-α, might function as mediators between subclinical LV diastolic dysfunction and depression.
Study limitation
Although the present study contains several strengths, such as the epidemiological setting and the application of a novel TDI technique for the evaluation of LV function, it has several limitations. First, because of a cross-sectional study design, we are not able to assert a causal relationship between depression and subclinical LV changes in asymptomatic patients who were free of CVD. Second, systematic interview, including follow-up evaluation for the diagnosis of depression, was not conducted by a trained psychiatrist. Third, the severity of depression was evaluated only by the BDI scoring method. Although BDI is an effective and well-validated tool in assessing depression in patients with CVD, there are other validated questionnaires, other than BDI, in the diagnosis of depression. Fourth, we excluded participants who were 80 years old or more, because they might have unidentified confounding factors such as hidden malignancy or potential CAD. Considering that the incidence of diastolic dysfunction is very high in this aged population group, their exclusion might have influenced the study results. Finally, given that a variety of sociocultural factors might influence the development of depression, a population-based study limited to a single ethnic group cannot generalise study findings to other ethnic groups.
Conclusions
Depression has been known to be a risk factor of CVD and an independent predictor of worse cardiovascular outcomes. Whether depression is a cause or consequence of CVD remains unclear. Our results, demonstrating the presence of subclinical LV diastolic functional and structural changes in depressed subjects without CVD, suggest that clinical depression is likely to lead to subclinical LV alterations. Further studies on the mechanisms underlying depression, and the impairment of LV structure and function, are needed. In addition, researches on whether such alterations progress to overt heart failure, and are reversible with pharmacologic and psychotherapeutic interventions, are also needed.
References
Footnotes
Funding This study was supported by grants (2009-E00454-00 and 2010-E71001-00) from the Korean Centers for Disease Control and Prevention.
Competing interests None.
Patient consent Obtained.
Ethics approval This study was approved by the Human Subjects Review Committee at the Korea University Ansan Hospital.
Provenance and peer review Not commissioned; externally peer reviewed.