Article Text

Abstract
Objective We aimed to investigate whether preoperative serum neutrophil gelatinase-associated lipocalin (sNGALpre-op) predicted postoperative acute kidney injury (AKI) during hospitalisation and 1-year cardiovascular and all-cause mortality following adult cardiac surgery.
Methods This study was a post hoc analysis of the Effect of Remote Ischemic Preconditioning on Clinical Outcomes in Patient Undergoing Coronary Artery Bypass Graft Surgery trial involving adult patients undergoing coronary artery bypass graft. Postoperative AKI within 72 hours was defined using the International Kidney Disease: Improving Global Outcomes classification.
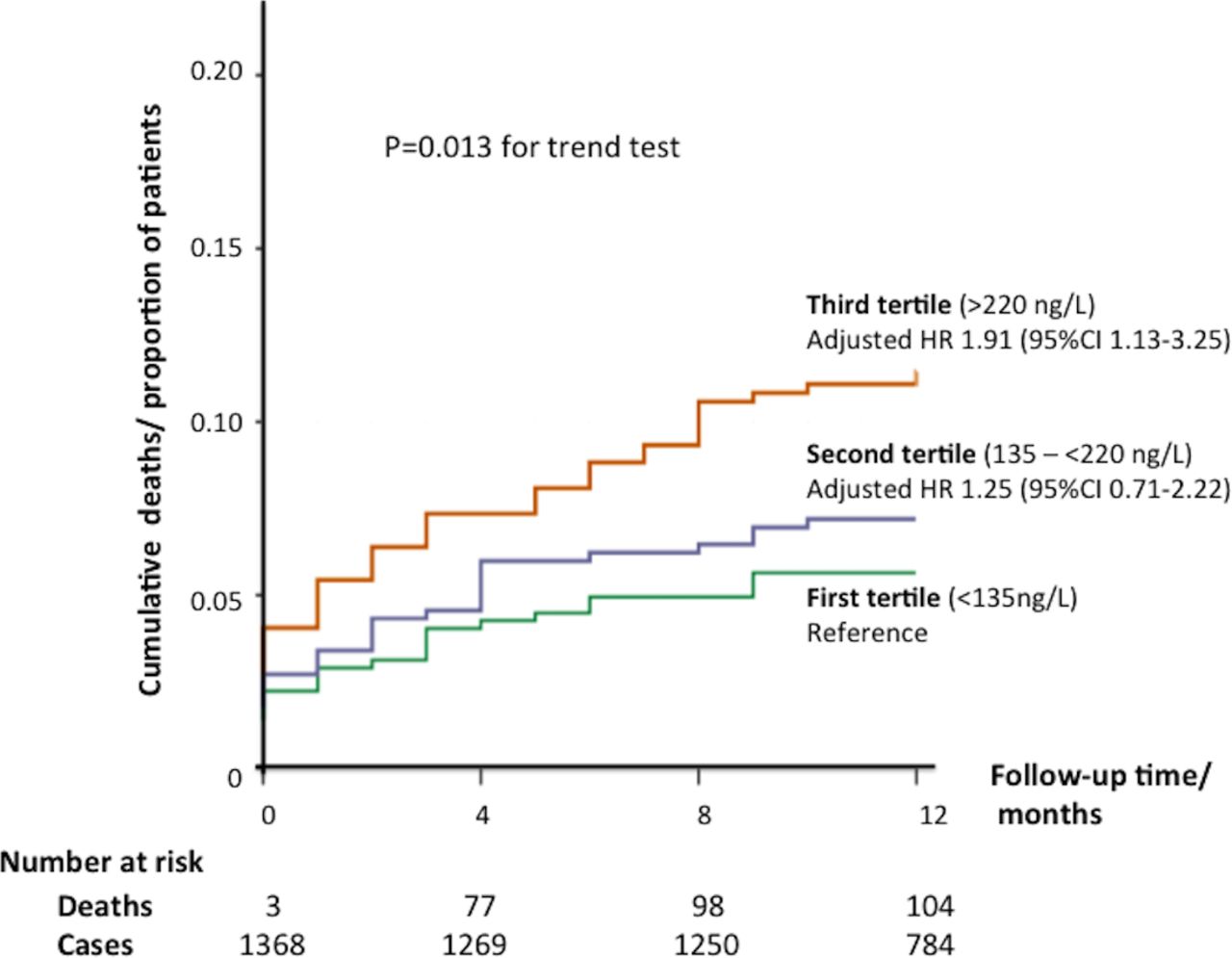
Results 1371 out of 1612 patients had data on sNGALpre-op. The overall 1-year cardiovascular and all-cause mortality was 5.2% (71/1371) and 7.7% (105/1371), respectively. There was an observed increase in the incidence of AKI from the first to the third tertile of sNGALpre-op (30.5%, 41.5% and 45.9%, respectively, p<0.001). There was also an increase in both cardiovascular and all-cause mortality from the first to the third tertile of sNGALpre-op, linear trend test with adjusted p=0.018 and p=0.013, respectively. The adjusted HRs for those in the second and third tertiles of sNGALpre-op compared with the first tertile were 1.60 (95% CI 0.78 to 3.25) and 2.22 (95% CI 1.13 to 4.35) for cardiovascular mortality, and 1.25 (95% CI 0.71 to 2.22) and 1.91 (95% CI 1.13 to 3.25) for all-cause mortality at 1 year.
Conclusion In a cohort of high-risk adult patients undergoing cardiac surgery, there was an increase in postoperative AKI and 1-year mortality from the first to the third tertile of preoperative serum NGAL. Those in the last tertile (>220 ng/L) had an estimated twofold increase risk of cardiovascular and all-cause mortality at 1 year.
Clinical trial registration NCT101247545; Post-results.
- coronary artery disease
- coronary artery disease surgery
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 4.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/4.0/
Statistics from Altmetric.com
Introduction
Acute kidney injury (AKI) occurs in up to 30%1 2 of adult patients undergoing cardiac surgery, and its presence is associated with worse short-term and long-term morbidity and mortality.3–5 Even mild to moderate increases in serum creatinine following cardiac surgery are associated with higher 30-day mortality.6 7 Around a fifth of patients with AKI will go on to require renal replacement therapy,8 and this subgroup has the worst prognosis with in-hospital mortality rates up to 60%.9 The development of AKI is multifactorial, and the underlying mechanisms remain unclear, although acute tubular necrosis is assumed to be the predominant pathology.10 Although several tools have been developed to predict the development of AKI prior to cardiac surgery, they have been predominantly designed to predict severe AKI requiring dialysis.2 More work remains to be done to improve the identification of those at risk of even milder grades of AKI prior to cardiac surgery.2
Neutrophil gelatinase-associated lipocalin (NGAL) belongs to the lipocalin family and is produced predominantly by the liver and white blood cells.11 It is released excessively in the blood pool and in the urine after injury to the kidney tubules.12 NGAL has previously been termed the ‘troponin-like’ biomarker to detect AKI,13 but after promising results in children undergoing cardiac surgery,14 it has not performed as well for the early detection of AKI in adults.15 This can be partly explained by the fact that NGAL is not specific for the kidney injury, as it can also be released during sepsis, inflammation and acute exacerbations of chronic illnesses, and therefore it remains a research tool.14 Most recently, preoperative plasma NGAL has been shown to be independently associated with 3-year mortality following adult cardiac surgery.16 There are some conflicting reports on whether preoperative plasma NGAL can predict postoperative AKI,17 18 but those studies were underpowered. Therefore, we aimed to investigate whether preoperative serum NGAL (sNGALpre-op) predicted both postoperative AKI during hospitalisation and 1-year cardiovascular and all-cause mortality in adults undergoing cardiac surgery.
Methods
The current study was a post hoc analysis of the Effect of Remote Ischemic Preconditioning on Clinical Outcomes in Patient Undergoing Coronary Artery Bypass Graft Surgery (ERICCA) (NCT01247545), the trial design and results of which have been previously published.19 20 In brief, 1612 patients were prospectively recruited in this multicentre, randomised controlled trial between April 2011 and March 2014 but only those with data on sNGALpre-op were included in this analysis (n=1371). The inclusion criteria were adults aged >18 years of age and with an additive European System for Cardiac Operative Risk Evaluation (EuroSCORE) ≥5 (high risk), undergoing on-pump coronary artery bypass grafting (CABG) with or without valve surgery, with blood cardioplegia. Those with an estimated glomerular filtration rate (eGFR) <30 mL/min/1.73 m2 were excluded. They were randomised to remote ischaemic conditioning (RIC) or sham preconditioning. The clinical endpoints collected were cardiovascular death and all-cause mortality at 1 year, non-fatal myocardial infarction, coronary revascularisation or stroke at 1 year and AKI within 72 hours followingsurgery as defined by the International Kidney Disease: Improving Global Outcomes classification (KDIGO).21 There was no difference in the incidence of AKI between those who were randomised to RIC or sham. Serum NGAL was measured from blood collected in serum-separating tubes preoperatively using CircuLex NGAL/Lipocalin 2 ELISA. The study was approved by the National Health Service Research Ethics Committee, and all patients provided informed written consent.
AKI within 72 hours was graded as none, 1, 2, 3 as per the KDIGO criteria as follows: grade 1: serum creatinine 1.5–1.9 times baseline or an increase in serum creatinine ≥26.5 μmol/L; grade 2: serum creatinine 2.0–2.9 times baseline; and grade 3: serum creatinine 3.0 times baseline or increase in serum creatinine to ≥353.6 μmol/L or initiation of renal replacement therapy. The primary outcomes of interest were any AKI grade during hospitalisation and cardiovascular and all-cause mortality at 1 year.
Statistical analysis
Statistical analysis was performed using SPSS V.23. sNGALpre-op was analysed as tertiles. Continuous data were expressed as means and SD or medians and (first quartile–third quartile), and categorical data were reported as frequencies and percentages. Unadjusted associations of the tertiles of sNGALpre-op with other baseline and procedure variables were performed using one-way analysis of variance or Kruskal-Wallis test where appropriate. Logistic regression analysis was performed to assess whether sNGALpre-op was an independent predictor any grade of AKI (as a binary outcome), after adjusting for known preoperative predictors of AKI (age, gender, diabetes mellitus, hypertension, peripheral vascular disease (PVD), previous CABG, type of surgery planned, use of intra-aortic balloon pump, baseline eGFR, baseline left ventricular ejection fraction (LVEF) category and preoperative high sensitivity troponin T).2 22 This analysis was performed using tertiles of sNGALpre-op, as previously done,16 to allow findings to be more easily translated to the clinical setting. Kaplan-Meier curves were used to assess survival at 1 year per tertile. The primary analysis for the cumulative incidence of cardiovascular and all-cause mortality at 1 year was performed using Cox proportional hazard (with censoring of data to the date of occurrence of the primary endpoint, lost to follow-up, withdrawal from the study or at 1 year), and the HRs were computed with 95% CI after adjusting for the factors that were present in both EuroSCORE II23 and the Society of Thoracic Surgeon (STS) score24 that were available from our cohort (namely age, gender, eGFR, PVD, previous stroke, previous CABG, baseline LVEF category, diabetes mellitus, use of intra-aortic balloon pump, type of surgery planned and preoperative high sensitivity troponin T).
Results
Out of 1612 patients recruited in the ERICCA trial, 1371 patients had sNGALpre-op measured. These patients had a mean age of 76.0±6.6 years and 27.5% were female. As expected, they were in the high-risk category for cardiac surgery with a median additive EuroSCORE of 6 (5–7). Further details of the baseline characteristics of these 1371 patients per tertile are provided in table 1. The overall all-cause mortality and cardiovascular mortality was 7.7% (105/1371) and 5.2% (71/1371), respectively. AKI data were available in 97% (1330/1371) of patients. AKI during the initial hospitalisation occurred in 39.6% of patients (31.2% AKI grade 1). The median sNGALpre-op was 175 (117–257) ng/L and range of 27–3171 ng/L. sNGALpre-op was divided into three groups according to tertiles <135 ng/L, 135–<220 ng/L and ≥220 ng/L. There was no difference in the prevalence of diabetes mellitus, hypertension, dyslipidaemia and vascular disease among the three tertiles as shown in table 1. Furthermore, there was no difference in the type of surgery or duration of the cardiopulmonary bypass and cross-clamp times. However, patients in the higher tertiles were more likely to be older, of the male gender, have higher baseline creatinine and eGFR and spend longer time on intensive care unit and in hospital. The cardiovascular and all-cause mortality at 1 year per tertile and per the presence or absence of AKI are summarised in table 2.
Characteristics of patients according to tertiles of sNGALpre-op
One-year cardiovascular and all-cause mortality rates per tertiles of sNGALpre-op and per presence or absence of AKI
sNGALpre-op and AKI
On a per-tertile basis, there was an increase in the incidence of AKI with increasing tertile of sNGALpre-op from 30.5% in the first tertile, 41.5% in the second tertile and 45.9% in the third tertile. Using the first tertile of sNGALpre-op as reference, multivariable analysis shown that the second tertile of sNGALpre-op had an OR of 1.69 (95% CI 1.23 to 2.30), and the third tertile of sNGALpre-op had an OR of 1.53 (95% CI 1.12 to 2.10), p=0.009 for linear trend test, to predict AKI, after adjusting for known preoperative predictors of AKI.
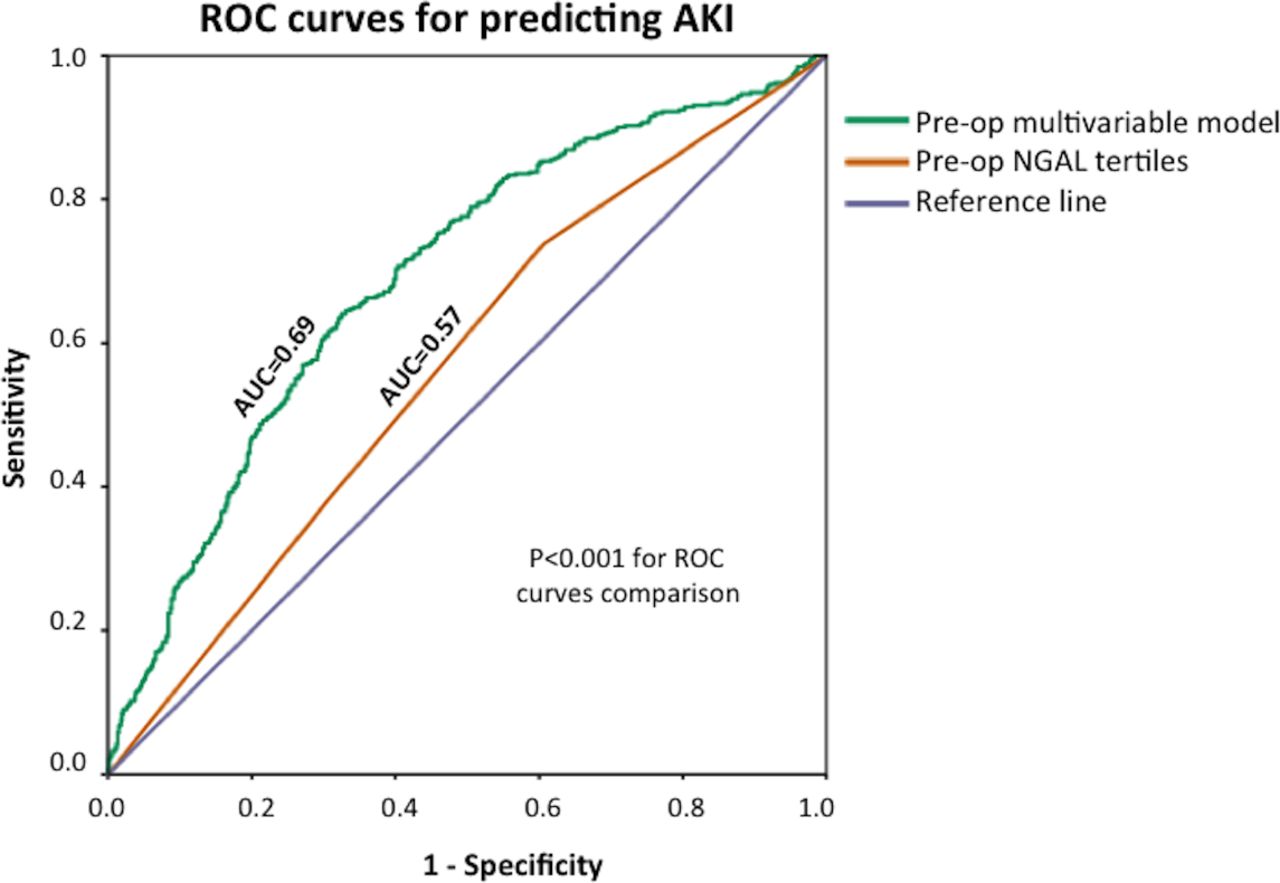
Receiver operating characteristic (ROC) curve analysis showed that sNGALpre-op was a predictor of AKI, but the c-statistic was only 0.57 (95% CI 0.54 to 0.61). The c-statistic improved to 0.69 (95% CI 0.66 to 0.73) (p<0.001 for ROC curves comparison) when age, gender, diabetes mellitus, hypertension, PVD, previous CABG, type of surgery planned, use of intra-aortic balloon pump, baseline eGFR, baseline ejection fraction and baseline high sensitivity troponin T were included in the model together with tertiles of sNGALpre-op as shown in figure 1.

ROC curves of sNGALpre-op in tertiles and the preoperative multivariable model to predict AKI. AKI, acute kidney injury; AUC, area under the curve; ROC, receiver operating characteristic; sNGALpre-op, preoperative serum neutrophil gelatinase-associated lipocalin.
AKI and mortality
Patients with AKI had a higher mortality at 1 year with an all-cause mortality rate of 12.1% versus 4.1% (table 2), when compared with those without AKI with an adjusted HR (adjusted for the above EuroSCORE II and STS-derived preoperative predictors of mortality) of 2.67 (95% CI 1.72 to 4.13), adjusted p<0.001 from the Cox regression analysis. Those with AKI also had worse cardiovascular mortality at 1 year with a mortality rate of 7.8% versus 2.7%, when compared with those without AKI, with an adjusted HR of 2.88 (95% CI 1.67 to 4.98), adjusted p<0.001 from the Cox regression analysis.
sNGALpre-op and mortality
After a follow-up of 12 months, 5.5% of patients in the first tertile died, compared with 7.0% in the second tertile and 10.5% of the patients in the third tertile as summarised in table 2. There was an increase in both cardiovascular and all-cause mortality from the first to the third tertile of sNGALpre-op, linear trend test with adjusted p=0.018 and p=0.013, respectively. With sNGALpre-op in the first tertile as the reference, the adjusted HR (adjusted for the above EuroSCORE II and STS-derived preoperative predictors of mortality) for those in the second and third tertiles of sNGALpre-op were 1.60 (95% CI 0.78 to 3.25) and 2.22 (95% CI 1.13 to 4.35) for cardiovascular mortality, and 1.25 (95% CI 0.71 to 2.22) and 1.91 (95% CI 1.13 to 3.25) for all-cause mortality at 1 year. Figure 2 shows the Kaplan-Meier curves for 1-year all-cause mortality according to tertiles of sNGALpre-op.
{kind=link}
{kind=link}
Kaplan-Meier curves for 1-year all-cause mortality according to tertiles of sNGALpre-op. sNGALpre-op, preoperative serum neutrophil gelatinase-associated lipocalin.
Discussion
The major findings of this study of high-risk patients undergoing cardiac surgery were as follows: (1) preoperative serum levels of NGAL predicted postoperative AKI, after accounting for preoperative clinical parameters (age, gender, diabetes mellitus, hypertension, PVD, previous CABG, type of surgery planned, use of intra-aortic balloon pump, baseline eGFR, baseline ejection fraction and baseline high sensitivity troponin T), with the performance of sNGALpre-op to predict AKI improving when these clinical parameters were included in the model; (2) tertiles of sNGALpre-op were associated with mortality after adjusting for confounders, with those in the third tertile having a twofold increase in the hazard for cardiovascular and all-cause mortality; (3) the overall incidence of postoperative AKI in this cohort was 39.6% and was as high as 45.9% for those in the third tertile of sNGALpre-op; (4) the presence of AKI was associated with mortality, and in our cohort, there was more than twofold increase in both cardiovascular and all-cause mortality at 1 year.
The performance of the model to predict AKI was improved when clinical parameters were included in addition to sNGALpre-op, but the c-statistic was only increased to 0.69. Other risk scores to predict AKI have had c-statistics ranging between 0.72 and 0.84, but most of them were designed to predict worse grades of AKI.2 Therefore, Huen et al 2 recently concluded that more studies are required to develop risk models to predict milder forms of AKI after cardiac surgery in a systematic review of existing risk scores. However, our study included high-risk patients with EuroSCORE ≥5 only and whether by applying the same approach of using sNGALpre-op with clinical parameters to predict any grades of AKI would yield a higher diagnostic performance warrants further investigation.
Postoperative urinary NGAL25 in contrast to postoperative plasma NGAL16 has been shown to be associated with all-cause 3-year mortality. Whether pNGALpre-op could predict AKI and mortality has also been investigated. Haase-Fielitz et al 17 found no difference in preoperative serum NGAL between those who developed AKI when compared with those who did not. However, this study only included 100 patients and did not have mortality data. However, Doi et al 18 showed that preoperative plasma NGAL was an independent risk factor for postoperative AKI in 146 patients. A larger study of 1191 patients showed that preoperative plasma NGAL was a predictor of 3-year mortality, but the relationship between NGAL and AKI was not assessed.16 In the general population, baseline plasma NGAL has also been shown to be associated with 10-year cardiovascular mortality.26 In a cohort of community-dwellers with a mean age of 70 years, plasma NGAL was a significant predictor of mortality, independent of traditional risk factors and renal function.27 We have shown in a larger cohort of high-risk patients that sNGALpre-op was a predictor of both AKI following cardiac surgery, as well as a predictor of 1-year cardiovascular and all-cause mortality, after adjusting for known preoperative predictors of AKI. Therefore, sNGALpre-op could complement existing tools to risk-stratify patients prior to cardiac surgery.
AKI has typically been reported to occur in up to 30%1 2 of patients undergoing adult cardiac surgery, but the incidence of AKI in our cohort was higher at 39.6%. This may be explained by the inclusion of patients with an additive EuroSCORE of ≥5 and therefore representative of the incidence of AKI in a high-risk cohort.
Limitations
Our cohort may not be representative of the wider population of patients undergoing CABG surgery as these patients were included in a randomised controlled trial. There are currently no established cut-off values as shown by the study by Moledina et al,16 which used cut-off values of 155 ng/L and 251 ng/L for the tertiles and we used 130 ng/L and 220 ng/L. Although intraoperative factors play a role in the development of postoperative AKI, we only looked at preoperative factors as the aim of this study was to assess the ability of sNGALpre-op to identify those at higher risk of AKI and mortality prior to surgery. Ten per cent of the cases had missing data when it came to performing the analysis for the adjusted models. We did not specifically collect data on sepsis or exacerbation of chronic illness prior to surgery, which are known confounders for elevated NGAL levels. However, these patients were considered fit enough for major heart surgery, and therefore it is unlikely these confounders were present at the time.
Conclusions
In a cohort of high-risk adult patients undergoing cardiac surgery, preoperative serum NGAL was an independent predictor of postoperative AKI and 1-year cardiovascular and all-cause mortality. Those in the third tertile of preoperative serum NGALpre-op (>220 ng/L) had a twofold increase risk of postoperative AKI and mortality at 1 year. The risk stratification of patients prior to cardiac surgery may be improved by adding preoperative serum NGAL to existing risk scores for AKI and mortality and warrants further investigations.
Key messages
What is already known about this subject?
The development of acute kidney injury following adult cardiac surgery is associated with short-term and long-term morbidity and mortality.
What are the new findings?
Preoperative serum neutrophil gelatinase-associated lipocalin was an independent predictor of postoperative acute kidney injury and 1-year mortality.
How might these results change the focus of research or clinical practice?
Preoperative serum neutrophil gelatinase-associated lipocalin could be used on top of existing risk scores to further risk-stratify those at higher risk of postoperative acute kidney injury and 1-year mortality.
References
Footnotes
Contributors Conception this work: HB, LC, DMY and DJH. Acquisition of the data: LC, RE, DJ, SKM, GK, CL, JPM and DMY. Analysis and interpretation of the data: HB, RM, BC, JN, TC and DJH. Drafting of the manuscript: HB, RM, BC, LC and DJH. Critical review of the manuscript: CL, DMY, DJH, TC, LC, GK, DJ, JN, JPM, SKM and CL. Final approval of the version to be published: all authors. Guarantor of this work: DJH.
Funding The ERICCA study was supported by grants from the Efficacy and Mechanism Evaluation Program (a Medical Research Council and National Institute of Health Research partnership) (09/100/05) and the British Heart Foundation. Part of this work was supported by the National Institute for Health Research, University College London Hospitals, Biomedical Research Centre, the British Heart Foundation(FS/10/039/28270), Duke-National University Singapore Medical School, the Singapore Ministry of Health’s National Medical Research Council under its Clinician Scientist-Senior Investigator scheme (NMRC/CSA7SI/0011/2017) and Collaborative Centre Grant scheme (NMRC/CGAug16C006) and the Singapore Ministry of Education Academic Research Fund Tier 2 (MOE20167T2727021).
Competing interests None declared.
Patient consent Obtained.
Ethics approval This study was approved by the National Health Service Research Ethics Committee, and all patients provided informed written consent.
Provenance and peer review Not commissioned; externally peer reviewed.