Article Text

Abstract
Objectives Recently published clinical guidelines recommend cardiac resynchronisation therapy (CRT) for patients with heart failure (HF) with reduced LVEF and non-left bundle branch block (non-LBBB) QRS morphology. We sought to define the potential benefit of CRT in these patients through meta-analysis of randomised controlled trials (RCTs) that have reported outcomes in patients with non-LBBB QRS morphology.
Methods We searched MEDLINE and EMBASE for RCTs of CRT that reported outcomes according to QRS morphology. We performed meta-analysis of these RCTs to assess the effect of CRT on the end points of death, HF hospitalisation, and the composite of death and HF hospitalisation.
Results Five RCTs were analysed, including 6523 participants (1766 with non-LBBB QRS morphology). CRT was not associated with a reduction in death and/or HF hospitalisation in subjects with non-LBBB QRS morphology (HR 0.99 95% CI 0.82 to 1.20).
Conclusions CRT is not associated with a reduction in death or HF hospitalisation in patients with non-LBBB QRS morphology. Wide QRS with non-LBBB morphology remains an area of uncertainty for CRT, which is included in the recent European Society of Cardiology guidelines with a weaker strength of recommendation, but is not supported by a dedicated RCT.
Statistics from Altmetric.com
Video abstract
Introduction
Several randomised controlled trials (RCTs), initially in patients with severe symptoms,1–3 and more recently in those with mild symptoms,4–6 have proven the efficacy of cardiac resynchronisation therapy (CRT) to reduce morbidity and mortality in patients with heart failure (HF) with LV systolic dysfunction and prolonged QRS duration. The benefit of CRT in patients with LVEF <35% and left bundle branch block (LBBB) QRS morphology is well established,7 and this is reflected in the 2013 European Society of Cardiology (ESC) guidelines on cardiac pacing and CRT which give a strong recommendation (Class I) for CRT in patients with LBBB.8 However, a systematic review9 and meta-analysis7 of RCTs suggested a lack of benefit for CRT in patients with non-LBBB QRS morphology (ie, right bundle branch block (RBBB) or non-specific intraventricular conduction delay (NIVCD)). Furthermore, a recent retrospective analysis of over 24 000 Medicare patients with a CRT defibrillator demonstrated worse outcomes in patients with non-LBBB QRS morphology compared with those with LBBB.10
The 2013 ESC guidelines give a Class IIa, Level B recommendation for CRT in patients with non-LBBB QRS morphology and QRS duration >150 msec, and a weaker recommendation (Class IIb, Level B) for patients with non-LBBB QRS morphology with QRS duration 120–150 msec; both recommendations are for patients with LVEF <35% and New York Heart Association (NYHA) class II–IV symptoms.8 Most recently, an updated technology appraisal of CRT and implantable cardioverter defibrillators (ICDs) published in the UK in June 2014 by the National Institute for Health and Care Excellence (NICE) continues to recommend CRT in patients with LVEF <35% and non-LBBB QRS morphology with QRS duration >150 msec (all NYHA classes), as well as patients with QRS duration 120–149 msec with severe symptoms (NYHA class IV).11 Since the original meta-analysis,7 further CRT studies have been published in more contemporary cohorts.12–15 Given that the new recommendations from NICE have been made after publication of these analyses we sought to perform a contemporary meta-analysis of RCTs to assess the impact of CRT on death and HF hospitalisation in patients with non-LBBB QRS morphology.
Methods
Study eligibility
Studies were considered for inclusion if they evaluated the use of CRT in participants with non-LBBB or RBBB QRS morphology and evaluated mortality or HF hospitalisation. Single arm studies, case reports, case series, letters and editorials were excluded but relevant reviews were retrieved to identify additional studies.
Search strategy
Our search was carried out using the Ovid SP interface covering MEDLINE and EMBASE from inception until August 2014. The exact search terms were “cardiac resynchronization therapy” AND (“right bundle branch block” OR “non-left bundle branch block”).
Two reviewers (MAK and FZA) independently checked retrieved titles and abstracts for eligibility, and the relevant abstracts were checked by the other reviewers (CSK and MAM). Finally, two reviewers hand-searched bibliographies of included studies, as well as full-text review articles identified from the search (MAK and FZA).
Data extraction
Two reviewers (MAK and FZA) extracted data on study design, patient characteristics, treatment, follow-up, results and performed quality assessment of included studies. This was checked by the other reviewers (CSK and MAM).
Data synthesis
RevMan 5.1.6 (Nordic Cochrane Centre) was used to conduct random effects meta-analysis using inverse variance method for mean difference. The random effects model was used because it considers study heterogeneity when generating an average estimate. Statistical heterogeneity was evaluated through the I2 statistic with values of 30–60% representing moderate heterogeneity.16 We performed sensitivity analysis excluding studies that were RBBB only and performed additional meta-regression considering the effect of the start year of the trials, and another based on the mean year across the duration of the trials for analyses with more than two studies.
Validity assessment
Validity assessment was performed by considering use of blinding, outcome ascertainment, baseline differences, loss to follow-up and selective reporting. A subjective overall risk of bias was also assigned for each study based on these factors. In addition, we planned to conduct asymmetry testing for publication bias provided that there were >10 studies in the meta-analysis, and if statistical heterogeneity was <50%.17
Results
Study selection process
Our search of MEDLINE and EMBASE yielded 337 results. After review of all titles and abstracts and full papers of relevant studies, five trials met the inclusion criteria: Cardiac Resynchronization—Heart Failure (CARE-HF),1 ,18 Comparison of Medical Therapy, Pacing and Defibrillation in Heart Failure (COMPANION),2 Resynchronization-Defibrillation for Ambulatory Heart Failure Trial (RAFT),4 ,12 Multicentre Automatic Defibrillator Implantation Trial with Cardiac Resynchronization Therapy (MADIT-CRT),5 ,15 ,20 and Resynchronization Reverses Remodelling in Systolic Left Ventricular Dysfunction (REVERSE).6 ,14 These results are shown in figure 1.
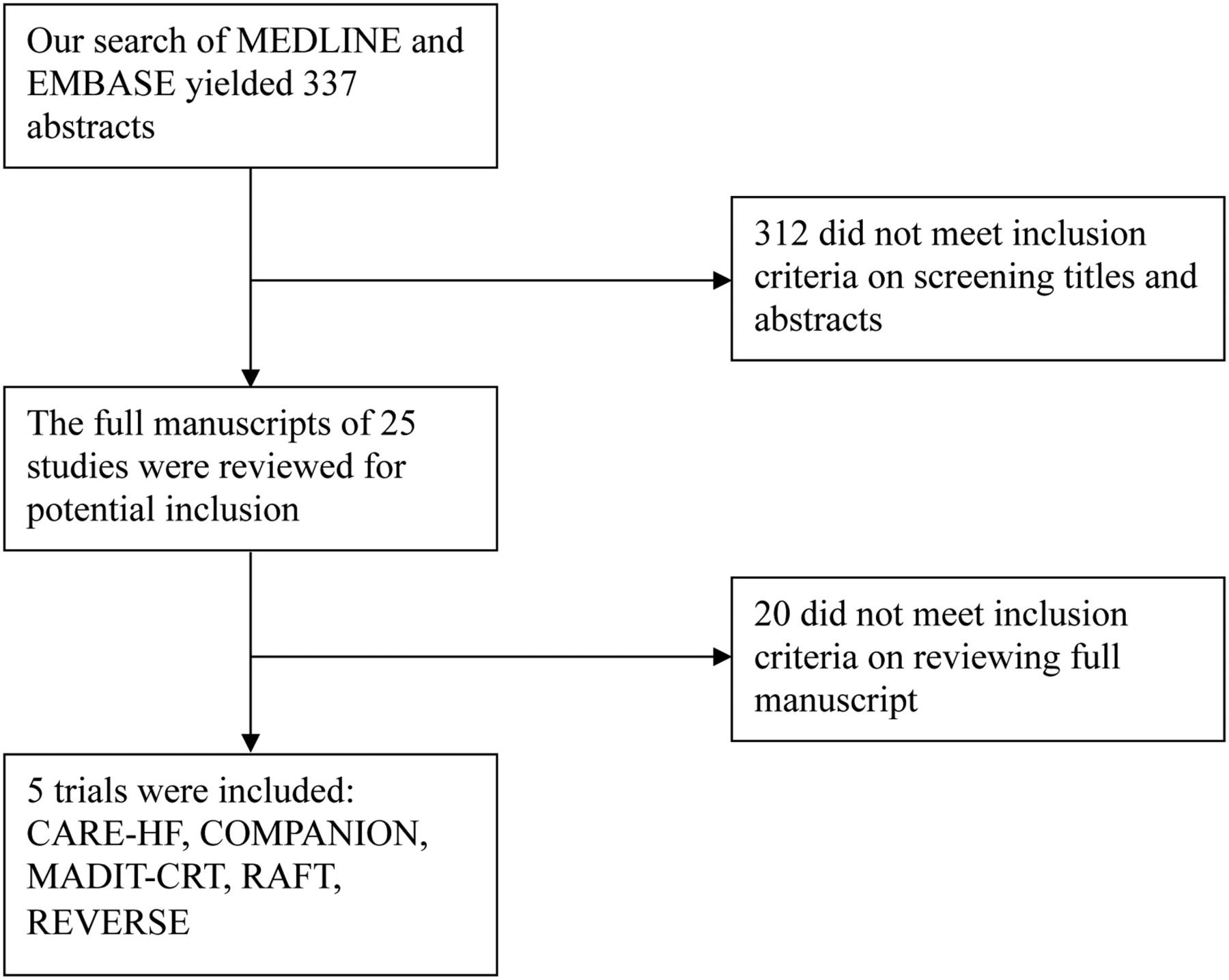
Study selection process.
Participant characteristics
Five RCTs were included. These trials evaluated participants from USA, Canada, Europe, Turkey and Australia between January 2000 and September 2013. The sample size of these trials ranged from 610 participants to 1820 participants, and there was a total of 6523 participants of whom 1766 had non-LBBB. The mean age of participants across all five studies was 65 years and 75% of participants were male. These results are shown in table 1.
Study design, participants and inclusion criteria for patients with non-LBBB QRS morphology who did or did not receive CRT
Two of the five trials evaluated participants who had NHYA class III or IV symptoms (CARE-HF1, COMPANION2). Two trials evaluated NHYA class I or II (MADIT-CRT5, REVERSE6) and one other trial evaluated participants with NHYA class II or III (RAFT4). The LVEF inclusion criteria ranged from ≤30% to ≤40% and the minimum QRS duration was ≥120 msec. These results are shown in table 2.
Participant cardiac function and ECG findings for patients with non-LBBB QRS morphology who did or did not receive CRT
Quality assessment of included studies
The quality assessment of included trials is shown in online supplementary appendix 1. All included trials had reliable measures for participant randomisation. Two of the included trials were non-blinded (CARE-HF1, COMPANION2) and for one other trial treating physicians were aware of study group assignments (MADIT-CRT5). An adjudication or end points committee was used to ascertain outcome in four trials (MADIT-CRT5, CARE-HF1, COMPANION2, REVERSE6). Three trials had no significant baseline differences between groups (MADIT-CRT5, COMPANION2, RAFT4).
Risk of adverse outcomes with or without CRT in participants with non-LBBB QRS morphology
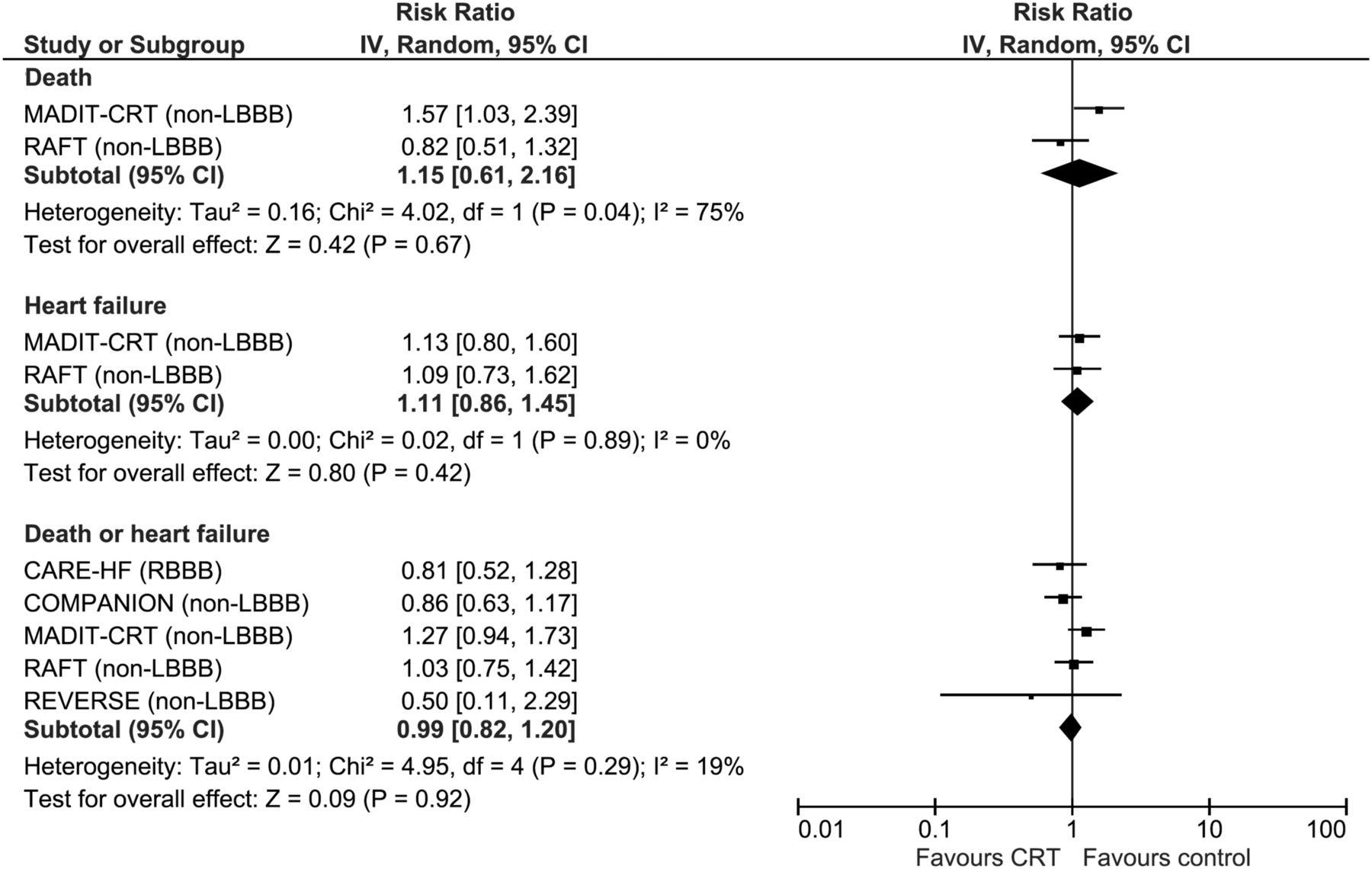
All five trials were included in the evaluation of whether treatment with CRT affects adverse outcomes (death, HF hospitalisation, and the composite of death or HF hospitalisation) in participants with non-LBBB QRS morphology. Outcomes for patients without LBBB in each trial are shown in table 3. Two studies were pooled to evaluate the risk of death, which was not significant (RR 1.15 95% CI 0.61 to 2.16, I2=75%, two trials, 581 participants with non-LBBB) (MADIT-CRT20, RAFT12). For risk of HF among the same two studies there was no evidence of any benefit associated with CRT treatment (RR 1.11 95% CI 0.86 to 1.45, I2=0%, two trials, 581 participants with non-LBBB). Considering death or HF, the pooled result of five studies was not significant (RR 0.99 95% CI 0.82 to 1.20, I2=19%, five trials, 1766 participants with non-LBBB) (CARE-HF18, COMPANION2, MADIT-CRT20, RAFT12, REVERSE14). These results are shown in figure 2.
Treatment group and results for patients with non-LBBB QRS morphology who did or did not receive CRT
{kind=link}
{kind=link}
Risk of adverse outcomes among patients with non-left bundle branch block (non-LBBB) QRS morphology who did or did not receive cardiac resynchronisation therapy (CRT).
Sensitivity analysis excluding trials of participants with RBBB
Sensitivity analysis was performed excluding the CARE-HF1 trial that reported RBBB rather than non-LBBB. After exclusion of this trial, the risk of death or HF was RR 1.03 95% CI 0.83 to 1.27 (four trials).
Meta-regression considering the effect of year of study
We performed two sets of meta-regression analyses: one based on the start year of the trials, and the other based on the mean year across the duration of the trials for the analysis of death or HF (see online supplementary figure S1). The analysis based on the start year and mean year across the duration of the trials yielded similar findings. All relationships from both analyses were not statistically significant.
Discussion
This meta-analysis of landmark CRT trials is the largest to date, including data from five RCTs and 6523 participants. We demonstrate no significant benefit of CRT in patients with non-LBBB QRS morphology, with an overall HR of 0.99 (95% CI 0.82 to 1.20) for the composite of death and HF hospitalisation. Wide QRS with non-LBBB morphology remains an area of uncertainty for CRT, which is included in recent ESC guidelines with a weaker strength of recommendation,8 but is not supported by a dedicated RCT.
To date, there have been no RCTs to address the efficacy of CRT specifically in patients with non-LBBB QRS morphology. Subgroup analysis of all the individual RCTs of CRT has not shown any benefit in reducing death or HF hospitalisation in patients with non-LBBB QRS morphology. Small retrospective analyses that lack a non-CRT control arm have indicated worse outcomes in CRT recipients with non-LBBB compared with LBBB.21–24 However, in the absence of a dedicated RCT of CRT in non-LBBB, the most appropriate method to estimate the benefit of CRT in these patients is to perform meta-analysis of subgroup data from RCTs enrolling LBBB and non-LBBB subjects.
Our data confirm the findings of the previous meta-analysis of Sipahi et al7 who demonstrated a similar lack of benefit of CRT in patients with non-LBBB QRS morphology. In addition to the RCTs analysed in the previous meta-analysis, the current study also includes data from the REVERSE6 trial, adding an additional 610 patients to the meta-analysis (283 patients without LBBB); this makes the current study the largest available meta-analysis of CRT in non-LBBB QRS morphology. Although the original report of REVERSE did not report death/HF outcomes according to QRS morphology, a subsequent retrospective analysis of QRS morphology yielded relevant subgroup data.14 The REVERSE analysis14 was not published at the time of the previous meta-analysis.
Two smaller studies, the Multicentre InSync Randomized Clinical Evaluation (MIRACLE) trial3 ,24 and the Multicentre InSync ICD Randomized Clinical Evaluation (MIRACLE ICD) trial25 did not report death or HF hospitalisation endpoints according to QRS morphology, and so were not included in the present meta-analysis. However, these were the only RCTs to enrol patients with moderate-to-severe symptoms (NYHA class III–IV) and report symptom-driven end points (change in NYHA class or quality of life) according to QRS morphology. This is of particular relevance as the recent NICE technology appraisal recommends CRT in patients with non-LBBB QRS morphology with QRS duration 120–149 msec who have NYHA class IV symptoms.11 While symptomatic improvement was observed in the small cohort of subjects with non-LBBB QRS morphology, in MIRACLE,24 subjective reporting of symptoms is difficult to standardise and reproduce in comparison with objective measures such as death or HF hospitalisation. Furthermore, only 8 out of 78 non-LBBB participants in MIRACLE had NYHA class IV symptoms (the majority being NYHA class III). MIRACLE ICD demonstrated an improvement in NYHA class, quality of life and exercise capacity that was not significantly influenced by QRS morphology, although only a small number of patients with isolated RBBB were enrolled (25 in the CRT arm, 24 in the control arm), of whom only approximately 10% were in NYHA class IV; the authors note that this post hoc analysis was not preplanned and may have been underpowered.25
In addition to the meta-analysis by Sipahi et al,7 a further individual patient meta-analysis of five CRT trials was recently published by Cleland et al.13 Although this study showed no benefit of CRT on all-cause mortality, or the composite of death or HF hospitalisation, in univariate subgroup analyses of subjects with RBBB or NIVCD, when QRS duration was removed from multivariate analysis there was no interaction between QRS morphology and outcomes from CRT.13 Longer QRS duration is an important predictor of CRT response.26 It was observed that patients with NIVCD had shorter QRS duration compared with patients with LBBB and RBBB, which may account for the lack of benefit observed in patients without LBBB after multivariate analysis.
The study by Cleland et al examined a different set of RCTs compared with the present study, including data from the aforementioned MIRACLE and MIRACLE ICD trials, as well as CARE-HF, REVERSE and RAFT which were included in the current study. However, this analysis did not include data from COMPANION and MADIT-CRT, both large trials enrolling 1520 and 1820 patients, respectively, which were included in our data set. As such, the total sample size of our analysis is approximately double that of the analysis by Cleland et al (6523 vs 3872 patients), and the corresponding total number of patients with non-LBBB morphology is significantly greater in our study (1766 vs 813 patients).
Since the publication of the meta-analyses by Sipahi et al7 and Cleland et al,13 new data from the RAFT12 and MADIT-CRT15 trials have emerged. In RAFT, there was a benefit in patients without LBBB with NYHA class II–III symptoms after 2 years when QRS duration was ≥160 msec (HR for death or HF hospitalisation 0.53, 95% CI 0.29 to 0.96), but a trend towards possible harm in patients with QRS <160 msec (HR 1.38, 95% CI 0.89 to 2.14).12 However, the largest single study of the effects of CRT in non-LBBB QRS morphology comes from a subgroup analysis of MADIT-CRT, which enrolled 536 non-LBBB participants with NYHA class I–II symptoms and demonstrated no significant reduction in the primary end point of death or HF hospitalisation in these patients.20 The recently published 7-year follow-up data from MADIT-CRT confirmed no clinical benefit of CRT in patients without LBBB for several end points, and non-LBBB was independently associated with an increase in mortality (HR 1.57, 95% CI 1.03 to 2.39) following adjustment for baseline covariates including QRS duration.15
Differences in cardiac physiology between LBBB and non-LBBB QRS morphology likely underpin the lack of benefit of CRT observed in the latter group. In LBBB RV contraction occurs first, and LV contraction is dyssynchronous due to initial contraction of the septum against the non-activated LV free wall. The main aim of CRT is to ameliorate this mechanical dyssynchrony. Several studies have investigated ventricular electrical activation patterns in patients with wide QRS.27–31 Initial work indicated that LV activation delay may be similar between HF patients with RBBB and LBBB30 however this study only included six patients with RBBB. More recently it has been shown that there is significant heterogeneity in LV activation time (LVAT) among patients with HF with RBBB, with over 50% of RBBB subjects having LVAT ≤100 msec, similar to patients with HF with narrow QRS,27 in whom CRT has been shown to be of no benefit (or possibly harmful) in the large Echocardiography Guided Cardiac Resynchronisation Therapy (EchoCRT) RCT;32 in contrast patients with LBBB had significantly longer LVAT, despite similar QRS duration to patients with RBBB. Importantly, a small number of patients with RBBB had prolonged LVAT, similar to that seen in patients with LBBB.27 These findings may provide a potential explanation for the apparent heterogeneity of CRT response observed in patients without LBBB in the RAFT analysis.12 Work published very recently has also demonstrated significantly shorter LVAT and greater heterogeneity in LV activation pattern in patients with NIVCD compared with LBBB.28 The same study has suggested that ventricular electrical uncoupling (the difference between LV and RV activation times) may be a more powerful predictor of CRT response than QRS duration or the presence of LBBB.28 Furthermore, it has also been shown that there may be significant heterogeneity in ventricular activation patterns even within cohorts of patients with LBBB.29 ,31
These electrocardiographic activation mapping studies serve to illustrate the highly complex relationship between QRS morphology and QRS duration. Furthermore, other important clinical variables such as gender may influence this relationship, with women deriving greater prognostic benefit from CRT than men in MADIT-CRT; notably in this trial a greater proportion of women had LBBB compared with men (87% and 65%, respectively).33 More recently, women have been shown to derive potential benefit from CRT at narrower QRS durations than men.34 Although a previous meta-analysis showed that QRS duration ≤150 msec was not associated with improvements in clinical outcome following CRT,26 recent work, including the individual patient meta-analysis by Cleland et al,13 suggests that there is a continuous relationship between QRS duration and magnitude of CRT response, particularly in patients with LBBB.12 ,34 Furthermore, the Cleland meta-analysis suggested possible mortality benefit with QRS ≥126 msec, with robust evidence for benefit with QRS ≥140 msec.13 Accordingly, the authors’ data provides support to the current NICE and ESC recommendations for CRT in patients with LBBB with QRS ≥120 msec, despite the findings of the previous meta-analysis,26 as the cut-off of QRS ≥150 msec represents an arbitrary figure used to dichotomise RCTs for subgroup analysis.
In contrast, we do not feel that differences in bundle branch block morphology can be considered as arbitrary cut-offs to be used in the same way that the QRS duration ≥150 msec value has been used, as the electrocardiographic activation mapping studies support the hypothesis that LBBB, RBBB and NIVCD represent different pathophysiological entities and thus different substrates for CRT therapy. Thus, in contrast to QRS duration, there is not likely to be a continuous relationship between QRS morphologies and CRT response. Accordingly, the data from our meta-analysis does not support the use of CRT in patients with non-LBBB QRS morphology, regardless of QRS duration.
Strengths and limitations
The major strength of this meta-analysis is the large number of patients included in the analysis, making it the largest analysis to date of CRT in non-LBBB QRS morphology. The main limitation is the use of subgroup data for the meta-analysis, rather than individual patient data, and therefore our data has limited utility in assessing the interaction of QRS morphology with other important clinical variables, for example, QRS duration. In the absence of a dedicated non-LBBB RCT, an individual patient-level analysis of CRT efficacy according to QRS duration in these subjects is mandated. It is also noteworthy that there is a significant time span (13 years) across the enrolment period of the included trials, and as such the possibility of heterogeneity due to advances in other HF therapies cannot be excluded through meta-regression without access to individual patient-level data. Furthermore, our analysis only included mortality and HF hospitalisation as end points, and not symptom-driven end points such as quality of life or change in NYHA class; as such we cannot exclude a symptomatic benefit of CRT in patients without LBBB, although data on these outcomes in patients without LBBB is even more limited.
Conclusion
This meta-analysis shows no reduction in death or HF hospitalisation from CRT in patients with non-LBBB QRS morphology. Wide QRS with non-LBBB morphology remains an area of uncertainty for implanting a CRT device, included in recent ESC guidelines with a weaker strength of the recommendation, but not supported by a dedicated trial. A dedicated RCT of CRT in patients with non-LBBB QRS morphology is needed to establish the efficacy of CRT in this subset of patients with HF.
Key messages
What is already known on this subject?
Cardiac resynchronisation therapy (CRT) is recommended for patients with severe LV systolic dysfunction and QRS duration ≥120 msec.
Previous analyses have suggested a lack of benefit in patients with non-left bundle branch block (LBBB) QRS morphology.
What might this study add?
This is the largest CRT meta-analysis to date.
CRT is not associated with a reduction in death or heart failure hospitalisation in patients with non-LBBB QRS morphology.
How might this impact on clinical practice?
Clinicians need to reconsider the risk versus benefit of CRT in patients with non-LBBB QRS morphology as recommended in contemporary CRT guidelines.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
- Data supplement 2 - Online figure
Footnotes
Correction notice The CRT outcomes for the RBBB subgroup in the CARE-HF and MIRACLE trials had been erroneous in the original published version of the manuscript; these data have now been amended with the correct figures. Importantly, after these errors have been addressed, the principal findings of the analysis are unchanged, in that CRT is not associated with reduction in mortality or heart failure hospitalisation in patients with non-LBBB QRS morphology.
Contributors CC and CSK drafted the manuscript. MAK and FZA performed data extraction. CSK performed the literature search and meta-analysis. MAM and CSK checked the results of the data extraction. MAM, DKS, AP and AZ critically reviewed the manuscript.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.