
Abstract
Background:
The aim of this study was to evaluate the relationship between insulin resistance and preclinical abnormalities of the left ventricular structure and function detected in severe obesity by Color Doppler Myocardial Imaging (CDMI). Forty-eight consecutive severely obese patients (Group O) (11 males, 37 females, mean age 32.8±7 years) were enrolled. Forty-eight sex- and age-matched non-obese healthy subjects were also recruited as controls (Group C). All subjects underwent conventional 2D-Color Doppler echocardiography and CDMI. The homeostasis model assessment insulin resistance index (HOMA-IR) was used to assess insulin resistance results. Obese subjects had a greater left ventricular mass index (by height) (58.8±14 g/m2.7) than controls (37±8 g/m2.7) (P<0.0001), owing to compensation response to volume overload caused by a greater cardiac output (P<0.02). Preload reserve was increased in obese subjects, as demonstrated by a significant increase in left atrial dimension (P<0.0001). Obese patients had a slightly reduced LV diastolic function (transmitral E/A ratio: Group O, 1.1±0.8 vs Group C, 1.5 ±0.5; P<0.002). Cardiac deformation assessed by regional myocardial systolic strain and strain rate (SR) values was significantly lower (abnormal) in obese patients than in controls, both at the septum and lateral wall level. These strain and SR abnormalities were significantly related to body mass index. In addition, the early phase of diastolic function, evaluated using SR, was compromised in obese patients (P<0.001). The HOMA-IR values in obese patients were significantly higher (3.09±1.6) than those determined in the control group (0.92±0.5) (P<0.0001). The HOMA-IR values, in the obese group, were significantly related to systolic strain and SR values sampled at the septum level (P<0.0001).
Conclusion:
In conclusion, this study has demonstrated that obese patients pointed out systolic structural and functional abnormalities at a preclinical stage, in particular through strain and SR analysis; on the other hand, those altered CDMI parameters well distinguish obese subjects as compared with the control group. Furthermore, another main finding of the study was that myocardial deformation (systolic strain) could have a correlation with insulin resistance level.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others
References
Flegal KM, Carrol MD, Ogden CL, Johnson CL . Prevalence and trends in obesity among US adult, 1999–2000. JAMA 2002; 288: 1772–1773.
Bray GA . Risks of obesity. Endocrinol Metab Clin N Am 2003; 32: 787–804.
Grundy SM . Obesity, metabolic syndrome, and cardiovascular disease. J Clin Endocrinol Metab 2004; 89: 2595–2600.
Sowers JR . Obesity as a cardiovascular risk factor. Am J Med 2003; 115: 37–41.
Unger R . Minireview: weapons of lean body mass destruction: the role of ectopic lipids in the metabolic syndrome. Endocrinology 2003; 144: 5159–5165.
Szczepaniak L, Dobbins R, Metzger G, Sartoni-D'Ambrosia G, Arbique D, Vongpatanasin W et al. Myocardial triglycerides and systolic function in humans: in vivo evaluation by localized proton spectroscopy and cardiac imaging. Magn Reson Med 2003; 49: 417–423.
Petersen LR, Herrero P, Schechtman KB, Racette SB, Waggoner AD, Kisrieva-Ware Z et al. Effect of obesity and insulin resistance in myocardial substrate metabolism and efficiency in Young women. Circulation 2004; 109: 2191–2196.
Pascual M, Pascual DA, Soria F, Vicente T, Hernandez AM, Tebar FJ et al. Effects of isolated obesity on systolic and diastolic left ventricular function. Heart 2003; 89: 1152–1156.
Isaaz K, Thompson A, Ethevenot G, Cloez JL, Brembilla B, Pernot C . Doppler echocardiographic measurement of low velocity motion of the left ventricular posterior wall. Am J Cardiol 1989; 64: 66–75.
Oki T, Tabata T, Yamada H, Wakatsuki T, Mishiro Y, Abe M et al. Left ventricular diastolic properties of hypertensive patients measured by pulsed tissue Doppler imaging. J AmSoc Echocardiogr 1998; 11: 1106–1112.
Urheim S, Edvardsen T, Torp H, Angelsen B, Smiseth OA . Myocardial strain by Doppler echocardiography: validation of a new method to quantify regional myocardial function. Circulation 2000; 102: 1158–1164.
Wong Chiew Y, O'Moore-Sullivan T, Leano R, Byrne N, Beller E, Marwick TH . Abnormalities of left ventricular myocardial characteristics associated with obesity. Circulation 2004; 110: 3081–3087.
Crepaldi G, Belfiore F, Bosello O, Cavizel F, Contaldo F, Enzi G et al. Italian consensus conference-overweight, obesity and health. Int J Obes Relat Metab Disord 1991; 15: 781–790.
Grundy SM, Cleeman JI, Merz CN, Brewer Jr HB, Clark LT, Hunninghake DB . Implications of recent clinical trials for the National Cholesterol Education Program adult treatment panel III guidelines (NCEP Report). Circulation 2004; 110: 227–239.
Wallace TM, Matthews DR . The assessment of insulin resistance in man. Diabetes Med 2002; 19: 527–534.
Giorgi D, Di Bello V, Pedrinelli R, Bertini A, Talini E, Dell'Omo G et al. Ultrasonic Tissue characterization and Doppler tissue imaging in the analysis of the left ventricular function in essential arterial hypertension: a preliminary study. Echocardiography – J Cardiovasc Ultrasound Allied Techniques 2002; 3: 187–198.
Nagueh SF, Middleton KJ, Kopelen HA, Zoghbi WA, Quinones MA . Doppler tissue imaging: a non invasive technique for evaluation of left ventricular relaxation and estimation of filling pressures. J Am Coll Cardiol 1997; 30: 1527–1533.
Hooge J, Heimdal A, Jamal F, Kukulski T, Bijnens B, Rademakers F . Regional strain and SR measurements by cardiac ultrasound: principles, implementation and limitations. Eur J Echocardiogr 2000; 1: 154–170.
Weidemann F, Jamal F, Sutherland GR, Claus P, Kowalski M, Hatle L . Myocardial function defined by strain rate and strain during alterations in inotropic states and heart rate. Am J Physiol Heart Circ Physiol 2002; 283: H792–H799.
Bland JM, Altman DG . Measurement error and correlations coefficients. BMJ 1996; 313: 341–342.
Kenchaiah S, Evans JC, Levy D, Wilson PWF, Benjamin EJ, Larson MG et al. Obesity and the risk of heart failure. N Eng J Med 2002; 347: 305–313.
Iacobellis G, Ribaudo MC, Leto G, Zappaterreno A, Vecci E, Di Mario U et al. Influence of excess fat on cardiac morphology and function: Study in uncomplicated obesity. Obes Res 2002; 10: 767–773.
Iacobellis G, Ribaudo MC, Zappaterreno A, Vecci E, Tiberti C, Di Mario U et al. Relationship of insulin sensitività and left ventricular mass in uncomplicated obesity. Obes Res 2003; 11: 518–524.
Peterson LR, Waggoner AD, Schechtman KB, Meyer T, Gropler RJ, Barzilai B et al. Alteration in left ventricular structure and function in young healthy obese women. J Am Coll Card 2004; 43: 1399–1404.
Ahmed Q, Chung-Park M, Tomashefski Jr JF . Cardiopulmonary pathology in patients with sleep apnoea/obesity hypoventilation syndrome. Hum Pathol 1997; 28: 264–269.
Acknowledgements
We thank EMAC srl (Genua, Italy) for their precious technological support and Dr Giovanna Lastrucci for editorial assistance. This work was supported by ‘Centro Multidisciplinare per la Diagnosi e la Terapia dell'Obesita e dei Disturbi del Comportamento Alimentare’, University Hospital of Pisa.
Author information
Authors and Affiliations
Corresponding author
Appendices
Appendix A
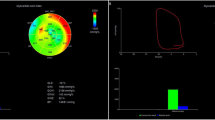
A myocardial segment contained inside a region of interest (ROI) is considered in its entirely. The frame rate ranged between 75 and 90 Hz. The ROI is bounded by four segments, two of them across the tissue and the other two parallel to the segment in a way that the enclosed area always contains the entire tissue segment during its movement. One example of such a segmental ROI is shown in Figure 1. The software automatically recognizes the moving tissue inside the outlined area and the analysis is performed on the myocardial wall segment contained inside the area. In this way, the ROI becomes a responsive area that continuously follows the wall.
The velocity along the entire segment is computed and it is then averaged across the myocardial thickness, called V(s,t), the resulting velocity, where s is the material coordinate (or the transmural level, see Figure 3), along the segment, and t indicated the time along the frames. The strain rate (Eulerian), SR(s,t), is evaluated on each frame and at every section along the segment, s, as the velocity gradient along the wall dV/ds. When the tissue is not aligned with the scan line, the velocity projected along the tissue is used. The derivative is computed by best fitting (in the least-squares sense) the slope in the V(s) profile, over a length of 2 cm about every point s. The strain (Lagrangian), St(s,t), is computed from the time integration of the SR as reported in the literature.1A, 2A, 3A

Strain is defined up to a constant value; this is fixed when a zero-strain state is automatically selected as the instant of maximum elongation over the entire selected tissue.4A, 5A The presence of uncontrolled noise in the data may lead to the appearance of a drift, a systematic trend, in the strain signal. This phenomenon is automatically eliminated here by requiring that every heartbeat must begin/close with zero trend-diastolic strain.
As described, all the quantities are computed as averaged across the thickness. This approach produces profiles that are smoother than punctual values. For this, results are evaluated and presented without any additional artificial smoothing.
Appendix references
- (1A):
-
Heimdal A, Stoilen A, Torp H, Skjarpe T. Real-time SR imaging of the left ventricle by ultrasound. J Am Soc Echocardiogr 1998; 11:1013–1019.
- (2A):
-
Edvardsen T, Gerber BL, Garot J, Bluemke DA, Lima JAO, Smiseth OA. Quantitative assessment of intrinsic regional myocardial deformation by Doppler strain rate echocardiography in humans. Circulation 2002; 106:50–56.
- (3A):
-
Sutherland GR, Stewart MJ, Groundstroem KWE, Moran CM, Fleming AD, Guell-Peris PJ, Rimersma RA, Flenn LN, Fox KAA, McDicken WN. Color Doppler myocardial imaging: a new technique for the assessment of myocardial function. J Am Soc Echocardiogr 1994;7:441–758.
- (4A):
-
Donovan CL, Armstrong WF, Bach DS. Quantitative Doppler tissue imaging of the left ventricular myocardium: validation in normal subjects. Am Heart J 1995;130:100–104.
- (5A):
-
Sutherland GR, Di Salvo G, Claus P, D'hooge J, Bijnens B. Strain and strain rate imaging: a new clinical approach to quantifying regional myocardial function. J Am Soc Echocardiogr 2004; 17:788–802.
Rights and permissions
About this article
Cite this article
Di Bello, V., Santini, F., Di Cori, A. et al. Relationship between preclinical abnormalities of global and regional left ventricular function and insulin resistance in severe obesity: a Color Doppler Imaging Study. Int J Obes 30, 948–956 (2006). https://doi.org/10.1038/sj.ijo.0803206
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ijo.0803206
Keywords
This article is cited by
-
Assessment of atrial conduction time in patients with polycystic ovary syndrome
Journal of Interventional Cardiac Electrophysiology (2014)
-
Early Subclinical Left-Ventricular Dysfunction in Obese Nonhypertensive Children: A Tissue Doppler Imaging Study
Pediatric Cardiology (2013)
-
Effect of patient and hospital characteristics on outcomes of elective ventral hernia repair in the United States
Hernia (2013)
-
Impact of body mass index on diastolic function in patients with normal left ventricular ejection fraction
Nutrition & Diabetes (2012)
-
Two‐Dimensional Strain and Twist by Vector Velocity Imaging in Adolescents With Severe Obesity
Obesity (2012)
