Article Text

Abstract
Objective To investigate the association between regular coffee consumption and the prevalence of coronary artery calcium (CAC) in a large sample of young and middle-aged asymptomatic men and women.
Methods This cross-sectional study included 25 138 men and women (mean age 41.3 years) without clinically evident cardiovascular disease who underwent a health screening examination that included a validated food frequency questionnaire and a multidetector CT to determine CAC scores. We used robust Tobit regression analyses to estimate the CAC score ratios associated with different levels of coffee consumption compared with no coffee consumption and adjusted for potential confounders.
Results The prevalence of detectable CAC (CAC score >0) was 13.4% (n=3364), including 11.3% prevalence for CAC scores 1–100 (n=2832), and 2.1% prevalence for CAC scores >100 (n=532). The mean ±SD consumption of coffee was 1.8±1.5 cups/day. The multivariate-adjusted CAC score ratios (95% CIs) comparing coffee drinkers of <1, 1–<3, 3–<5, and ≥5 cups/day to non-coffee drinkers were 0.77 (0.49 to 1.19), 0.66 (0.43 to 1.02), 0.59 (0.38 to 0.93), and 0.81 (0.46 to 1.43), respectively (p for quadratic trend=0.02). The association was similar in subgroups defined by age, sex, smoking status, alcohol consumption, status of obesity, diabetes, hypertension, and hypercholesterolaemia.
Conclusions In this large sample of men and women apparently free of clinically evident cardiovascular disease, moderate coffee consumption was associated with a lower prevalence of subclinical coronary atherosclerosis.
Statistics from Altmetric.com
Introduction
The effect of coffee consumption on cardiovascular health has remained controversial.1 In spite of earlier concerns about a potential increase in cardiovascular disease (CVD) risk associated with coffee consumption, a recent meta-analysis of 36 prospective studies showed that moderate coffee consumption was associated with a decreased risk of CVD, with the strongest reduction at 3–5 cups/day.2 Coffee consumption has been associated with improved insulin sensitivity,3–5 reduced low density lipoprotein cholesterol (LDL-C) oxidation,6 ,7 and reduced risk of type 2 diabetes.8 ,9 However, coffee consumption has also been associated with increased cholesterol concentrations10 ,11 and acute pressor effects, although the relationship of coffee consumption to the risk of hypertension is still unclear.1
Coronary artery calcium (CAC) detected by cardiac CT is a subclinical marker of coronary atherosclerosis that predicts future coronary heart disease (CHD)12 in a wide range of ages, including asymptomatic young adults.13 CAC provides information on underlying pathologic changes in coronary arteries and thus allows for a detailed assessment of the early stages of CVD, which is distinct from the occurrence of plaque rupture and thrombosis in clinical events.14 Only two studies have examined the relationship between coffee consumption and CAC, with inconsistent results.15 ,16 We therefore examined the association between coffee consumption and the presence of CAC in a large sample of asymptomatic men and women attending a health screening examination.
Methods
Study population
The Kangbuk Samsung Health Study is a cohort study of Korean men and women who underwent comprehensive annual or biennial examinations at the Kangbuk Samsung Hospital Total Healthcare Centers in Seoul or Suwon, South Korea.17 The population for this cross-sectional analysis included all participants (n=30 485) who completed a food frequency questionnaire (FFQ) and who underwent a comprehensive health screening examination including cardiac CT for CAC scoring between March 2011 and April 2013. Annual or biennial health screening examinations are widely performed in Korea, as health examinations are mandatory for all workers under the Industrial Safety and Health Law. CAC scoring has become a common CVD screening test in Korea.17 After participants had completed self-administered questionnaires, all examinations including CT scan for CAC scoring were performed.
We excluded 437 participants with a history of CVD, 474 participants who had implausible estimated energy consumption levels (beyond 3 SDs from the loge-transformed mean energy consumption), 1824 participants with missing information on coffee consumption, and 3371 participants with missing information on smoking status. The final sample size for the analysis was 25 138 participants (figure 1).

Flow diagram of the included study participants. CAC, coronary artery calcium.
This study was approved by the Institutional Review Board of the Kangbuk Samsung Hospital. The requirement of informed consent was waived because we used non-identified retrospective data routinely collected during the health screening process.
Assessment of coffee consumption
Usual dietary consumption was assessed using a 103-item self-administered FFQ designed for use in Korea.18 The reproducibility and validity of the nutrient information provided by this FFQ have been evaluated among 124 Korean subjects aged 40–70 years. Participants were asked how often, on average, they consumed each type of food or beverage during the past year. The FFQ had three predefined categories of portion size, ranging from small to large, and nine predefined categories of frequency, ranging from never or seldom to ≥ three times per day for foods, and from never or seldom to ≥ five times per day for beverages. Participants were also asked to report the consumption period (ie, 3, 6, 9, or 12 months) for seasonal consumption of fruits. The FFQ asked about total coffee consumption without differentiating between caffeinated and decaffeinated coffee. However, decaffeinated coffee is not yet widely popular in Korea.19 A recipe, portion size, and nutrient database was constructed with a food composition table from the Korean Nutrition Society.20
Measurement of CAC
All CT scans were obtained with a Lightspeed VCT XTe 64 slice multidetector CT (MDCT) scanner (GE Healthcare, Tokyo, Japan) with a standard scanning protocol using 2.5 mm thickness, 400 ms rotation time, 120 kV tube voltage, and a 124 mAS (310 mA×0.4 s) tube current under ECG-gated dose modulation. Quantitative CAC scores were calculated using the method proposed by Agatston et al.21 The interobserver and intraobserver reliability values of CAC scores were both excellent, with intraclass correlation coefficients of 0.99. If more than one CAC measurement was available for a participant during the study period, the initial measurement was used.
Assessment of other variables
Data on medical history, medication use, family history, physical activity, alcohol consumption, smoking habits, and sociodemographic characteristics were collected through a self-administered questionnaire, whereas the anthropometric parameters and blood pressure were measured by trained staff during the health examinations.17 Physical activity levels were assessed by the Korean-validated version of the short form of the International Physical Activity Questionnaire (IPAQ); participants were classified as inactive, minimally active, and health enhancing physically active (HEPA).22 Hypertension was defined as systolic blood pressure (SBP) ≥140 mm Hg, diastolic blood pressure ≥90 mm Hg, a participant report of a previous diagnosis, or current antihypertensive medication use.
Blood specimens were sampled from the antecubital vein after at least a 10 h fast. Measurements of serum biochemical parameters, including serum concentrations of glucose, haemoglobin A1c (HbA1c), total cholesterol, triglycerides, LDL-C, high density lipoprotein cholesterol (HDL-C), and serum high sensitivity C reactive protein (hsCRP) have been described in detail elsewhere.17 Diabetes mellitus was defined as fasting serum glucose ≥126 mg/dL, HbA1c ≥6.5%, self-report of a previous diagnosis, or use of blood glucose lowering agents. Hypercholesterolaemia was defined as a serum total cholesterol ≥240 mg/dL, self-report of a previous diagnosis, or current use of cholesterol lowering medication. The Laboratory Medicine Department at Kangbuk Samsung Hospital has been accredited by the Korean Society of Laboratory Medicine and participates annually in inspections and surveys by the Korean Association of Quality Assurance for Clinical Laboratories and the College of American Pathologists Proficiency Testing programme.
Statistical analysis
Habitual coffee consumption was categorised as none, <1, 1–<3, 3–<5, and ≥5 cups/day. For the primary analyses, we modelled loge(CAC score+1) using robust Tobit regression model with the Huber-White estimation of SEs.14 We loge-transformed the CAC scores since their distribution was skewed to the right and used Tobit models because the CAC scores were left-censored at 0 Agatston units (non-detectable CAC scores). Tobit models were used to estimate CAC score ratios and their 95% CIs for each category of coffee consumption. CAC score ratios represent the ratio of the geometric means of CAC scores comparing each category of coffee consumption to the group with no coffee consumption. In a secondary analyses, we categorised CAC scores as a dichotomous variable (CAC score >0 compared with CAC score 0) and used logistic regression to estimate the ORs for detectable CAC according to the categories of coffee consumption.
Statistical models were initially adjusted for age, sex, centre, and year of screening examination (model 1) and then further adjusted for potential confounding factors determined a priori,23 including education level (high school graduate or less, community college or university graduate, graduate school or higher, and unknown), physical activity level (inactive, minimally active, HEPA, and unknown), smoking status (never, former, and current), BMI (body mass index, kg/m2), parental history of CHD (yes vs no), alcohol consumption (none, <5, 5–<20, ≥20 g/day, and unknown), total energy consumption (kcal/day), and consumption of fruits, vegetables, and red and processed meats (quartiles, g/day) (model 2). Further adjusting for tea consumption (including black, green tea, and any other teas) did not materially change the results. We additionally adjusted for potential intermediate variables, including SBP, fasting serum glucose, total cholesterol, triglycerides, and HDL-C (model 3). We conducted quadratic trend tests by including linear and quadratic terms of the median coffee consumption within each coffee consumption category as continuous variables in the regression models, and statistical significance was evaluated using Wald tests.
We conducted subgroup analyses by age (<40 vs ≥40 years), sex (men vs women), smoking (non-current vs current smoker), BMI (<25 vs ≥25 kg/m2), alcohol drinking (non-drinker vs drinker), diabetes (yes vs no), hypertension (yes vs no), and hypercholesterolaemia (yes vs no). We tested for statistical interactions by using Wald tests for the product term of coffee consumption categories with the stratification variable.
In sensitivity analyses, we repeated the multivariate analyses after excluding those who did not consume coffee because of the possibility that they could represent individuals with unfavourable health conditions, and each category was compared with the reference category of coffee drinkers of <1 cup/day. All analyses were conducted using STATA V.12.1 (Stata Corp, College Station, Texas, USA). Statistical tests were a two-sided test, and p<0.05 was considered statistically significant.
Results
The average ±SD age of study participants was 41.3±7.5 years, and 83.7% of participants were male. The prevalence of CAC scores >0 was 13.4% (n=3364), including 11.3% prevalence for CAC scores 1–100 (n=2832), and 2.1% prevalence for CAC scores >100 (n=532). The mean ±SD consumption of coffee was 1.8±1.5 cups/day. Compared with non-coffee drinkers, individuals in the highest categories of coffee consumption were more likely to be older, men, and current smokers and to have higher education, less frequent vigorous-intensity physical activity, obesity, and hypercholesterolaemia, and to have a lower proportion of hypertension (table 1). Compared to non-coffee drinkers, those with high coffee consumption also had higher concentrations of fasting serum glucose, HbA1c, total cholesterol, triglycerides, and LDL-C, and lower HDL-C and SBP, and they had a higher consumption of total energy, red and processed meats, alcohol, and a lower consumption of fruits and vegetables.
Characteristics of study participants by categories of coffee consumption
In a model that adjusted for age, sex, centre, and year of screening examination (table 2; model 1), the CAC ratios (95% CI) comparing coffee drinkers of <1, 1–<3, 3–<5, and ≥5 cups/day to non-coffee drinkers were 0.86 (0.55 to 1.34), 0.82 (0.53 to 1.26), 0.78 (0.50 to 1.22), and 1.77 (0.66 to 2.06), respectively (p for quadratic trend=0.20). Further adjusting for potential confounders strengthened the inverse association between coffee consumption and CAC, most likely due to smoking status. In multivariable adjusted models (model 2), the corresponding estimates were 0.77 (0.49 to 1.19), 0.66 (0.43 to 1.02), 0.59 (0.38 to 0.93), and 0.81 (0.46 to 1.43), respectively (p for quadratic trend=0.02). The findings were similar after adjustment for SBP, fasting serum glucose, total cholesterol, triglycerides, and HDL-C (model 3).
Coronary artery calcium (CAC) score ratios* (95% CIs) by categories of coffee consumption
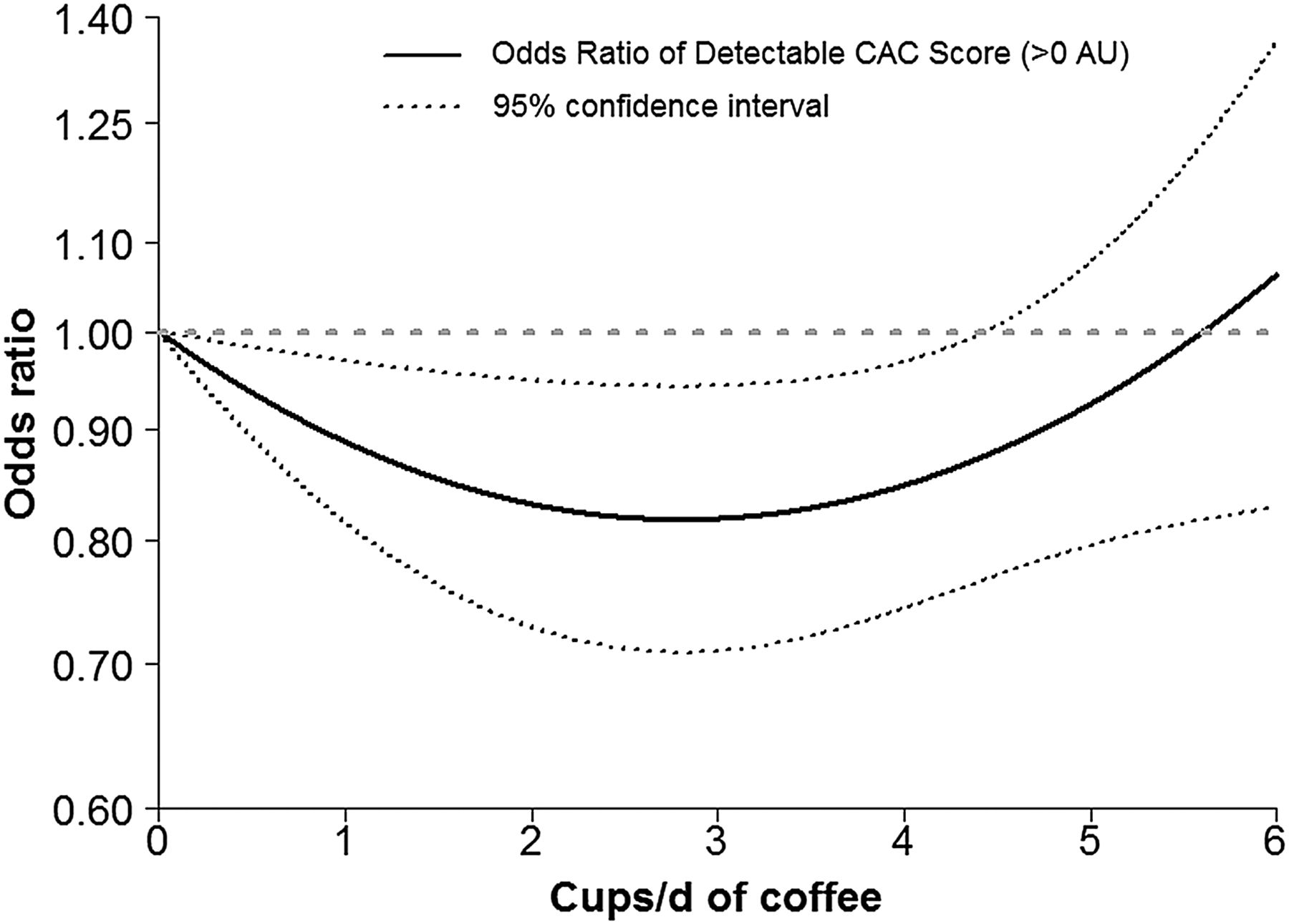
The results from logistic regression models using categories of CAC scores were consistent with the Tobit models. The multivariable adjusted ORs (95% CIs) for CAC score >0 comparing coffee drinkers of <1, 1–<3, 3–<5, and ≥5 cups/day to non-coffee drinkers were 0.90 (0.74 to 1.10), 0.85 (0.71 to 1.03), 0.80 (0.66 to 0.97), and 0.94 (0.73 to 1.20), respectively (p for quadratic trend=0.02) (table 3, model 2), with little change after adjustment for potential intermediate variables. The significant quadratic trend between coffee consumption and detectable CAC scores was also evident after adjusting for potential confounders (figure 2).
OR* (95% CIs) for the presence of coronary artery calcium (CAC) score by categories of coffee consumption

{kind=link}
{kind=link}
OR of detectable coronary artery calcium scores (CAC score >0) by coffee consumption. The curves represent the adjusted OR of detectable CAC scores ( >0 Agatston unit) and coffee consumption. The dose response association of coffee consumption was estimated by using a linear and a quadratic term for coffee consumption in the multivariable logistic regression. The model adjusted for age, sex, centre, and year of screening examination, education level (high school graduate or less, community college or university graduate, graduate school or higher, and unknown), physical activity level (inactive, minimally active, health enhancing physically active, and unknown), smoking status (never, former, and current), body mass index (kg/m2), parental history of coronary heart disease (yes vs no), alcohol consumption (none, <5, 5–<20, ≥20 g/day, and unknown), total energy consumption (kcal/day), and consumption of fruits, vegetables, and red and processed meats (quartiles, g/day). A similar trend was observed in robust Tobit regression models of CAC ratios.
The association was consistent in subgroup analyses, and there were no statistically significant interactions (data not shown; p for interaction >0.05). In sensitivity analyses where we excluded non-coffee drinkers, the multivariable adjusted CAC score ratios (95% CIs) comparing coffee drinkers of 1–<3, 3–<5, and ≥5 cups/day to coffee drinkers of <1 cup/day were 0.86 (0.68 to 1.09), 0.77 (0.59 to 1.00), and 1.04 (0.67 to 1.62), respectively (model 2).
Discussion
In this large sample of Korean men and women apparently free of clinically evident CVD, coffee consumption was associated with a lower prevalence of CAC, a marker of subclinical coronary atherosclerosis. The association was U-shaped, with participants drinking 3–<5 cups/day having the lowest prevalence of subclinical coronary atherosclerosis. The association was similar after adjustment for cardiovascular risk factors or potential mediators. Our findings are consistent with a recent body of literature showing that moderate coffee consumption may be inversely associated with cardiovascular events.
The relationship between coffee consumption and CVD has been extensively investigated with conflicting results. However, several large prospective studies and reviews have concluded that habitual coffee consumption is associated with decreased risk of cardiovascular events, and this association was most evident for moderate coffee consumption levels.9 ,24–26 A recent meta-analysis of 36 prospective studies also showed that moderate coffee consumption was associated with decreased CVD risk, with the largest reduction at 3–5 cups/day.2
Long term coffee consumption was associated with improved endothelial function.27 Only two studies, however, have investigated the association between coffee consumption and CAC.15 ,16 In the Rotterdam study (n=1570),15 a moderate (>3–4 cups/day) to high coffee (>4 cups/day) consumption was associated with a decreased prevalence of a CAC score >400 compared with ≤3 drinks/day in women, but an increased risk was observed in non-smoking men. In the Coronary Artery Risk Development in Young Adults (CARDIA) study (n=5115),16 caffeinated and decaffeinated coffee consumption was not associated with coronary calcification or with progression over 5 years of follow-up. In the Rotterdam and CARDIA studies,15 ,16 measurements of coffee intake were taken several years before CAC measurements (an average of 7 years in the Rotterdam Study and at least 8 years in CARDIA), which may have induced misclassification of exposure status. In our study, coffee consumption was assessed on the same day of the screening exam or in the previous 14 days, minimising misclassification of exposure and avoiding biased reporting as dietary information was collected before CAC measurements. The inconsistent findings across studies could also be attributable to other methodological issues, including differences in sample size, control for potential confounding factors, measures of coffee consumption, study population (age, ethnicity, and sex composition), or prevalence of CAC.
Although none of the potential mediating variables fully explained the relationship between coffee and the presence of CAC, several mechanisms have been suggested for the association between moderate coffee and cardiovascular risk. Chronic coffee consumption has been associated with reduced risk of type 2 diabetes,8 ,9 a strong risk factor for atherosclerosis. In addition, coffee drinking might improve insulin sensitivity and β-cell function, presumably due to the presence of antioxidant compounds in the coffee.3–5 Although acute coffee consumption might increase blood pressure, this effect seems to disappear with chronic coffee consumption and large prospective studies do not support the hypothesis that high coffee consumption increases the risk of hypertension.1 In our data, we observed an inverse relationship between regular coffee consumption and SBP, but adjusting for SBP and other CVD risk factors did not materially change the association between coffee consumption and the presence of CAC. Coffee also contains phenolic compounds with high antioxidant activity that might prevent LDL-C oxidation,6 ,7 and coffee consumption was inversely associated with markers of inflammation28 and endothelial dysfunction.29 On the other hand, coffee, particularly unfiltered coffee, has shown a cholesterol raising effect.10 ,11 Further research is needed to understand the potential effects of moderate coffee consumption on CVD risk, which are likely to be complex and at least partly independent of traditional CVD risk factors.
The present study has several limitations. First, the cross-sectional design limits the possibility of establishing causal inferences as we cannot rule out reverse causation or residual confounding. However, we examined the association in asymptomatic individuals free of reported CVD and used as outcome CAC, a marker of subclinical disease not recognised by study participants. Furthermore, the estimates did not change after adjusting for a variety of CVD risk factors or after excluding non-coffee drinkers who might abstain from coffee drinking due to unfavourable health status. Second, exposure assessment of coffee and other lifestyle factors was based on self-report and subject to measurement error, which would tend to attenuate the observed associations. Third, we were unable to differentiate between caffeinated and decaffeinated coffee. Decaffeinated coffee, however, is not popular among Koreans.19 In addition, a previous study did not show substantial differences in the association between caffeinated and decaffeinated coffee and CAC.16 Finally, our results were based on a sample of relatively healthy, young and middle-aged, educated Koreans, and might not be generalisable to other populations.
Our study also has several strengths. The large sample size provides sufficient power to detect the association between coffee drinking and CAC scores while controlling for a wide range of potential confounders. Data collection in the Kangbuk Samsung Health Study is subject to careful standardisation and quality control. Also, we had information on a large number of CVD risk factors that could be used to adjust for potential confounders in multivariable models.
In conclusion, we found that moderate daily coffee consumption was associated with decreased prevalence of CAC in a large sample of asymptomatic adults free of CVD. Our study adds to a growing body of evidence suggesting that coffee consumption might be inversely associated with CVD risk. Further research is warranted to confirm our findings and establish the biological basis of coffee's potential preventive effects on coronary artery disease.
Key messages
-
What is already known on this subject?
-
The relationship between coffee consumption and cardiovascular disease is controversial. Several large prospective studies and reviews have concluded that habitual coffee consumption may be associated with decreased risk of cardiovascular events, and this association was most evident for moderate coffee consumption levels.
-
What might this study add?
-
In this large sample of Korean men and women free of clinically evident cardiovascular disease, coffee consumption was associated with a lower prevalence of coronary artery calcium, a marker of subclinical coronary atherosclerosis. The association was U-shaped, with participants drinking 3–<5 cups/day having the lowest prevalence of subclinical coronary atherosclerosis.
-
How might this impact on clinical practice?
-
Moderate daily coffee consumption was inversely associated with subclinical coronary atherosclerosis. Large scale and randomised controlled studies are needed to prove causation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Press release
Files in this Data Supplement:
Footnotes
-
Contributors All authors were involved in the preparation of the manuscript, have read the manuscript, agree with the analyses of the data and the conclusions reached in the manuscript, and are accountable for all aspects of the work.
-
Competing interests None.
-
Patient consent Requirement for informed consent was waived because the study used non-identified retrospective data routinely collected during health screening process.
-
Ethics approval Ethics approval was provided by the Institutional Review Board of the Kangbuk Samsung Hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.