Article Text

Statistics from Altmetric.com
- heart failure
- primary percutaneous coronary intervention
- remote ischaemic conditioning
- ST elevation myocardial infarction
- ventricular remodelling
Introduction
Remote ischaemic conditioning (rIC) is a non-invasive cardioprotective therapy in which serial bouts of short lived periods of ischaemia/reperfusion (I/R) in a distant organ or tissue bed confers protection to the heart during ischaemia.1 It can be performed by the inflation of a standard sphygmomanometer cuff placed on the upper arm and inflated above systolic pressure to temporarily halt blood flow, typically utilising four cycles of 5 min of cuff inflation interspersed by 5 min of complete cuff deflation.2 More recently, this process has been simplified by the development of an automated rIC device (the autoRIC Device).
The mechanisms through which rIC confers cardioprotection have not been fully elucidated but numerous animal and human models have highlighted the importance of humoral signalling acting in conjunction with neural and inflammation pathways.3 When used after the onset of ST segment elevation myocardial infarction (STEMI) and either prior to revascularisation or at the onset of reperfusion with primary percutaneous coronary intervention (P-PCI), rIC has been shown in early clinical studies to reduce the final infarct size as assessed by biomarker release, reduce the extent of left ventricular (LV) dysfunction as well as reduce major adverse cardiac and cerebral events (MACCE)4–8 although it should be noted that not all studies have been positive.9
Recently, experimental animal studies have demonstrated that in addition to its acute effect, repeated bouts of daily rIC applied after a myocardial infarction (MI) may also be beneficial. In a rat model of acute MI, Wei et al 10 induced MI by left anterior descending coronary artery (LAD) ligation and then applied rIC for 28 days, either daily or intermittently (every 3 days). They did not see any difference in infarct size but observed a dose-dependent improvement in LV remodelling as well as survival to 84 days compared with a control group given rIC only at the time of MI.10 This suggests that chronic rIC applied after an MI may confer distinct and separate benefits, especially on LV remodelling, to those from acute application at the time of MI.
The trial was designed as the first clinical study to test the hypothesis that repeated daily rIC for 4 weeks following successful revascularisation of a STEMI with P-PCI can reduce maladaptive cardiac remodelling as assessed by cardiac MRI (CMR).
Methods
Trial design and governance
The trial was a multicentre, double-blind, randomised clinical study performed at four P-PCI centres in the UK (Leicester Glenfield Hospital, Kettering General Hospital, Royal Derby Hospital and The Royal Free Hospital, London). The study was approved by the National Health Service Research Ethics Committee (12/EM/0304), registered with ClinicalTrials.gov (NCT0166461) and was conducted in accordance with the principles of Good Clinical Practice and according to the Declaration of Helsinki, under the oversight of University of Leicester (UNOLE 0306). The trial was coordinated by the National Institute for Health Research Leicester Cardiovascular Biomedical Research Unit.
Participant recruitment
The Consolidated Standards of Reporting Trials diagram for the study is shown in figure 1. The study was conducted between November 2012 and October 2016. The aim was to recruit 72 subjects who completed the study protocol (see the Statistical Analysis section). A total of 1855 patients were screened for inclusion, of which 99 were randomised. Twenty-six participants withdrew or were withdrawn after randomisation and 73 patients (38 patients in the treatment group and 35 patients in the control group) completed the study.
- Download figure
- Open in new tab
- Download powerpoint
Participant flow diagram—CONSORT (Consolidated Standards of Reporting Trials) diagram of recruitment to the trial. CMR, cardiac MRI; LVEF, left ventricular ejection fraction.
Participants were recruited from patients presenting with a first STEMI who had undergone a successful P-PCI and were not deemed to require any further intervention. Potential participants over the age of 18 were approached on the day or the day after the procedure if they met all the inclusion criteria and did not meet any exclusion criteria (box 1). Transthoracic echocardiography was performed after obtaining consent and left ventricular ejection fraction (LVEF) was calculated according to the modified Simpson Biplane method. This echocardiographic-derived LVEF assessment was used purely for assessing eligibility to the trial and was not used in the final analysis.
Trial eligibility criteria—full inclusion and exclusion criteria
Inclusion criteria
LVEF <45% on baseline echocardiogram.
First STEMI.
Successful revascularisation by P-PCI.
Able to attend research centre for baseline and 4-month follow-up appointment.
Competent to consent.
Exclusion criteria
<18 years of age.
ICD or CRTP/D in situ.
History of heart failure.
Haemoglobin <11.5 g/dL, creatinine >200 µmol/L and/or GFR <30 mL/min/m2.
Known malignancy or other comorbid condition which in the opinion of the investigator was likely to have significant negative influence on life expectancy.
Significant complications or illness following MI including cardiogenic shock, ischaemic mitral regurgitation, ventricular wall rupture, severe pericarditis or recurrent malignant arrhythmias.
CMR contraindicated or unobtainable due to claustrophobia or significantly raised BMI.
Further planned coronary interventions including surgery.
Enrolment in another clinical trial.
BMI, body mass index; CMR, cardiac MRI; CRTP/D, cardiac resynchronisation therapy/defibrillator; GFR, glomerular filtration rate; HF-PEF, heart failure with preserved ejection fraction; HF-REF, heart failure with reduced ejection fraction; ICD, implantable cardiac defibrillator; LVEF, left ventricular ejection fraction; MI, myocardial infarction; P-PCI, primary percutaneous coronary intervention; STEMI, ST segment elevation myocardial infarction.
Randomisation
Participants were block randomised according to age (<45 and ≥45), gender and infarct location (anterior vs all others) with a 1:1 allocation to the rIC or the sham group. Randomisation was conducted by using a secure randomisation web service (Sealed Envelope, London, UK). The participants, cardiologists involved in their care and study investigators analysing all outcome data were blinded to the assigned treatment group.
Implementation of treatment
All participants were given and trained in the use of a device that automatically delivers rIC or a sham treatment—the autoRIC Device, a CE marked licenced product developed by CellAegis Devices (Toronto, Canada). The device allowed self-implementation of therapy by participants in their own homes by the simple press of a button. In the active treatment (rIC) group, the device delivered 4×5 min cycles of inflation at 200 mm Hg interspersed with 5 min of deflation between each cycle with a total treatment time of 35 min. In the control group, the sham device went through the same timed cycles but with inflation only to 10 mm Hg. During the inflation period, both devices made identical vibrating noises. With ethics approval, participants were not told of the level of inflation required to deliver active treatment. Specifically, although the inflation pressure in the sham treated group was much lower, since they had not experienced a device inflated to a higher pressure, and their device appeared to deliver a ‘treatment’, they were unaware that they were in the control group. Starting on the third day following their P-PCI, participants implemented the treatment for 28 consecutive days. Participants were instructed to use the autoRIC Device at the same time of day and on the same arm. No stipulation was made as to a certain time of day, so long as the intervals between treatments were approximately 24 hours. Participants were asked to keep a diary of use of the device and were removed from the trial if they returned an incomplete diary sheet, missed more than three treatment sessions or missed more than 2 consecutive days of treatments. For those participants still in hospital at day 3, use of the device was started predischarge.
CMR outcomes
The primary endpoint was change in LVEF from participant’s baseline to 4-month follow-up scan. Secondary CMR endpoints included: changes in final LV infarct size, left ventricular end-diastolic volume index (LVEDVI), left ventricular end-systolic volume index (LVESVI) and left ventricular stroke volume index, all indexed to body surface area (BSA) between baseline and 4 months.
Participants recruited at Glenfield Hospital, Kettering General Hospital and Royal Derby Hospital had CMR performed at Glenfield Hospital and locally for those recruited at the Royal Free Hospital. All scans were supervised by cardiologists with an interest in CMR, and consisted of localisers, long axis cine images, contrast administration, a complete short axis stack for calculation of LV volumes, mass and ejection fraction (EF) and finally late gadolinium enhancement for quantification of infarct size as previously described.11 CMR analysis was undertaken at the University of Leicester core laboratory using CVI42 (Circle Cardiovascular Imaging, Calgary, Canada) by an experienced CMR observer (JRA) blinded to randomisation or temporal order of scans. Endocardial and epicardial borders were manually contoured on contiguous short axis LV slices, excluding papillary muscles and trabeculae at end-diastole and at end-systole. The following LV parameters were determined: end-diastolic volume, end-systolic volume, stroke volume, EF and myocardial mass, using well-established protocols.12 Illustrative CMR late gadolinium images at baseline and follow-up from a patient are shown in the online supplementary figure.
Supplementary file 1
Clinical outcomes and follow-up
At 4 months, MACCE comprising recurrent MI, hospitalisation for heart failure, hospitalisation not for heart failure, stroke or transient ischaemic attack, unstable angina and ischaemia driven revascularisation were documented and the Kansas City Cardiomyopathy Questionnaire (KCCQ) was completed by surviving participants to assess quality of life measures in relation to heart failure. All participants had blood samples taken before the start of rIC or sham therapy on day 3 post-P-PCI and then again on the same day as their 4-month follow-up CMR. Samples were collected in EDTA tubes, processed for plasma and stored at −80°C. A non-competitive N-terminal pro-brain natriuretic peptide (NT-proBNP) assay was used to analyse all collected plasma samples in a single batch as previously described.13
Statistical analysis
Analysis was carried out on an intention-to-treat basis. The primary outcome was the change in LVEF from baseline CMR to 4-month follow-up CMR. To inform sample size, reported changes in LVEF after MI from recent trial and registry data in the P-PCI era14–17 were combined and an estimated increase of 7.7%±7.5% in LVEF reflecting the natural recovery after MI was calculated. On the basis that rIC would increase LVEF by 5% above this natural recovery (ie, a 12.7% increase in the active treatment group) a sample of 36 in each group was needed for an alpha level 0.05% and 80% power using a two-sided test. To allow for a drop-out rate of 20%, we aimed to recruit 45 patients in each group or 90 patients in total. During the trial, we found a higher-than-expected drop-out and eventually recruited 50 patients in each group. The study was not powered to detect any differences in clinical outcomes between the two groups.
Continuous data are expressed as a mean (SD) or a median (IQR) and compared with Student’s t-test or Mann Whitney test as appropriate. Binary data are expressed as number (percentage) of patients, and comparisons were performed with Χ2 or Fisher exact test. For CMR variables and NT-proBNP, we calculated changes from baseline for each patient and the comparison of changes between two treatment groups was conducted with Mann-Whitney or Student’s t-test as appropriate. We confirmed that the data were normally distributed before undertaking analysis. A linear regression model was also fitted to compare the changes of LVEF with adjustment for important baseline variables and known predictors. We included age, gender, diabetes status, smoking status, infarct size, LVEF and presence/absence of microvascular obstruction at baseline in the initial model, and selected the final model using a backward approach. All statistical analyses were conducted using SAS V.9.4.
Results
Participants
Participants in the treatment and control groups were well matched in terms of baseline characteristics and demographics (table 1). There was a non-statistically higher proportion of smokers in the treatment group and diabetics in the control group. In both groups, the majority of infarcts were caused by LAD occlusion. All participants received drug-eluting stents; thrombus evacuation was infrequently performed. Mean post-MI echocardiography estimated LVEF before recruitment was 40% for both groups. Discharge medication was very similar between the two groups with high use of optimal medical therapy. There was no significant difference between length of hospital stay with a mean of 2.9 days in the control group and 3.0 days in the treatment group.
Demographics and clinical characteristics at baseline*
Tolerability of the autoRIC Device
Of the 26 participants who withdrew, only one (in the treatment arm) did so because they could not tolerate the device and withdrew after 2 days. No serious adverse effects were reported. There were three reports of mild discomfort when using the device, but in all cases the participants stated it was bearable and less noticeable with time. There was one report of tingling in the fingers or hands. There were no incidents of prolonged pain or of permanent marks, bruises or spots after application of the device.
CMR outcomes
Baseline CMR was performed at a median of 4 days (IQR: 4–5 days) post-P-PCI in the treatment group and 4 days (IQR: 3–6 days) in the control group (p=0.826). Follow-up CMR was performed at a median of 123 days (IQR: 122–125 days) in the treatment group and 122 days (IQR: 120–126 days) in the control group (p=0.299) after P-PCI. Of the total 73 participants who completed the study, all had LVEF assessments but two participant’s follow-up CMRs had insufficient data to allow for infarct size estimation.
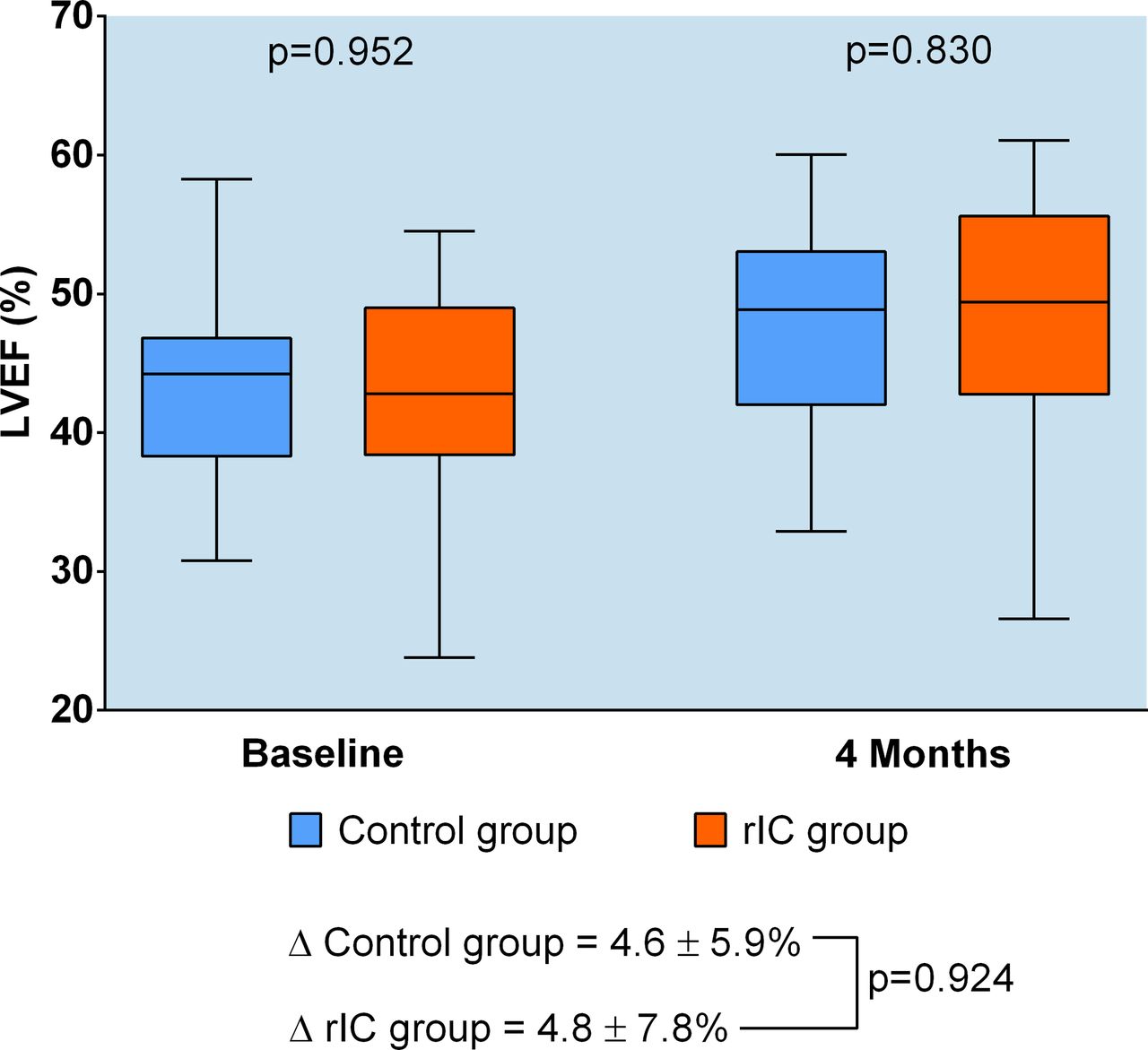
Mean baseline LVEF was not significantly different between treatment group (42.8%, IQR: 38.5–48.6) and control group (44.3%, IQR: 38.3–46.8) (p=0.952). There was no statistically significant difference in the primary endpoint of CMR assessed LVEF recovery from baseline to 4 months between the treatment and control groups (figure 2 and table 2). The mean increase in LVEF over 4 months was 4.8%±7.8% in the treatment group and 4.6%±5.9% in the control group (p=0.924). In multivariable regression analysis, infarct size (p=0.0003) and baseline LVEF (p<0.001) predicted change in LVEF at 4 months, and the effect of rIC treatment remained insignificant (p=0.862) after adjusting for these two covariates.

{kind=link}
Cardiac MRI (CMR) assessment of left ventricular ejection fraction (LVEF) at baseline and 4 months—d ifference in LVEF as assessed by CMR from baseline scan to 4-month scan in the control (blue) versus treatment (orange) groups.
CMR outcomes
With regard to secondary CMR outcomes, there were no differences at baseline in infarct size, LVESVI or prevalence of microvascular obstruction (MVO) between the treatment and control groups (table 2). Mean baseline LVEDVI was significantly higher in the treatment group (99.8 mL/m2 (84.9–114.4)) than control group (86.3 mL/m2 (76.9–95.9)) (p=0.012). However, this may mainly reflect the effect of indexing (because of the small difference in BSA between the groups, table 1) as LVEDV was not significantly different (189.5 (158.8–218.4) vs 182.0 (135.6–194.8), p=0.128). There were no significant differences between the two groups in the changes in infarct size, LVEDVI or LVESVI at 4 months (table 2). Specifically, in a multivariable analysis similar to that carried out for the change in LVEF, the change in LVEDVI between the treatment and control groups at 4 months remained not significant (p=0.972).
Clinical outcomes, quality of life and biomarkers
There was no statistically significant difference in MACCE at 4 months between the two groups, although overall numbers were small (table 3). Furthermore, there were no differences in the KCCQ outcome scores at 4 months or the change in NT-proBNP levels from baseline to 4 months (table 3).
Clinical, quality of life and biomarker outcomes
Discussion
This trial has shown that in patients who have undergone successful P-PCI for STEMI, daily rIC for 4 weeks did not result in a greater improvement in LVEF at 4 months as assessed by CMR compared with a control group that underwent sham conditioning.
rIC extends the pre-existing paradigm of local ischaemic conditioning, which has been demonstrated in numerous studies to attenuate I/R injury via a number of mechanisms including modulation of key intracellular pathways such as the reperfusion injury salvage kinase and survivor activating factor enhancement pathways, which act predominantly to inhibit opening of the mitochondrial permeability transition pore.18 A number of trials have shown that one-off rIC at around the time of P-PCI for STEMI can increase the myocardial salvage index and reduce biomarker release and that this translates to better clinical outcomes in terms of MACCE and LVEF.4–8
The rationale for this trial was provided by preclinical data,10 showing that repeatedly administered rIC over 4 weeks produced additional beneficial changes in LV function after an MI over and above that observed with a single application at the time of MI. These functional changes were accompanied by positive modulation of key remodelling processes such as a reduction in oxidative stress, attenuation of the expression of genes associated with fibrosis and hypertrophy, and blunting of the inflammatory response with reduced levels of neutrophil and macrophage infiltration in the myocardium.10 Previously, the same group had demonstrated that repetitive rIC significantly altered the behaviour of neutrophils after MI with reduced levels of adhesion at days 1 and 10 as well as a reduction in phagocytosis at day 10, apoptosis at days 1 and 10 and an overall change in the prolife of cytokine release.19 Yamaguchi et al 20 reinforced the potential of repeated rIC post-MI and implicated exosomes as mediators for signalling in rIC, possibly by their action of transferring antifibrotic microRNAs such as miR29a as well as insulin-like growth factor-1, which is known to be protective in the context of remodelling. We have shown in a rat myoblast cell culture model that that humoral modulation induced by rIC benefits a number of the maladaptive processes that contribute to post-MI remodelling including cardiomyocyte hypertrophy, differentiation of fibroblasts to pathological myofibroblasts and the upregulation of prohypertrophic and profibrotic genes.21 In human studies, Jones et al 22 have shown that daily rIC for 1 week improved endothelial function and microcirculation both locally and remotely possibly via increased STAT-3 activation triggering an increase in endothelial progenitor cells.
The use of CMR rather than echocardiography allowed for more accurate quantification of LVEF and volumes as well as allowing for the measurement of infarct size and MVO which is not possible with standard echocardiography. With regard to participant selection, we specifically looked at the effects of rIC on naïve myocardium, excluding patients with a history of MI or heart failure to examine any effect of the intervention on acute remodelling. As far as we are aware, the trial is one of the first studies where rIC was delivered chronically using an automated device. In addition to consistency, the autoRIC Device also allowed for better patient blinding, as patients in the control arm were also issued with the device and instructed in its use in an identical manner to the patients in the treatment arm. Their device was also programmed to cycle but not inflate and none of the participants were aware of the assigned treatment. Finally, the trial illustrates the challenge of undertaking studies in patients with post-STEMI LV dysfunction in the modern era of P-PCI. Over 1800 subjects are needed to be screened to identify 99 patients with an EF <45% with a substantial proportion excluded because of preserved LV function (figure 1).
This trial was designed as a proof of concept phase II study and was powered to detect a substantial increase in LVEF (5%) over the natural recovery that occurs post-STEMI. The extent of the latter was estimated from a collation of recent trial and registry studies.14–17 Despite targeting individuals with impaired LV function, the observed improvement in LVEF in the control group (4.6%±5.9%) was less than expected (7.7%±7.5%), and therefore it is possible that the level to which the study was powered or any more modest improvement due to rIC could have been missed. A post hoc power calculation based on the observed increase in LVEF in the control group suggested that to detect a 3% greater increase in the treatment arm would require a total sample size of 560 patients. It should be noted that while we did not find an effect of rIC on changes in LVEF between baseline and 4 months, in the multivariable analysis we did see a significant impact of two well-established determinants of LV remodelling, namely infarct size and baseline LVEF,23 indicating that the study was adequately powered to detect such effects. However, ultimately the goal of any therapy is to impact on clinical outcomes. There were very few such events in this trial (table 3) and it should be emphasised that the trial was not powered to detect any differences in clinical outcomes.
The trial did not implement rIC until day 3 post-MI. This is different from the experimental protocol of Wei et al 10 where the benefits of chronic rIC were observed on top of rIC applied at the time of the MI. Our rationale for delaying the implementation of rIC was to determine any potential effects of rIC on ventricular remodelling, independently of any effects on the initial infarct. This may also have impacted on the null outcome as some studies have suggested that acute remodelling begins very early postinfarct.24 25 Therefore, by instigating treatment on day 3, a number of the upstream mechanisms that can lead to maladaptive remodelling and heart failure may have already been upregulated or downregulated and the potential for rIC to modulate them may have been attenuated. Pryds et al 26 recently demonstrated that the use of a once daily rIC regimen for 4 weeks similar to that applied in this trial did not improve LVEF in patients with chronic ischaemic heart failure. This supports the theory that to reap the maximum benefits from repeated rIC post MI in terms of remodelling, treatment should be instigated early in the acute phase. The currently recruiting Chronic Remote Ischemic Conditioning to Modify Post-MI Remodelling trial (CRIC-RCT) (http://clinicaltrials.gov/NCT01817114) may answer this question as it uses a similar protocol to this trial but commences rIC at the time P-PCI.
Another potential reason for the lack of clinical translation of the beneficial effects on LV function of chronic rIC seen in the post-MI rodent model10 is the use of adjunctive therapies (including beta blockers, ACE inhibitors/angiotensin receptor blockers and mineralocorticoid receptor antagonists) in the post-MI setting in patients. These therapies have been shown to attenuate maladaptive remodelling.27–29 In the animal model, the effect of rIC was assessed naive of these treatments, whereas in this trial any benefit needed to be shown on top of these established therapies. Similarly, the effect of chronic rIC in the animal model was studied in the absence of any comorbidities. For example, diabetes mellitus has been shown to attenuate the effect of rIC30 and patients with this condition were not excluded from the study.
To enable participant blinding, patients in the control group were also given and instructed in the use of a device. Although every effort was made to make the sham devices look and behave like the treatment devices and participants were not made aware of what constituted active treatment (see the Methods section), because the sham device only inflated to a maximum pressure of 10 mm Hg it is possible that some of the control patients may have deduced that they were in the control arm. This was unavoidable. However, it should be noted that the assessment of the primary outcome (change in LVEF after 4 months with MRI) was done entirely blinded to treatment assignment and indeed the scans were assessed in a random order.
Finally, daily oversight of correct application of daily rIC was limited due to the nature of the participants’ implementing their own treatment at home. While the autoRIC Device is simple and easy to use even for very frail participants, the generation of device used during this trial had no interrogative capability to assess compliance; a subsequent device that can monitor compliance has been developed (CRICtrac, CellAegis Devices). Although it was standard practice to telephone participants regularly to monitor device use, we also relied on participant diaries, similar to ones used in drug trials, to encourage and evaluate concordance.
Conclusions
In this phase II, double-blinded, multicentre randomised controlled trial, daily rIC for 4 weeks starting on day 3 in patients with significantly impaired LV function following successful P-PCI for STEMI did not substantially improve LVEF at 4 months. Although this trial does not itself provide support for further investigation of repeated application of rIC in this setting, given its limited power it does not exclude the possibility of chronically applied rIC causing clinically meaningful improvement in LVEF post-STEMI. This trial provides valuable information on the scale of the trial that would be necessary to demonstrate such an effect in the context of contemporary treatment of STEMI and highlights other issues that may affect the outcome of such a study.
Key messages
What is already known on this subject?
Remote ischaemic conditioning (rIC) has been shown to reduce infarct size when used at the time of primary percutaneous coronary intervention (P-PCI) in ST segment elevation myocardial infarction (STEMI).
Preclinical studies have suggested the protective benefits of rIC may extend to the remodelling phase following myocardial infarction and thus may positively impact ventricular remodelling.
What might this study add?
This first-in-man phase II clinical trial compared daily rIC for 4 weeks post-STEMI treated with P-PCI with sham treatment to assess the effect of rIC on ventricular remodelling in patients with impaired left ventricular function (left ventricular ejection fraction (LVEF) <45%).
rIC was started 3 days after STEMI.
rIC did not significantly impact the primary endpoint of improvement of LVEF at 4 months postinfarct.
How might this impact on clinical practice?
Our study did not find evidence of a substantial impact on ventricular remodelling of chronic rIC administered after STEMI.
However, because of the size of the study a modest but clinically relevant effect was not ruled out.
Furthermore, rIC was started 3 days postinfarct and earlier initiation might have been more beneficial.
Future studies also need to establish any impact on clinical outcomes.
Acknowledgments
Glenfield Hospital: Jayshree Gracey, Sue Parish, Ellie Clarke, Emma Beeston, Susan Sterland, Sadat Edroos. Royal Derby Hospital: Praveen Sadarmin, Marie Appleby, Eithne Heneghan. Royal Free Hospital: Angelique Smit, Karl Salazar, Tushar Kotecha. Kettering General Hospital: Dinu Johns, Charmaine Beirnes, Lissy Jose. CMR scans were performed in the NIHR Leicester Clinical Research Facility. The authors acknowledge the financial support from the NIHR Leicester Cardiovascular Biomedical Research Unit and the Masonic Charitable Foundation. The authors also thank CellAegis Devices for providing the autoRIC Devices for the study.
References
Footnotes
Contributors APV conceived and designed the trial and drafted the manuscript. NJS provided overall supervision and was the chief investigator. All other authors were involved in either recruitment of participants or analysis of CMR or secondary outcome investigation results. All authors were involved in the final draft of the manuscript. NJS acts as the guarantor for the overall content of the work.
Funding This research received financial support from the NIHR Leicester Cardiovascular Biomedical Research Unit and the Masonic Charitable Foundation.
Competing interests None declared.
Patient consent Not required.
Ethics approval NHS Research Authority-NRES Committee East Midlands-Northhampton.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The original data to all the results outlined in the manuscript can be provided in raw format on request in an anonymised form.