Article Text

Abstract
Objective Low-gradient (LG) severe aortic stenosis (AS) and preserved EF with reduced stroke volume are associated with an adverse prognosis, but the relationship of stroke volume index (SVI) with mortality among a range of values is unknown. We investigated the prognostic impact of SVI in this population.
Methods We examined 405 consecutive patients with preserved EF (≥50%) and severe AS (valve area <1.0 cm2) with LG (<40 mm Hg) using echocardiography. Patients were stratified into quartiles based on SVI distribution (group 1: <38 mL/m2 (n=90), group 2: 38–43 mL/m2 (n=105), group 3: 43–48 mL/m2 (n=104) and group 4: >48 mL/m2 (n=106)).
Results Groups 1 and 2 had poorer survival with medical management compared with 3 and 4 (3-year estimate 46% and 67% vs. 78% and 73%, respectively, p=0.002) although aortic valve replacement referral rate was similar (53%–62%, p=0.57). An inverse relationship was observed between SVI and mortality (HR 1.28 (1.11 to 1.46) per every 5 mL/m2 decrease in SVI). After multivariable analysis, SVI was the strongest predictor of mortality (HR 0.92 (0.89 to 0.95), p<0.0001). Using different SVI cutpoints, SVI <35 was associated with highest mortality (HR 2.36 (1.49 to 3.73), p<0.001), followed by SVI <38 (HR 2.09 (1.39 to 3.16), p<0.001) and by SVI <43 (HR 2.05 (1.38 to 3.05), p<0.001). Survival with SVI ≥43 was similar to age and sex-matched controls (3-year estimate 84%, p=0.24); survival for SVI <43 was significantly worse (3-year estimate 63%, p<0.001).
Conclusions Lower SVI is incrementally associated with mortality in LG severe AS with preserved EF. These findings have implications for classification of AS severity, identification of high-risk groups and subsequent management.
Statistics from Altmetric.com
Introduction
Low flow, low-gradient (LG) severe aortic stenosis (AS) with preserved EF is a recently described syndrome associated with reduced survival.1–6 The mechanism of low stroke volume (SV) has been attributed to reduced systemic arterial compliance (SAC), smaller LV cavity size due to concentric remodelling, restrictive physiology resulting in impaired LV filling and diminished LV systolic function despite preserved EF.7 In order to improve AS assessment and determine the optimal treatment strategy, a new flow-gradient classification has been proposed incorporating the mean aortic valve gradient along with normal vs. reduced stroke volume index (SVI).5 Studies have arbitrarily used a cutpoint of SVI <35 mL/m2 to define the low flow group;1–6 however, other cutpoints have not been investigated, and whether SVI has a graded relationship for predicting outcome in this group of patients is unknown. We have recently investigated the prevalence of flow-gradient patterns in severe AS with preserved EF at our own institution and found that SVI <35 mL/m2 is strongly predictive of poor outcome in patients with LG severe AS and preserved EF.8 We hypothesised that lower SVI may have a graded association with mortality and that such knowledge may improve risk prediction in this population. Accordingly, we investigated the prognostic impact of SVI among a range of values in a population of patients with LG severe AS with preserved EF.
Methods
Patients
The Mayo Clinic Institutional Review Board approved this cohort study. Consecutive patients aged ≥18 years who underwent transthoracic echocardiography between 1 January 2006 and 31 December 2011 with the following criteria were enrolled: (1) aortic valve area (AVA) <1.0 cm2, (2) preserved LV EF (≥50%), (3) LG (mean gradient <40 mm Hg) and (4) absence of prosthetic valves, complex congenital heart disease, supravalvular or subvalvular AS, hypertrophic cardiomyopathy, and concomitant moderate or severe native valvular lesions. These criteria led to a final study population of 405 patients. The medical record was manually reviewed for symptoms, comorbidities and laboratory data.
2D and Doppler echocardiography
Comprehensive 2D and Doppler echocardiographic studies were performed on commercially available ultrasound equipment (Acuson Sequoia, Siemens Medical, Mountain View, California, USA; Vivid-7, GE Healthcare, Milwaukee, Wisconsin, USA; and IE33, Phillips Healthcare, Andover, Massachusetts, USA) in accordance with the American Society of Echocardiography guidelines.9 ,10 Blood pressure was measured by manual sphygmomanometer and cardiac rhythm measured by electrocardiography at the time of echocardiography. EF was measured using the modified 2D Quinones formula or biplane method of disks. LV outflow tract diameter was measured in the parasternal long axis view in early systole from the point of aortic cusp insertion into the interventricular septum to the point of aortic cusp insertion into the intervalvular fibrosa. LV outflow tract time velocity integral was measured using pulsed wave Doppler by placing the sample volume just below the region of flow convergence at approximately 5 mm apically from the aortic valve in the apical long axis view and aligning it parallel with blood flow. LV SV was calculated by the Doppler method (LV outflow tract area×LV outflow tract velocity–time integral measured by pulsed-wave Doppler). An additional measurement of SV by the cube formula (SV=LVEDD3−LVESD3) was calculated for comparison with the Doppler method. A non-imaging probe was routinely used in multiple transducer positions (apical, suprasternal, supraclavicular, subcostal and right parasternal) in order to record the peak aortic jet velocity. The position that yielded the highest aortic valve velocity was used and at least three signals were traced and averaged to determine the time–velocity integral and calculate transvalvular pressure gradient. For patients in atrial fibrillation, 10 cardiac cycles were averaged to obtain the SV and mean aortic pressure gradient.
Afterload assessment
Ventricular afterload was assessed using the methods derived from echocardiography and systolic blood pressure (10). Valvuloarterial impedance (Zva), a measure of global LV afterload, was calculated using the following formula:11 Zva (mm Hg/mL/m2)=(mean systolic aortic valve Doppler gradient+systolic blood pressure)÷SVI. SAC, a measure of pulsatile arterial load, was measured using the formula: SAC (mL mm Hg−1 m−2)=SVI÷(systolic—diastolic blood pressure). Systemic vascular resistance (SVR), a measure of non-pulsatile vascular load, was measured using the formula: SVR (dyne s cm−5)=80×mean blood pressure÷cardiac output.
Clinical outcomes
Symptom onset, need for aortic valve intervention (valvuloplasty, transcatheter or surgical aortic valve replacement (AVR)) and vital status were determined using the medical record.
Statistical analysis
Patients were stratified into quartile groups based on distribution of SVI. Additional comparisons were made with a group of patients with the most commonly used cutpoint for low flow used in the literature, SVI <35 mL/m2. Data are reported as mean±SD or number and percentage for categorical variables. Student's t test was used to compare continuous variables and Fisher exact test to compare categorical variables between individual groups. Analysis of variance was used to compare multiple groups. Pairwise comparisons were performed using a post hoc Bonferroni significance level (p<0.008). Kaplan–Meier analysis with log-rank testing was used for temporal analysis of time to event outcomes in each group. An adjusted survival curve was also created using a semiparametric approach, assuming covariates follow the proportional hazards assumption while not requiring proportional hazards for SVI group. Survival of each group was compared with expected survival for an age and sex-matched Minnesota white population.12 The primary endpoint of interest was all-cause mortality. The secondary endpoint was all-cause mortality censored at the time of AVR. c-Statistics and the Akaike Information Criterion,13 a measure of model fit, were used to compare various SVI cutpoints for predicting overall mortality. A Cox proportional hazards multivariable model with stepwise elimination was used to determine predictors of all-cause mortality. Candidate variables included into the multivariable model included age, sex, body mass index (BMI), SVI, EF, AVA, mean gradient, peak velocity, Zva, SAC, right ventricular systolic pressure, hypertension, coronary artery disease, diabetes mellitus, atrial fibrillation, history of heart failure, prior transient ischaemic attack or stroke, chronic obstructive pulmonary disease, serum creatine, prior coronary artery bypass grafting surgery, and symptomatic status. c-Statistics were used to summarise the discriminatory ability of the new multivariable model compared with standard predictive variables. Difference in c-statistics and 95% CI were calculated and tested using the SE estimated from the 1000 bootstrap samples. The present study had approximately 80% power to detect a HR of 1.9 between two equal sized groups of 200 subjects. Statistical analysis was performed using SAS software V.9.3 and JMP software V.10.0, (Cary, North Carolina, USA). An a priori level of significance was determined at p<0.05.
Results
Out of 14 656 patients with AS undergoing transthoracic echocardiography, 9558 were excluded for AVA >1 cm2, 2231 excluded for reduced EF, 1156 excluded for concomitant moderate valvular lesions and 1299 excluded for mean gradient ≥40 mm Hg. Of 405 patients with LG severe AS and preserved EF, 90 (22%) had SVI <38 mL/m2, 105 (26%) had SVI 38–43 mL/m2, 104 (26%) had SVI 43–48 mL/m2 and 106 (26%) had SVI ≥48 mL/m2. There were 53 (13%) patients with SVI <35 mL/m2. More patients in groups 1 (n=61, 68%) and 2 (n=72, 69%) were symptomatic at the time of initial presentation compared with groups 3 (n=46, 44%) and 4 (n=50, 47%), (p<0.001). Patients with BMI ≥30 kg/m2 were more often symptomatic compared with patients with BMI <30 kg/m2 (65% vs. 53%, p=0.03).
Age was similar among groups, and there was a higher prevalence of women in group 4 compared with the other groups (table 1). Body size was smaller in group 4, with more obesity present in group 1. Hypertension was common in all groups, but most prevalent in group 3. Atrial fibrillation was more common in low SVI groups (1 and 2). There was no difference in the prevalence of other comorbidities between groups including coronary artery disease, chronic pulmonary disease, renal dysfunction, anaemia, heart failure and history of stroke. Diuretic and ACE inhibitor use was more common in groups 1 and 2 compared with other groups.
Characteristics of stroke volume groups in LG severe aortic stenosis with preserved EF
Resting heart rate was higher in groups with lower SVI, but there were no significant differences in blood pressure (table 2). EF was consistently lower and relative wall thickness higher with decreasing SVI, but there were no differences in LV dimensions. Indexed AVA was consistently smaller in the low SVI groups. Peak aortic velocity and mean gradient were lower with decreasing SVI. There were no differences in LV outflow tract diameter, medial E/e’ or estimated right ventricular systolic pressure between groups.
Haemodynamic features according to SVI in LG severe aortic stenosis with preserved EF
Outcomes
Mean follow-up duration was 2.55±1.87 years and 305 (75%) had >1 year of follow-up. During the follow-up period, AVR was performed in 42 patients in group 1, 48 patients in group 2, 45 patients in group 3 and 41 patients in group 4 (2-year estimates: 44%, 39%, 49% and 56%, p=0.17 for AVR among groups). Concomitant coronary artery bypass grafting was performed at the time of AVR in 19 (45%) patients in group 1, 22 (46%) in group 2, 20 (44%) in group 3 and 14 (34%) in group 4 (p=0.42). Death occurred in 34 patients in group 1, 31 patients in group 2, 17 patients in group 3 and 22 patients in group 4 (2-year estimates: 56%, 71%, 82% and 85%, p=0.002).
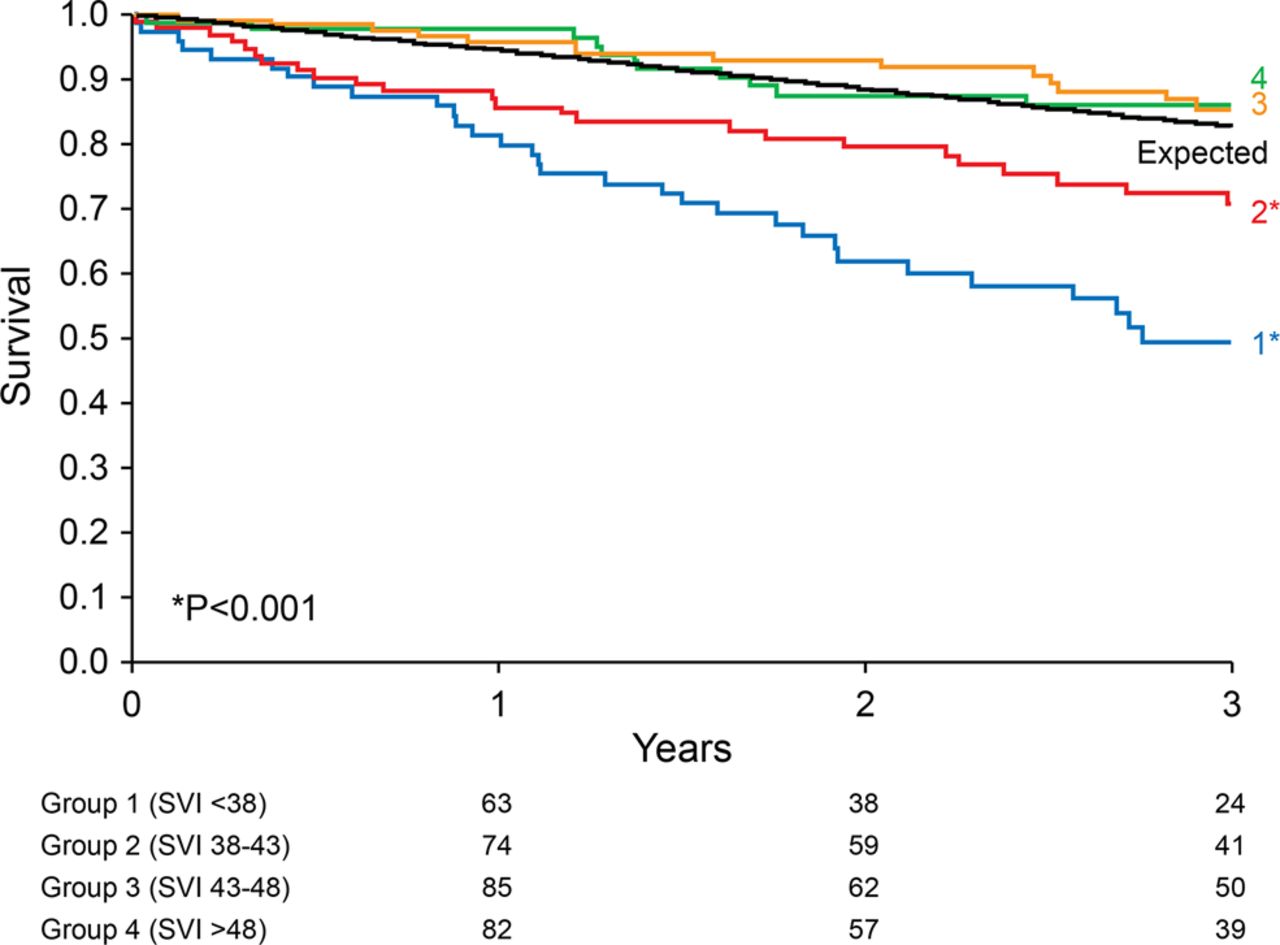
Examination of the residuals from the proportional hazards model showed that SVI as a continuous variable was linearly associated with the risk of death (HR 0.94, 95% CI 0.92 to 0.97, p<0.0001 for every 1 mL/m2 increase in SVI). Overall survival was lowest in group 1 (3-year estimate 54%), followed by group 2 (3-year estimate 70%), group 4 (3-year estimate 80%) and group 3 (3-year estimate 86%) (p=0.002). Compared with an age and sex-matched expected population, group 1 had the poorest survival (3-year estimate 54% vs. 84% expected, p<0.001), group 2 also had reduced survival (3-year estimate 70% vs. 81% expected, p=0.02), and groups 3 and 4 had survival similar to an age and sex-matched group (3-year estimate 86% vs. 80% expected, p=0.33; and 80% vs. 76%, p=0.48, respectively). Adjusted survival is shown in figure 1. To evaluate whether BMI influenced survival in the SVI <43 group, an interaction between BMI and SVI was tested and found to be non-significant (p=0.49). We also noted that the subgroup of patients with BMI <25 kg/m2 and SVI <43 (n=52) had significantly reduced survival compared with that of age and sex-matched controls (3-year estimate 44% vs. 76% expected, p<0.001).

Stroke volume index (SVI) quartiles and adjusted survival. Group 1 (SVI <38 mL/m2) had the lowest survival (3-year estimate 49%), followed by group 2 (SVI 38–43 mL/m2; 3-year estimate 70%), group 4 (SVI >48 mL/m2; 3-year estimate 85%) and group 3 (SVI 43–48 mL/m2; 3-year estimate 86%) (p<0.001). Groups 1 and 2 had reduced survival compared with expected (p<0.001). Survival estimates were computed at the mean of variables in the multivariable model: age (80 years), body mass index (28.3 kg/m2) and right ventricular systolic pressure (39.3 mm Hg).
c-Statistics for SVI <35, SVI <38 and SVI <43 mL/m2 in predicting all-cause mortality were 0.56 (0.52 to 0.61), 0.58 (0.53 to 0.63) and 0.61 (0.56 to 0.66), respectively (table 3). SVI as a continuous variable yielded a c-statistic value of 0.61 (0.55 to 0.67).
SVI cutpoints and overall mortality
Groups 1 and 2 had the poorest survival with medical management (censored at AVR) compared with groups 3 and 4 (3-year estimate 46% and 67% vs. 78% and 73%, respectively, p=0.002) although referral rate for AVR was similar among groups (53%–62% underwent AVR, p=0.57). Thirty-day survival after AVR was excellent in all groups (98±2% in groups 1, 2 and 3, respectively, and 97±3% in group 4, p>0.99).
Univariable and multivariable analysis
Univariable age-adjusted predictors of mortality are shown in table 4. After multivariable analysis, age, BMI, right ventricular systolic pressure and SVI were independent predictors of all-cause mortality (table 4). Using the cube formula-derived SVI, SVI remained predictive of all-cause mortality (HR 0.98 (0.96 to 0.99) p=0.03) and remained a significant predictor of outcome after multivariable analysis (HR 0.98 (0.96 to 0.99) p=0.02). For the secondary endpoint of mortality censored at AVR, multivariable analysis yielded the same independent predictors: age, BMI, right ventricular systolic pressure and SVI (table 5). On comparing the new proposed multivariable model (age, BMI, SVI and RVSP) with a model composed of variables previously shown to be predictive of mortality in AS (age, heart rate, peak aortic velocity, EF and creatine14), the c-statistic for the new model was 0.74 (0.68 to 0.79) while the ‘traditional model’ c-statistic was 0.63 (0.57 to 0.70) (difference in c-statistics: 0.096 (0.030 to 0.161), p=0.004).
Predictors of mortality
Predictors of mortality censored at aortic valve replacement
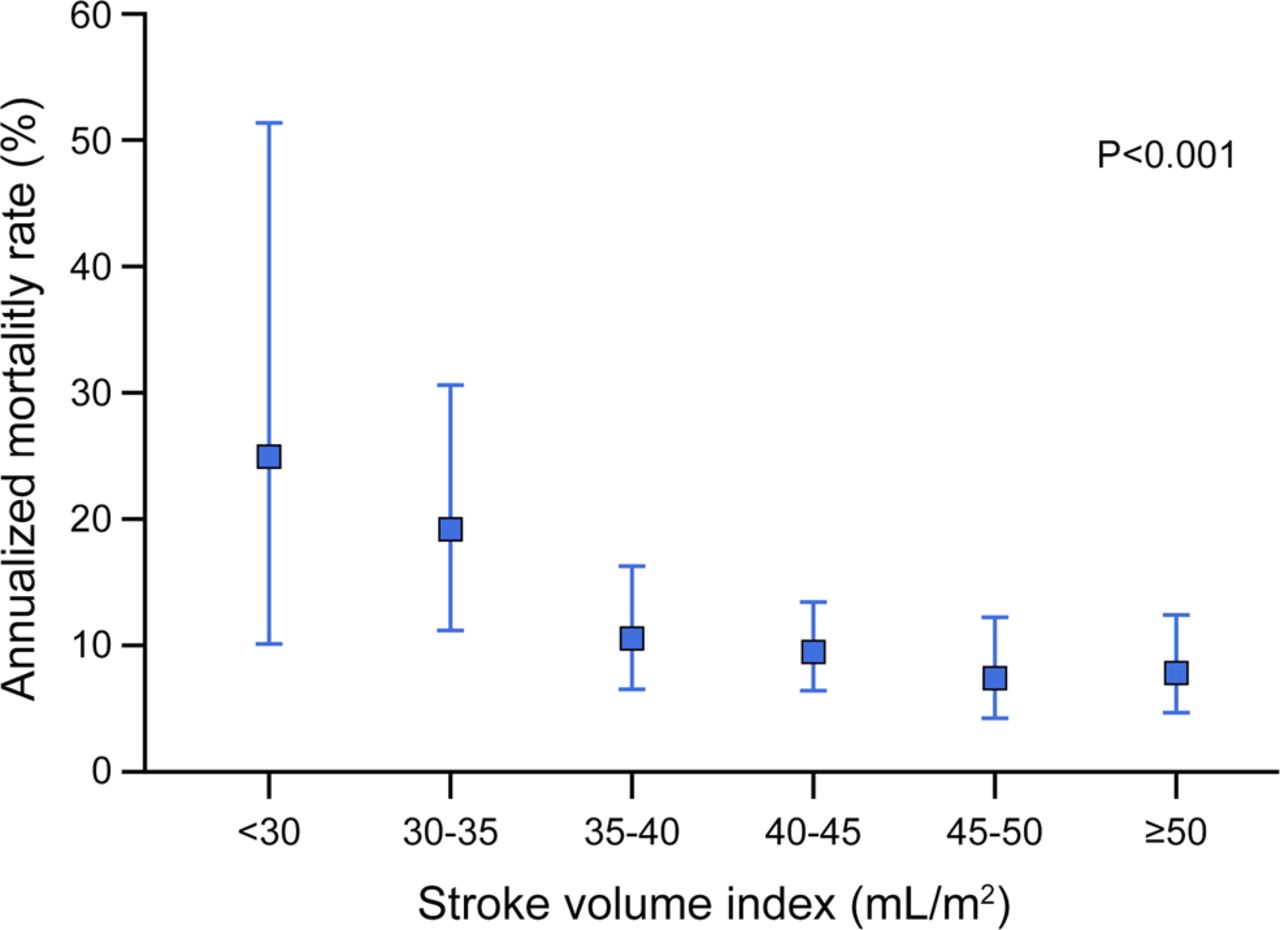
SVI was inversely associated with mortality (HR 1.28 (1.11 to 1.46) per every 5 mL/m2 decrease in SVI). Annualised mortality rates according to SVI in 5 mL/m2 increments are shown in figure 2. Using different SVI cut off points, SVI <35 was associated with highest mortality (HR 2.36 (1.49 to 3.73) p<0.001), followed by SVI <38 (HR 2.09 (1.39 to 3.16) p<0.001) and SVI <43 (HR 2.05 (1.38 to 3.05), p<0.001).

{kind=link}
{kind=link}
Annualised mortality rate according to stroke volume index (SVI). Annualised mortality rate was progressively higher with lower SVI (p<0.001), with highest mortality seen in patients with SVI <35 mL/m2.
Discussion
The principle finding of this analysis is that lower SVI is incrementally associated with mortality, thus providing ‘real-world’ range and clinical applicability to a single threshold for SVI that has been arbitrarily chosen for patients with LG severe AS and preserved EF. The presence of low flow defined as SVI <35 mL/m2 in patients with LG severe AS with preserved EF has been shown to predict a poor prognosis, especially when these patients are managed conservatively without AVR.1–5 ,8 In the present study, SVI <43 and <35 mL/m2 were independently and incrementally associated with increased mortality in patients with LG severe AS with preserved EF. The finding of a sharp rise in increased mortality when SVI reaches ≤35 mL/m2 lends support to the current definition of low flow proposed in recent valvular heart disease guidelines.15 ,16 However, there were many patients with SVI of 35–43 mL/m2 who were also at increased risk compared with a ‘normal flow’ population; these findings may further aid in the process to individualise the care of the AS patient. Although the presence of a low-flow state is associated with reduced survival in AS patients with preserved EF, these lower-flow patients have a referral rate for AVR similar to normal SVI patients. These data underscore the need to improve risk stratification with a new emphasis on incorporation of SVI into algorithms, particularly as we face a growing population of elderly patients with calcific AS.
The inverse association of SVI with mortality, particularly in patients with SVI <43 mL/m2, may be explained by multiple underlying mechanisms. Similar to a recent invasive study,17 arterial afterload was more abnormal in patients with reduced SV and may independently predict adverse cardiovascular events in patients with AS.4 ,18 Furthermore, patients with lower SVI also had a lower EF, a finding that has been linked with reduced survival in AS19 and may contribute to the observed relationship between SVI and survival. Although all patients had an EF ≥50%, studies of longitudinal strain in similar populations have shown that some may have abnormal systolic function.20 Although LV dimensions were no different between groups, relative wall thickness was higher in the low SVI groups, suggesting a greater degree of concentric remodelling which is also associated with reduced LV systolic function.21 Similar observations of a predisposition towards concentric remodelling and reduced longitudinal function in low flow LG severe AS with preserved EF have recently been replicated.22
A recent study showed that AVR improved survival in LG severe AS patients with both SVI <35 and ≥35 mL/m2.23 The survival benefit of AVR with SVI ≥35 mL/m2 may be explained by: (1) all patients in the study were symptomatic and (2) some with SVI ≥35 mL/m2 and LG may still be at higher risk, as demonstrated in the present study. Although different cutpoints of SVI were not explored, these results are consistent with our analysis that considering SVI as a continuous variable that has a graded association with survival may be helpful in estimating risk and potential benefit from AVR. Studies of high-risk AS patients undergoing transcatheter AVR have demonstrated that SVI is predictive of both early and late mortality following transcatheter AVR, suggesting that SVI should also be incorporated into risk algorithms in the high-risk subset of AS patients.24 ,25
Lower SVI (SVI <43 mL/m2) was associated with a higher prevalence of atrial fibrillation and previous heart failure episodes. Atrial fibrillation may contribute to lower SVI by both the reduction in diastolic filling time and loss of atrial systolic contribution, as well as increased neurohumoral activation. Heart failure with preserved EF is associated with atrial fibrillation, reduced SVI and peripheral arterial abnormalities; thus, it is not surprising that 20% of patients in the low SVI groups had previous episodes of heart failure. Unique baseline cardiovascular abnormalities (high arterial afterload, reduced LV function and predisposition to heart failure) may leave this population more vulnerable to the additional afterload of a calcified stenotic aortic valve, and thus may explain why they derive more clinical benefit from AVR than patients with normal SVI LG severe AS with preserved EF.8 ,17
A previous study highlighted the poor prognosis associated with coexistent severe pulmonary hypertension and severe AS;26 however, the present analysis adds to this understanding by showing that any degree of pulmonary hypertension increases risk in the LG AS population with preserved EF. Pulmonary hypertension in this group is likely a reflection of more advanced left heart disease and/or pulmonary disease, serving as an added clinical risk prediction tool. Higher BMI was associated with more favourable survival, which may be due to multiple factors surrounding the obesity paradox phenomenon.27 Additionally, patients with BMI >30 kg/m2 were more likely to have symptoms which may have impacted referral for AVR.
Limitations
While the retrospective nature is an inherent limitation, this study represents a large series of consecutive patients with LG severe AS and preserved EF who underwent comprehensive echocardiography and stringent clinical follow-up. Although many baseline variables were known, there may be features of the patient groups not accounted for which contributed to differences in outcomes. This study is unique in that it explores the relationship between SVI and mortality in patients with LG severe AS using a systematic AS measurement methodology that is consistently performed at our institution.
Conclusions
Lower SVI is incrementally associated with mortality in LG severe AS with preserved EF. SVI ≤35 mL/m2 was associated with the highest mortality, while SVI <38 and <43 mL/m2 were also associated with increased risk. These findings have implications for classification of AS severity, identification of high-risk groups and subsequent management.
Key messages
What is already known on this subject?
-
Low-gradient (LG) severe aortic stenosis (AS) and preserved EF with reduced stroke volume index (SVI) are associated with an adverse prognosis.
What might this study add?
-
Lower SVI is incrementally associated with mortality in LG severe AS with preserved EF. In addition to SVI <35 mL/m2, SVI <38 and <43 mL/m2 are also associated with increased mortality and are independent predictors of mortality.
How might this impact on clinical practice?
-
These data underscore the need to improve risk stratification of patients with AS with a new emphasis on incorporation of SVI into algorithms, particularly as we face a growing population of elderly patients with calcific AS. The data from this analysis support the use of SVI as a continuous variable and that in addition to SVI <35 mL/m2, SVI of 35–43 mL/m2 may also identify a higher risk group.
References
Footnotes
-
Contributors All authors contributed significantly to the completion of the study and the manuscript, including reading and approval of the manuscript in its current form.
-
Funding Funding was provided by the Cardiovascular Research Division, Mayo Clinic, Rochester, Minnesota, USA. This publication was supported by NIH/NCRR CTSA Grant Number UL1 RR024150. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH.
-
Competing interests None.
-
Ethics approval Mayo Clinic Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.