Article Text

Abstract
Objective Data on the contribution of ambulatory blood pressure (ABP) components to the risk of developing atrial fibrillation (AF) are limited. We prospectively tested the hypothesis that ABP may represent a potentially modifiable risk factor for the development of AF in a European population study.
Methods We recorded daytime blood pressure (BP) in 3956 subjects randomly recruited from the general population in five European countries. Of these participants, 2776 (70.2%) underwent complete 24-hour ABP monitoring. Median follow-up was 14 years. We defined daytime systolic BP load as the percentage BP readings above 135 mm Hg. The incidence of AF was assessed from ECGs obtained at baseline and follow-up and from records held by general practitioners and/or hospitals.
Results Overall, during 58 810 person-years of follow-up, 143 participants experienced new-onset AF. In adjusted Cox models, each SD increase in baseline 24 hours, daytime and night-time systolic BP was associated with a 27% (P=0.0056), 22% (P=0.023) and 20% (P=0.029) increase in the risk for incident AF, respectively. Conventional systolic BP was borderline associated with the risk of AF (18%; P=0.06). As compared with the average population risk, participants in the lower quartile of daytime systolic BP load (<3%) had a 51% (P=0.0038) lower hazard for incident AF, whereas in the upper quartile (>38%), the risk was 46% higher (P=0.0094).
Conclusions Systolic ABP is a significant predictor of incident AF in a population-based cohort. We also observed that participants with a daytime systolic BP load >38% had significantly increased risk of incident AF.
- ambulatory blood pressure
- atrial fibrillation
- incidence
- daytime systolic pressure load
- longitudinal studies
- population
Statistics from Altmetric.com
- ambulatory blood pressure
- atrial fibrillation
- incidence
- daytime systolic pressure load
- longitudinal studies
- population
Introduction
Atrial fibrillation (AF) is the most common cardiac arrhythmia in the general population, and its incidence is substantially increasing with the ageing populations.1 Over 50 years of observation in the Framingham Heart Study, the age-adjusted prevalence of AF increased from 20.4 to 96.2 cases per 1000 person-years in men and from 13.7 to 49.4 cases per 1000 person-years in women.2 Globally, the estimated number of individuals with AF in 2010 was 33.5 million,1 and the prevalence of AF is expected to significantly rise in the coming years.3 4 These data underscore the need for a better understanding of the complexity of AF determinants and for improvement of AF prevention strategies related to the specific modifiable risk factors.
It is well established that hypertension is one of the most important contributors to the burden of AF and can potentially explain more than one-fifth of all AF cases, and nearly one quarter, if a borderline high blood pressure (BP) was also included.5 The importance of individual BP components on conventional BP in the development of AF has also been investigated.6–9 In the Framingham Heart Study,10 participants belonging to the trajectory groups with persistently elevated systolic BP and longer antihypertensive treatment had an increased 15-year risk of incident AF as compared with participants who remained normotensive throughout the longitudinal data collection. The researchers suggested that each trajectory group of systolic and diastolic BP may have unique properties that require further investigation.10
Our previous study based on a large population database from four countries has shown that daytime ambulatory BP (ABP) was superior to conventional BP in the predicting of cardiovascular events and risk stratification.11 However, to our knowledge, only two small studies in patients with hypertension8 and in general population12 have investigated the relative significance of different ABP components in predicting new-onset AF. Accordingly, we prospectively tested the hypothesis that ABP measurement is a potentially modifiable risk factor for incident AF in general population randomly recruited in five European countries.
Methods
Study population
Recruitment for the Flemish Study on Environment, Genes and Health Outcomes (FLEMENGHO) started in 1985.13 A random sample of the households living in a geographically defined area of Northern Belgium was investigated with the goal to recruit an equal number of participants in each of six subgroups by sex and age. The European Project on Genes in Hypertension (EPOGH) investigators applied the same recruitment and examination protocols, questionnaires and follow-up procedures, as used in FLEMENGHO.14
Online supplementary table S1 lists detailed information on participation rate, enrolment and duration of follow-up of the included cohorts. We measured the conventional and ABP at baseline in 4314 participants, including 2904 FLEMENGHO and 1410 EPOGH participants. We excluded individuals if they were younger than 18 years (n=304) or if they had <10 daytime BP readings (n=38). After exclusion of 16 subjects with AF at baseline, the number of subjects totaled 3956. Of these, 2776 (70.2%) participants underwent complete 24-hour ABP monitoring including both daytime and night-time periods.
Supplementary file 1
Conventional and ABP measurement
At the participants’ homes, trained observers measured the conventional BP with a mercury sphygmomanometer, using the appropriate cuff size, with participants in the sitting position. The conventional BP was the average of five consecutive readings. We programmed portable BP monitors to obtain daytime ABP readings at 15 min or, in the FLEMENGHO study, 20 min intervals from 08:00 to 22:00 and at 45 min at night.11 15 The used devices implemented an oscillometric technique (SpaceLabs 90207; Spacelabs, Washington, USA, and The Takeda TM2430; A&D, Tokyo, Japan). Daytime and night-time was defined as the intervals ranging from 10:00 hours to 20:00 hours and from 00:00 hours to 06:00 hours, respectively.16 We weighted the individual means of the ABP by the time interval between successive readings. Recordings with less than 10 daytime and/or five night-time readings were not considered for analysis. For both conventional and ABP measurements, pulse pressure was the difference between the systolic and diastolic BP.
In line with current guidelines for the diagnosis and management of hypertension,17 we defined hypertension as a conventional BP equal to or exceeding 140 mm Hg systolic or 90 mm Hg diastolic or as use of antihypertensive drugs. Corresponding thresholds for daytime ambulatory hypertension were 135 mm Hg systolic and 85 mm Hg diastolic daytime BP. We defined daytime systolic BP load as the percentage BP readings above the cut-off point as defined by the European Society of Hypertension (135 mm Hg). Normotension was a consistently untreated normal BP on both conventional and ambulatory measurements. White-coat hypertension was a raised conventional BP in the presence of a normal daytime BP. Masked hypertension was an elevated ABP with normal conventional BP. Sustained hypertension was a consistently elevated BP on both conventional and ambulatory measurements. Patients on antihypertensive drug treatment were classified as having sustained hypertension.
Other measurements
In all centres, at the enrolment visit and at follow-up, a standardised questionnaire was used to collect detailed information on each subject’s medical history, smoking and drinking habits and intake of medications. Diabetes mellitus was a self-reported diagnosis, or use of antidiabetic agents, or a fasting blood glucose concentration of at least 7.0 mmol/L. In all subjects, standard supine 12-lead resting ECGs were obtained at baseline and at each follow-up visit.
AF ascertainment
We ascertained vital status and the incidence of fatal and non-fatal diseases from the appropriate sources in each country, as described elsewhere.14 We obtained the International Classification of Disease codes for the immediate and underlying cause of death. The diagnosis of sustained or paroxysmal AF was based on the medical records of general practitioners and in the regional hospitals and on ECG obtained at the baseline and follow-up visits. Each ECG was evaluated for the presence of AF by two cardiologists independently. The incidence date of AF was defined as the date of the first ECG showing AF or the date of the first hospital record or standardised questionnaire reporting a confirmed AF diagnosis.
Statistical methods
For database management and statistical analysis, we used SAS software V.9.4. We compared means and proportions by means of a large sample z-test and the χ2 test, respectively.
We first calculated the incidence of AF events according to cross-classification of conventional and daytime BP and quartile of daytime systolic pressure load while standardising for sex and age (age groups: <40 years, 40–60 years and >60 years) by the direct method. We used Cox regression to compute standardised HRs, which express the risk associated with a 1 SD increment in the baseline BP measurements. All Cox regression models included cohort as a random effect. The baseline characteristics considered as covariables in Cox regression were sex, age, body mass index (BMI), smoking, drinking, serum cholesterol, antihypertensive treatment, diabetes mellitus and a history of cardiovascular disease.
In the categorical analyses, we used the Kaplan-Meier survival function estimate and the log-rank test to plot and compare the cumulative incidence of AF across quartiles of conventional systolic BP, daytime systolic BP and daytime systolic BP load. While accounting for important covariables, we also expressed the risk in each systolic pressure or load quartile relative to the overall risk in the whole study population.
Results
Characteristics of participants
The 3956 subjects (mean age 43.1±15.1 years) included 2050 (51.8%) women. Of the participants, 2452 (62.0%) were normotensive, 219 (5.5%) had white-coat hypertension, 364 (9.2%) had masked hypertension, 321 (8.1%) had untreated sustained hypertension and 600 (15.1%) were on antihypertensive drug therapy. Online supplementary table S2 shows the baseline characteristics of these five groups. The whole study population consisted of 2574 Flemish (65.1%), 314 Italians (7.9%), 601 Polish (15.2%), 298 Russians (7.4%) and 174 Czechs (4.4%).
Incidence of AF and its determinants
In the overall study population (n=3956), median follow-up was 14.0 years (5th–95th percentile interval: 5.6–25.2 years). During 58 810 person-years of follow-up, 143 participants experienced AF with a median time-to-event of 12.0 years (2.43 events per 1000 person-years). Of the 2776 subjects who underwent complete 24-hour ABP monitoring including daytime and night-time periods, 111 participants experienced AF with a median time-to-event of 12.1 years (2.76 events per 1000 person-years). Table 1 lists the clinical characteristics of participants with and without incident AF in the whole cohort and in participants with complete 24-hour BP monitoring. Overall, participants with incident AF compared with those without event were older more likely to be male and had a higher prevalence of other cardiovascular risk factors. The conventional and ABP measurements according to AF incidence are shown in table 2.
Clinical baseline characteristics of the study participants with and without incident atrial fibrillation
Conventional and ambulatory blood pressures and heart rate of the study participants with and without incident atrial fibrillation
As expected the risk for AF increased across age groups: four events in participants younger than 40 years (incidence rate: 0.2/1000 person-years; number of subjects=1146), 71 events in the middle-age participants from 40 years to 65 years (3.4/1000 person-years; n=1395) and 36 events in participants older than 65 years (12.6/1000 person-years; n=235).
In addition to age, the incidence of AF increased significantly and independently with BMI (HRs for 5 kg/m2: 1.31; 95% CI 1.10 to 1.58; P=0.0028), history of cardiovascular disease (HRs: 2.54; 95% CI 1.66 to 3.87; P<0.0001) and was higher in men than in women (HRs: 1.73; 95% CI 1.21 to 2.49; P=0.0026). We did not observe any significant association of incident AF with antihypertensive drug treatment (P=0.59).
Risk of AF associated with conventional and ABP
The multivariate-adjusted HR (95% CI) associated with each 1 SD increase in all BP components for incident AF are shown in table 3. We stratified all analyses by cohort and adjusted for sex, age, BMI, total serum cholesterol, history of cardiovascular disease and diabetes, tobacco and alcohol use and antihypertensive drug treatment.
Conventional and 24-hour ambulatory blood pressure in the prediction of atrial fibrillation in 2776 participants with complete 24-hour ambulatory blood pressure monitoring
First, in analyses including 2776 participants with complete 24-hour ABP monitoring, the systolic BPs on 24-hour, daytime and night-time ambulatory measurement were all significant predictors of incident AF (table 3). In these models, each SD increase of systolic 24-hour, daytime and night-time BPs was associated with a 27% (P=0.0056), 22% (P=0.023) and 20% (P=0.029) increase in the risk for developing AF, respectively. Moreover, a higher diastolic BP on 24-hour ambulatory measurement was also associated with a significant increased risk for incident AF (P≤0.024; table 3). In this cohort, systolic BP on conventional measurement was only borderline associated with a 19% increased risk of AF (P=0.060; table 3). Second, in analyses including all 3956 participants with available daytime ABP our results remain similar (online supplementary table S3).
Risk of AF associated with daytime systolic BP load
We further investigated the importance of daytime systolic ABP in predicting incidence of AF by calculating systolic BP load as the percentage BP readings above 135 mm Hg during the day. Of notice, in 766 subjects (19.4%), there were no single systolic BP readings during the day above this limit. Because of its skew distribution (online supplementary figure S1, skewness=1.19) we categorised systolic BP load into quartiles. Table 4 shows the baseline characteristics of the study participants by quartiles of daytime systolic BP load. Participants with high systolic pressure load (>38%) were older, more likely to be male and had a higher prevalence of cardiovascular risk factors, including previous cardiovascular disease, diabetes mellitus, higher BMI and total cholesterol (P<0.05 for all, table 4).
Baseline characteristics of the study participants by quartiles of ambulatory daytime systolic blood pressure load
The risk for AF increased (P=0.0018 for trend) across increasing systolic BP load quartiles: from 10 in the lower quartile (sex-adjusted and age-adjusted incidence rate, 0.91/1000 person-years), to 34 in the medium-low (2.47/1000 person-years) and 42 in the medium-high (2.84/1000 person-years) quartiles, to 57 in the upper quartile (3.50/1000 person-years).
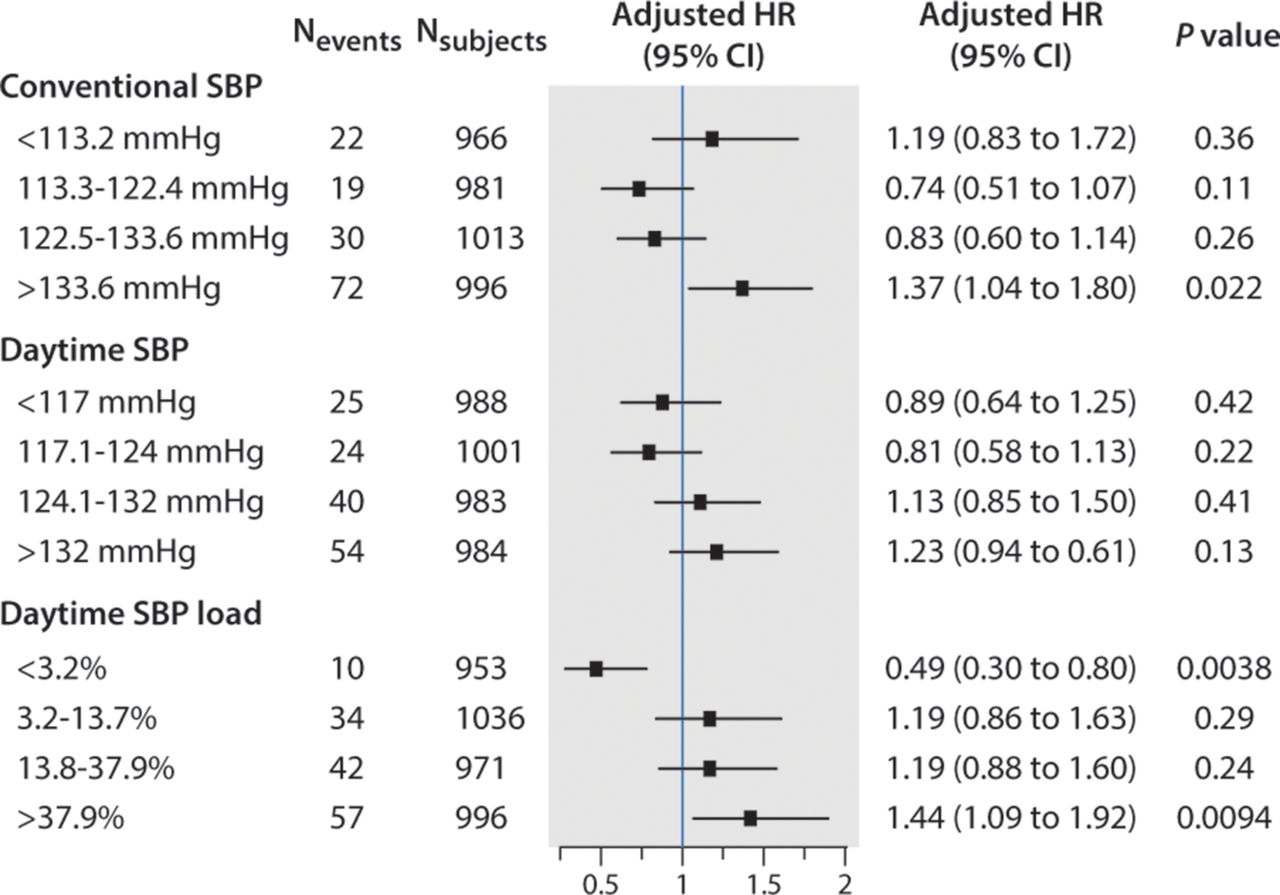
Figure 1 demonstrates the Kaplan-Meier cumulative incidence of AF events in quartiles of conventional and daytime systolic BP and daytime systolic BP load (log-rank test for all P<0.0001). Figure 2 shows the adjusted HR expressing the risk in each quartile compared with the average risk in the whole cohort. For daytime systolic ABP load, in the upper quartile, the risk for incident AF was significantly higher than the average risk (46%, P=0.0094), whereas in the lower quartile, the risk was significantly lower by 51% (P=0.0038). In the upper quartile of conventional systolic BP, the risk was higher than the average risk (37%, P=0.022; figure 2).

Cumulative incidence estimates (1-Kaplan-Meier survival estimates) for atrial fibrillation events by quartiles of conventional systolic blood pressure (SBP) (panel A), daytime systolic blood pressure (panel B) and daytime systolic blood pressure load (panel C). P values are for the differences between groups according to the log-rank test.

{kind=link}
{kind=link}
Multivariable adjusted HRs (95% CI) for atrial fibrillation in quartiles of conventional systolic blood pressure (SBP), daytime systolic blood pressure and daytime systolic blood pressure load in 3956 subjects. The HRs express the risks versus the average risk in the whole cohort (vertical line) and are adjusted for the covariables (centre, sex, age, body mass index, smoking, drinking, serum cholesterol, antihypertensive treatment, diabetes mellitus and a history of cardiovascular disease). P values are for the differences between the risk in quartiles and the population average risk.
Discussion
This study includes a large and comprehensive population-based assessment of both conventional and ABP monitoring on incident AF. Our principal finding is that mean, daytime and night-time systolic ABP were significant predictors of incident AF. Importantly, conventional systolic BP measured by observer at the participants’ homes was only borderline associated with risk of AF events. Moreover, we observed that the risk of new-onset AF was significantly associated with systolic daytime BP load. Indeed, systolic BP load during daytime of more than 38% was associated with a significant increased risk of AF.
On a population basis, hypertension is the most common predisposing factor for incident AF.18 However, one-off conventional BP measurements do not necessarily provide the complete information, in relation to the development of incident AF. In the Framingham study, Rahman et al 10 reported on longitudinal BP patterns, referred to as trajectories. The latter were more closely related to the development of AF than a single office BP measurement, especially when persistently elevated systolic BP is present (HR: 1.95; P=0.03 as compared with normotensive individuals) or antihypertensive treatment is used (HR: 1.97; P<0.0001). In the present study, we showed that ABP monitoring offered significantly incremental predictive value for incident AF, whereas a single conventional BP was only borderline associated with new-onset AF.
To our knowledge, two relatively small studies, one in patients with hypertension and another in a general population cohort, explored new-onset AF in relation to ABP measurements. Ciaroni et al 8 reported that after minimal adjustment for age, sex and BMI, baseline 24-hour systolic BP significantly predicted incident AF (HR: 1.16 per 10 mm Hg increase; 95% CI 1.06 to 2.47; P<0.001) in 597 treated patients with hypertension. In addition to a short follow-up period in this study (18 months) and 28 cases with AF, the authors did not provide information on the office BP measurements and daytime systolic BP. In a general population cohort consisting of 903 subjects, Perkiömäki et al 12 found that the 24-hour systolic BP predicted the occurrence of AF (n=91) over an average of 16.4 years of follow-up (HR: 1.09 per 10 mm Hg increase; P=0.023). The authors emphasised that this association was mainly driven by the association between incident AF and night-time systolic BP. In our study, we observed that the systolic BPs during the entire 24-hour period, daytime and night-time were all similarly associated with the incidence of AF.
Additionally, we found that systolic BP load during the day significantly predicted the new-onset AF. Systolic BP load could be easily calculated as the percentage daytime BP readings above 135 mm Hg. If this percentage exceeds ~38% of overall BP daytime readings, which is corresponded to the upper quartile of daytime systolic BP load in our population, it might be considered as a high BP load. For example, if a patient has overall 20 BP measurements during the day of which 10 recordings exceeding 135 mm Hg, the patient’s systolic BP load is as high as 50%.
Overall, AF might be considered as one of the manifestations of hypertensive target organ damage. Indeed, the presence of uncontrolled hypertension as identified by ABP monitoring leads to more damage in the heart, such as left ventricular hypertrophy, diastolic dysfunction and atrial dilatation. Indeed, a recent meta-analysis of 14 studies in 2485 subjects showed better correlation of echocardiographically measured left ventricular mass with systolic ABP as compared with its correlation with office systolic BP (0.37 vs 0.23).19 Along these lines, a high prevalence of left ventricular hypertrophy (52%) was observed in 1184 patients with non-valvular AF (mean age 72±11 years; 56% men).20 Doménech et al 21 reported the significant association between night-time BP and left atrial size in 48 patients with idiopathic AF. Given that ABP monitoring is associated with target organ damage in hypertension19 and with complications related to hypertension,11 our study emphasises yet again the importance of quantification of the BP ‘load’ with repeated BP measures.
Our study findings might have important clinical implications in the management of AF, including the prevention of AF. Better stratification of subjects at risk for new-onset AF is a way of objectively informing treatment decisions and discreetly distributing medical care. Our observations suggest that ABP monitoring should become routine in the AF risk stratification of patients with hypertension. We also reported, for the first time, that daytime systolic BP load might provide clinically relevant prognostic information on incident AF. This finding should be confirmed in future studies addressing incident AF. Another question is whether inclusion of systolic BP load might improve AF risk stratification in patients with hypertension.
Our study must be interpreted within the context of its potential limitations. First, our present analysis was based only on European population-based cohorts and might not be representative for non-European populations. Second, due to low statistical power, we did not perform sensitivity analysis stratified by age groups particularly in the participants above 65 years in whom AF screening is recommended. Third, in our study, conventional BP was measured at the participants’ homes by trained observers. These BP readings might not be the same conventional BP measurements if they were recorded in the clinic. However, our current data on incident AF in masked hypertension supported our main results on continuous ABP measurements. Fourth, we did not exclude the effect of different types of various antihypertensive drugs over time, which may modulate AF development. Of notice, the proportion of our participants on antihypertensive treatment at baseline was only 15.2%. Finally, the diagnosis of AF was based mainly on medical records and in part on ECG recordings during the regular follow-up visits. However, systematic ECG monitoring over time was not performed.
Conclusions
Systolic ABP is a significant predictor of incident AF in a population-based cohort. We also observed that participants with a daytime systolic BP load >38% had significantly increased risk of incident AF. Thus, effective management of BP load might be important to prevent incident AF.
Key messages
What is already known on this subject?
Previous studies have shown that ambulatory blood pressure (ABP) was superior to conventional blood pressure (BP) in the prediction of cardiovascular events and risk stratification. However, data on the contribution of ABP components to the risk of developing atrial fibrillation (AF) are scarce.
What might this study add?
Our study includes a large and comprehensive population-based assessment of both conventional and ABP monitoring on incident AF. Systolic ABP is a better predictor of incident AF as compared with conventional BP in a population-based cohort. We also observed that the risk of new-onset AF was significantly associated with systolic BP load. Indeed, systolic BP load during daytime of more than 38% was associated with a significant increased risk of AF.
How might this impact on clinical practice?
Better stratification of subjects at risk for new-onset AF is a way of objectively informing treatment decisions and discreetly distributing medical care. Our present findings suggest that ABP monitoring should become routine in the AF risk stratification of patients with hypertension. Our study emphasises the importance of quantification of the BP ‘load’ with repeated BP measures.
Acknowledgments
The list of investigators participated in the FLEMENGHO and EPOGH Study is provided in supplementary material.
References
Footnotes
VT and TK contributed equally.
Contributors KK-J, EC and JAS planned and coordinated the EPOGH and FLEMENGHO projects. VT, TK and LT constructed the database and did the statistical analyses. Responsibility for the integrity of the local datasets rests with: VT and EC (Mirano, Italy); TK, LT, NC and JAS (Noorderkempen, Belgium); KS-S and KK-J (Niepolomice, Poland); JS and JF (Pilsen, Czech Republic); TK and SM (Novosibirsk, Russia); and NG-M, ES and KN (Gdansk, Poland). VT, TK, LT GYHL and JAS wrote the first draft of the paper. All authors interpreted the results and approved the final version of the manuscript.
Funding The European Union (grants IC15-CT98-0329-EPOGH, LSHM-CT-2006-037093, HEALTH-F4-2007-201550, HEALTH-2011-278249-EU-MASCARA, ERC Advanced Grant-2011-294713-EPLORE, HEALTH-F7-305507 HOMAGE and PoC Grant 713601-uPROPHET) supported the Studies Coordinating Centre (Leuven, Belgium) and the studies in Kraków, Mirano and Novosibirsk. The Studies Coordinating Centre also received grants from the Fonds voor Wetenschappelijk Onderzoek Vlaanderen, Ministry of the Flemish Community, Brussels, Belgium (grants G.0880.13 and G.0881.13).
Competing interests None declared.
Patient consent Obtained.
Ethics approval The study complies with the Declaration of Helsinki. Each local Institutional Review Board approved the study protocol. All subjects provided informed consent in writing.
Provenance and peer review Not commissioned; externally peer reviewed.
Collaborators Belgium (Leuven) – T Kuznetsova, JA Staessen, L Thijs; Czech Republic (Pilsen and Prague) –J Filipovský, Z Marecková, J Peleška, J Seidlerová; Italy (Padua) – E Casiglia and V Tikhonoff; Poland (Kraków) – M Cwynar, J Gąsowski, T Grodzicki, K Kawecka-Jaszcz, M Kloch-Badełek, A Olszanecka, K Stolarz-Skrzypek, B Wizner, W Wojciechowska; (Gdansk) – N Gilis-Malinowska, K Kunicka, K Narkiewicz, W Sakiewicz, E Swierblewska and M Wójtowicz; Russian Federation (Novosibirsk) – T Kuznetsova, S Malyutina, Y Nikitin, A Ryabikov, and M Voevoda. Project coordinator: JA Staessen. Scientific coordinator: K Kawecka-Jaszcz. Echocardiographic study coordinator: T Kuznetsova. Steering committee: E Casiglia, J Filipovsky, K Kawecka-Jaszcz, Y Nikitin, JA Staessen. Data management committee: T Kuznetsova, JA Staessen, K Stolarz-Skrzypek, L Thijs, V Tikhonoff. Publication committee: E Casiglia, K Kawecka-Jaszcz, Y Nikitin.