
Short-Term Effect of Ambient Temperature and the Risk of Stroke: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Methods and Materials
2.1. Search Strategy and Study Criteria
2.2. Study Selection
2.3. Quality Assessment
2.4. Data Extraction and Publication Bias
2.5. Statistical Analysis
2.5.1. The First Stage
2.5.2. The Second Stage
3. Results


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Authors and year of publication | Outcomes Investigated | Published journal | Location and Period of Data Obtained | Study Design | model | No. Events | Variables Controlled | Lags |
|---|---|---|---|---|---|---|---|---|
| Kyobutungi et al. [30], 2005 | stroke morbidity | Eur. J. Epidemiol. | Germany, 1998–2000 | case-crossover | conditional logistic regression model | 303 | not mention | both |
| Wang et al. [31], 2014 | emergency room visits | PLoS ONE | China, 2000–2009 | time-series | DLNM | 6,962 | air pollution, pneumonia and influenza, holidays, DOW, trends | both |
| Dawson et al. [32],2008 | stroke admissions | Acta Neurol. Scand. | Scotland, 1990–2006 | time-series | negative binomial regression | 6,389 | trends, season and DOW | null |
| Chen et al. [33], 2013 | stroke mortality | Neurology | China, 1996–2002 | time-series | GAM and DLNM | 127,750 | risk factors, socio-demographic characteristics, air pollution and relative humidity | both |
| Matsumoto et al. [34], 2010 | stroke morbidity | J. Epidemiol. | Japan, 1995–2005 | case-crossover | Multilevel logistic regression | 450 | age, obesity, smoking, total cholesterol, systolicblood pressure, diabetes, all the meteorologicalparameters | null |
| Hori et al. [35], 2012 | emergency admission | Int. J. Environ. Health Res. | Japan, 2006–2010 | time-series | generalized linear Poisson regression model | 778 | DOW, holidays, influenza, air pollution, other meteorological factors | average |
| Morabito et al. [36], 2011 | stroke admissions | Stroke | Italy, 1997–2007 | time-series | GLM | 112,870 | temporal variables, categorical factors | single day |
| Hong et al.[37], 2003 | stroke admissions | Epidemiology | Korea, 1998–2000 | case-crossover | conditional logistic regression model | 545 | humidity and air pressure | single day |
| Wang et al.[38], 2013 | hospital admissions for ischemic stroke | PLoS ONE | China, 1990–2009 | time-series | DLNM | 1,908 | season, trend, DOW and public holidays, season | both |
| Atsumi et al. [39], 2013 | cardiovascular mortality | Circ. J. | Japan, 1993–2008 | time stratified case-crossover | conditional logistic regression model | 1,709 | relative humidity and air pollution. | both |
| Mostofsky et al. [40], 2014 | stroke morbidity | Cerebrovasc. Dis. Extra | USA, 1999–2008 | Time stratified case-crossover | conditional logistic regression model | 1,763 | PM 2.5, ozone and relative humidity | both |
| Breitner et al. [41], 2014 | cardiovascular mortality | Heart | Germany, 1990–2006 | time-series | DLNM | 187,943 | trend, season, DOW, influenza, relative humidity and barometric pressure | both |
| Wang et al. [42], 2009 | stroke admissions | Int. J. Biometeorol. | Australia, 1996–2005 | time-series | GEE | 12,387 | humidity, PM10,NO2, O3 and SO2 | null |
| Cevik et al. [43], 2014 | Emergency stroke admissions | Int. J. Biometeorol. | Turkey, 2009–2010 | time-series | GAM(generalized additive models) and DLNM | 373 | wind speed and air pressure | single day |
| Basu et al.[44], 2012 | emergency room visits | Epidemiology | USA, 2005–2008 | time-series | conditional logistic regression model | 1,215,023 | air pollution | both |
| Green et al. [45], 2010 | hospital admissions | Int. J. Public Health | USA, 1995–2005 | case-crossover | conditional logistic regression model | 91,806 | season,DOW,air pollution | both |
| Zhang et al. [46], 2014 | cerebrovascular mortality | Environ. Health | China, 2004–2008 | time-series | DLNM(distributed lag nonlinear model) | 20,308 | season, trends,DOW, relative humidity, air pollution | average |
| Shaposhnikov et al. [47], 2014 | hospitalizations | Int. J. Biometeorol. | Russia, 1992–2005 | time-series | generalized linear Poisson regression model | 1,096 | DOW, and geomagnetic storms | single day |
| Lim et al. [48], 2013 | stroke mortality | Int. J. Biometeorol. | Korea, 1992–2007 | time-series | GAM GLM | 149,598 | humidity, air pressure, air pollution, DOW, season, and year | both |
| Goggins et al. [49], 2012 | stroke admissions | Int. J. Biometeorol. | China, 1999–2006 | time-series | GAM | 130,962 | DOW and holiday, air pollution, other meteorological factors, influenza rates, season and trends | both |
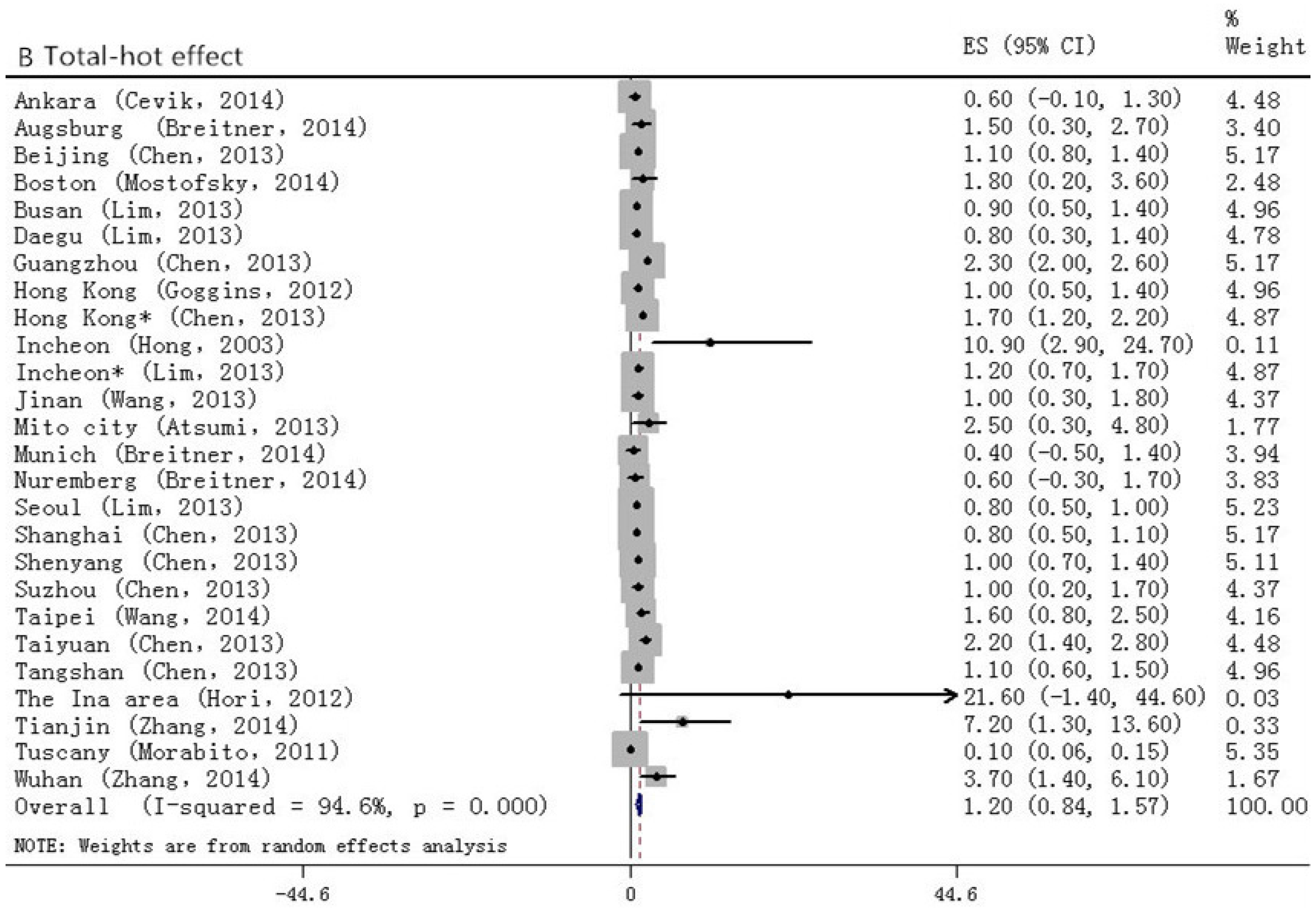
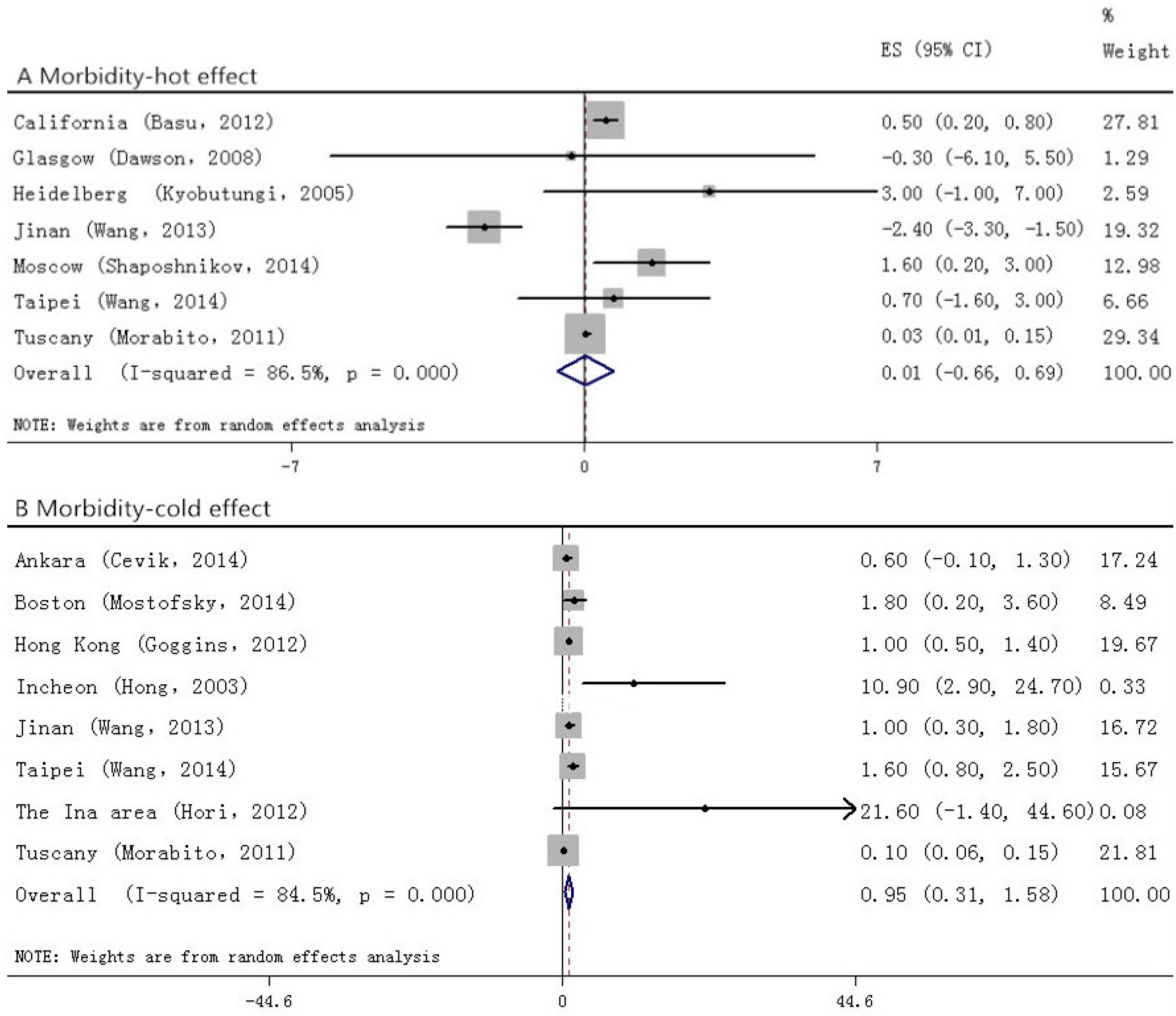
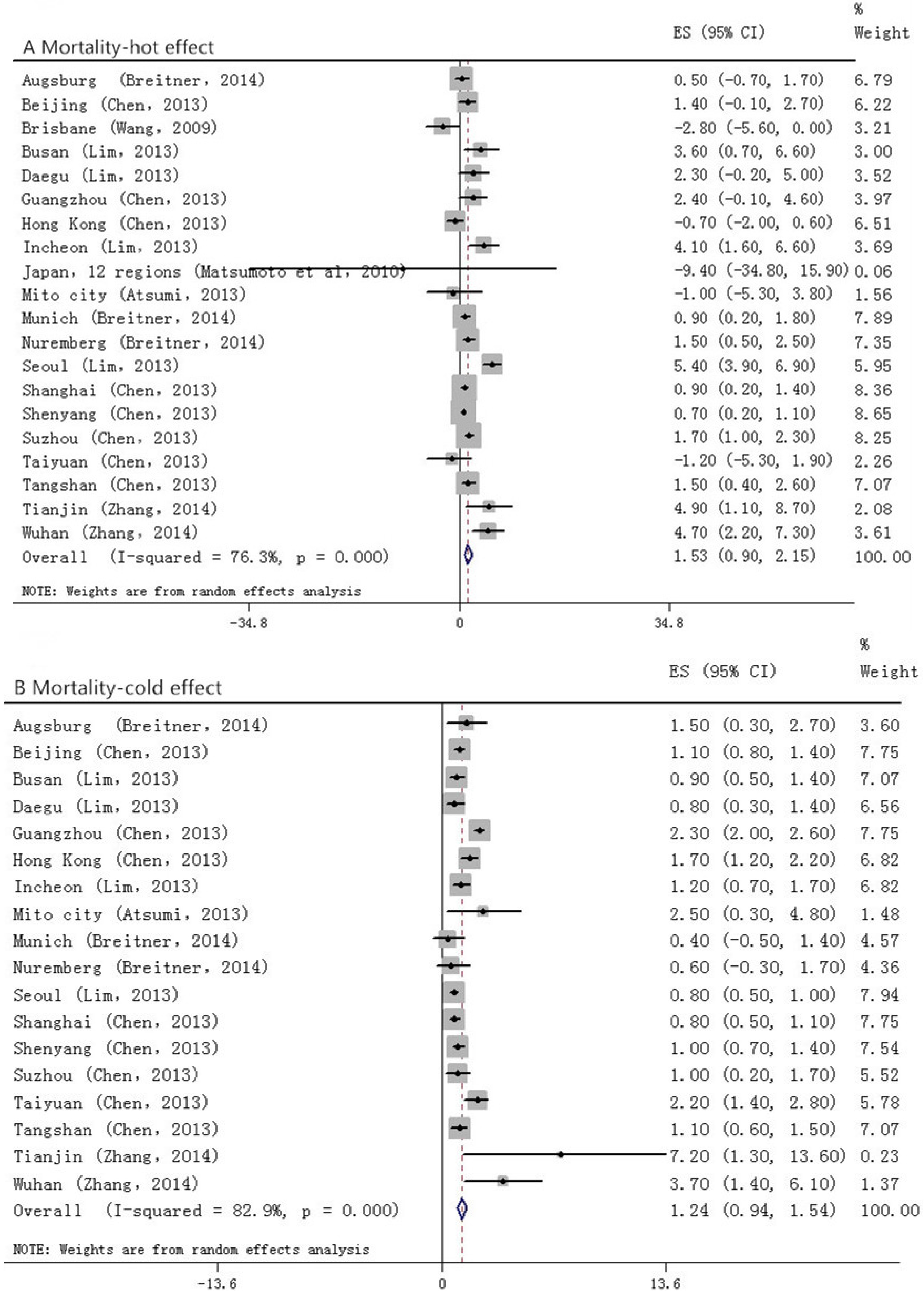
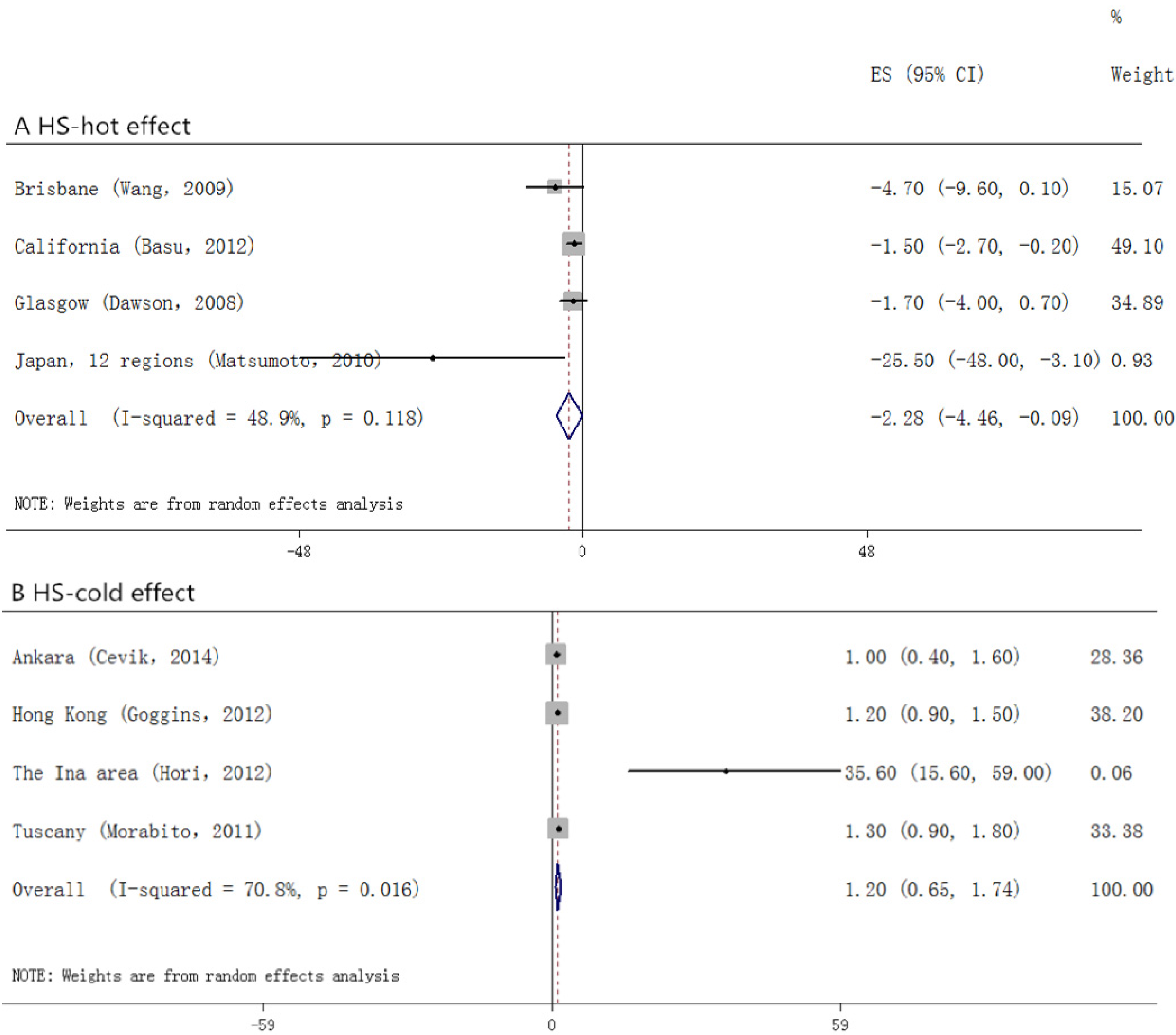
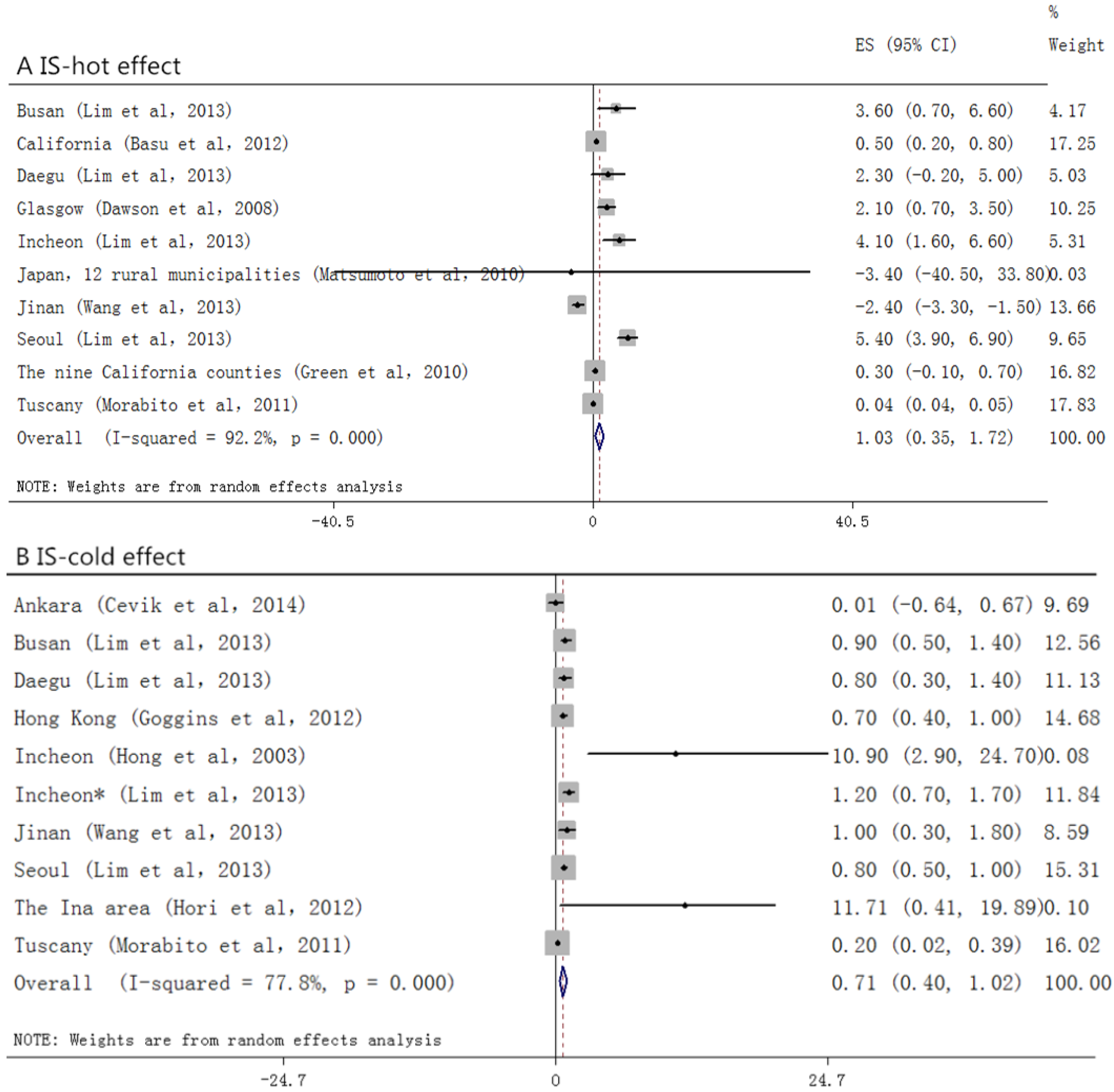
3.1. Overall Analyses
| Egger’s test, P | Total | Morbidity | Mortality | HS | IS |
|---|---|---|---|---|---|
| Hot effect | 0.196 | 1.000 | 0.536 | 0.221 | 0.803 |
| Cold effect | 0.071 | 0.711 | 0.148 | 0.734 | 0.178 |






3.2. Sensitivity Analyses
| Subtypes | <65 | ≥65 | Male | Female | Lag0 | Lag1 |
|---|---|---|---|---|---|---|
| Number of estimated areas | 7 | 7 | 6 | 6 | 6 | 3 |
| Number of estimated articles | 4 | 4 | 3 | 3 | 4 | 3 |
| Effect Size (95% CI) | 1.000 (1.000–1.001) | 1.008 (1.002–1.015) | 1.017 (1.003–1.030) | 1.019 (0.993–1.046) | 1.045 (1.007–1.082) | 1.010 (1.000–1.019) |
| Heterogeneity, I2,% | 0 | 78.4 | 0 | 62.3 | 93.2 | 9.9 |
| Publication Bias (Egger’s test, p) | 0.368 | 0.260 | 0.260 | 0.707 | 0.216 | 0.540 |
| Model | Fixed | Random | Fixed | Random | Random | Fixed |
| Age and Gender | <65 | ≥65 | Male | Female |
|---|---|---|---|---|
| Number of estimated areas | 6 | 6 | 5 | 5 |
| Number of estimated articles | 3 | 3 | 3 | 3 |
| Effect Size (95% CI) | 1.001 (1.000–1.002) | 1.005 (1.001–1.009) | 1.007 (1.002–1.011) | 1.009 (1.004–1.014) |
| Heterogeneity, I2,% | 0 | 60.9 | 40.4 | 51.8 |
| Publication Bias (Egger’s test, P) | 0.133 | 0.133 | 0.452 | 0.566 |
| Model | Fixed | Random | Random | Random |
| Subtypes | Lag0 | Lag1 | Lag2 | Lag3 | Lag4 | Lag02 |
|---|---|---|---|---|---|---|
| Number of estimated areas | 9 | 4 | 11 | 4 | 11 | 7 |
| Number of estimated articles | 6 | 4 | 4 | 4 | 4 | 3 |
| Effect Size (95% CI) | 0.999 (0.997–1.002) | 1.006 (0.996–1.016) | 1.003 (1.001–1.004) | 1.007 (1.002–1.012) | 1.002 (1.001–1.003) | 1.010 (1.000–1.021) |
| Heterogeneity, I2,% | 41.4% | 27.6 | 50.9 | 0 | 40.8 | 38.3 |
| Publication Bias (Egger’s test, P) | 0.002 | 0.308 | 0.349 | 0.734 | 0.814 | 0.764 |
| Model | Random | Random | Random | Fixed | Random | Random |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| CNKI | China National Knowledge Infrastructure |
| MACBE | major adverse cerebrovascular events |
| CI | confidence intervals |
| HS | hemorrhage stroke |
| IS | ischemic stroke |
| NE | note express |
| GBD | global burden of diseases |
| DOW | day of the week |
| RR | relative risk |
| OR | odds ratio |
| EN | expected number |
| AF | attribute fraction |
| GLM | generalized linear model |
| GAM | generalized additive models |
| GEE | generalized estimating equation |
| DLNM | distributed lag nonlinear model |
| AT | apparent temperature |
References
- Lim, S.S.; Vos, T.; Flaxman, A.D.; Danaei, G.; Shibuya, K.; Adair-Rohani, H.; AlMazroa, M.A.; Amann, M.; Anderson, H.R.; Andrews, K.G.; et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: A systematic analysis for the global burden of disease study 2010. Lancet 2012, 380, 2224–2260. [Google Scholar] [CrossRef]
- Costello, A.; Abbas, M.; Allen, A.; Ball, S.; Bell, S.; Bellamy, R.; Friel, S.; Groce, N.; Johnson, A.; Kett, M.; et al. Managing the health effects of climate change: lancet and university college London institute for global health commission. Lancet 2009, 373, 1693–1733. [Google Scholar] [CrossRef]
- Guo, Y.; Barnett, A.G.; Pan, X.; Yu, W.; Tong, S. The impact of temperature on mortality in Tianjin, China: A case-crossover design with a distributed lag nonlinear model. Environ. Health Perspect. 2011, 119, 1719–1725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, S.L.; Cakmak, S.; Hebbern, C.A.; Avramescu, M.L.; Tremblay, N. Climate change and future temperature-related mortality in 15 Canadian cities. Int. J. Biometeorol. 2012, 56, 605–619. [Google Scholar] [CrossRef] [PubMed]
- Tawatsupa, B.; Dear, K.; Kjellstrom, T.; Sleigh, A. The association between temperature and mortality in tropical middle income Thailand from 1999 to 2008. Int. J. Biometeorol. 2014, 58, 203–215. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, B.G.; Chalabi, Z.; Fenn, B.; Hajat, S.; Kovats, S.; Milojevic, A.; Wilkinson, P. Association of mortality with high temperatures in a temperate climate: England and Wales. J. Epidemiol. Community Health 2011, 65, 340–345. [Google Scholar] [CrossRef] [PubMed]
- Zanobetti, A.; Schwartz, J. Temperature and mortality in nine US cities. Epidemiology 2008, 19, 563–570. [Google Scholar] [CrossRef] [PubMed]
- Anderson, B.G.; Bell, M.L. Weather-related mortality: How heat, cold, and heat waves affect mortality in the United States. Epidemiology 2009, 20, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Curriero, F.C.; Heiner, K.S.; Samet, J.M.; Zeger, S.L.; Strug, L.; Patz, J.A. Temperature and mortality in 11 cities of the eastern United States. Am. J. Epidemiol. 2002, 155, 80–87. [Google Scholar] [CrossRef] [PubMed]
- Lozano, R.; Naghavi, M.; Foreman, K.; Lim, S.; Shibuya, K.; Aboyans, V.; Abraham, J.; Adair, T.; Aggarwal, R.; Ahn, S.Y.; et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the global burden of disease study 2010. Lancet 2012, 380, 2095–2128. [Google Scholar] [CrossRef]
- Hajat, S.; Kosatky, T. Heat-related mortality: A review and exploration of heterogeneity. J. Epidemiol. Community Health 2010, 64, 753–760. [Google Scholar] [CrossRef] [PubMed]
- Basu, R.; Feng, W.Y.; Ostro, B.D. Characterizing temperature and mortality in nine California counties. Epidemiology 2008, 19, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Barnett, A.G.; Tong, S.; Clements, A.C. What measure of temperature is the best predictor of mortality? Environ. Res. 2010, 110, 604–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [PubMed]
- Wells, G.; Parkash, R.; Healey, J.S.; Talajic, M.; Arnold, J.M.; Sullivan, S.; Peterson, J.; Yetisir, E.; Theoret-Patrick, P.; Luce, M.; et al. Cardiac resynchronization therapy: A meta-analysis of randomized controlled trials. Can. Med. Assoc. J. 2011, 183, 421–429. [Google Scholar] [CrossRef] [PubMed]
- Pieters, N.; Plusquin, M.; Cox, B.; Kicinski, M.; Vangronsveld, J.; Nawrot, T.S. An epidemiological appraisal of the association between heart rate variability and particulate air pollution: A meta-analysis. Heart 2012, 98, 1127–1135. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.; Chen, R.; Kan, H. Temperature-related mortality in 17 large Chinese cities: How heat and cold affect mortality in China. Environ. Res. 2014, 134, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Bruckner, T.A.; van den Berg, G.J.; Smith, K.R.; Catalano, R.A. Ambient temperature during gestation and cold-related adult mortality in a Swedish cohort, 1915–2002. Soc. Sci. Med. 2014, 119, 191–197. [Google Scholar] [CrossRef] [PubMed]
- Feigin, V.L.; Nikitin, Y.P.; Bots, M.L.; Vinogradova, T.E.; Grobbee, D.E. A population-based study of the associations of stroke occurrence with weather parameters in Siberia, Russia (1982–92). Eur. J. Neurol. 2000, 7, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Turner, L.R.; Connell, D.; Tong, S. The effect of heat waves on ambulance attendances in Brisbane, Australia. Prehospital Disaster Med. 2013, 28, 482–487. [Google Scholar] [CrossRef] [PubMed]
- Keim, S.M.; Mays, M.Z.; Parks, B.; Pytlak, E.; Harris, R.M.; Kent, M.A. Heat fatalities in Pima county, Arizona. Health Place 2007, 13, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Laaidi, K.; Zeghnoun, A.; Dousset, B.; Bretin, P.; Vandentorren, S.; Giraudet, E.; Beaudeau, P. The impact of heat islands on mortality in Paris during the August 2003 heat wave. Environ. Health. Perspect. 2012, 120, 254–259. [Google Scholar] [CrossRef] [PubMed]
- Stafoggia, M.; Forastiere, F.; Agostini, D.; Biggeri, A.; Bisanti, L.; Cadum, E.; Caranci, N.; de’Donato, F.; De Lisio, S.; De Maria, M.; et al. Vulnerability to heat-related mortality: A multicity, population-based, case-crossover analysis. Epidemiology 2006, 17, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.Y.; Zhang, Y.; Xu, C.Y.; Jia, B.T.; Wang, C.J.; Jia, Z.J.; Ni, H.; Wang, D.H.; Zhang, Z.; Zhao, G.; et al. Effects of meteorological elements on admission rates of cerebral infarction patients with hypertensive nephropathy from nine hospitals in Changchun city, Jilin province. Chin. Med. J. 2013, 126, 1934–1938. [Google Scholar] [PubMed]
- Bi, S.Z.; Chen, J.H.; Yuan, F.S. Study of the relationship between air temperature and stroke in Changzhi area. Chin. Crit. Care Med. 2012, 24, 556–557. [Google Scholar]
- Cheng, J.; Liu, J.; Zhang, R.; Yu, L.; Peng, J.; Chi, H.; et al. Relationship between temperature and stroke incidence in Shenzhen. Chin. J. Public Health. 2007, 23, 39–42. (in Chinese). [Google Scholar]
- Yang, J.; Liu, H.Z.; Ou, C.Q.; Lin, G.Z.; Zhou, Q.; Shen, G.C.; Chen, P.Y.; Guo, Y. Global climate change: Impact of diurnal temperature range on mortality in Guangzhou, China. Environ. Pollut. 2013, 175, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.; Zhang, J.L.; Lu, C. The relationship of temperature and stroke incidence in Beijing: a time-series study. Chin. J. Epidemiol. 2004, 25, 962–966. (in Chinese). [Google Scholar]
- Ebi, K.L.; Exuzides, K.A.; Lau, E.; Kelsh, M.; Barnston, A. Weather changes associated with hospitalizations for cardiovascular diseases and stroke in California, 1983–1998. Int. J. Biometeorol. 2004, 49, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Kyobutungi, C.; Grau, A.; Stieglbauer, G.; Becher, H. Absolute temperature, temperature changes and stroke risk: A case-crossover study. Eur. J. Epidemiol. 2005, 20, 693–698. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.C.; Lin, Y.K. Association between temperature and emergency room visits for cardiorespiratory diseases, metabolic syndrome-related diseases, and accidents in metropolitan Taipei. PLoS ONE 2014, 9, e99599. [Google Scholar] [CrossRef] [PubMed]
- Dawson, J.; Weir, C.; Wright, F.; Bryden, C.; Aslanyan, S.; Lees, K.; Bird, W.; Walters, M. Associations between meteorological variables and acute stroke hospital admissions in the west of Scotland. Acta Neurol. Scand. 2008, 117, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Wang, C.; Meng, X.; Chen, H.; Thach, T.Q.; Wong, C.M.; Kan, H. Both low and high temperature may increase the risk of stroke mortality. Neurology. 2013, 81, 1064–1070. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, M.; Ishikawa, S.; Kajii, E. Cumulative effects of weather on stroke incidence: A multi-community cohort study in Japan. J. Epidemiol. 2009, 20, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Hori, A.; Hashizume, M.; Tsuda, Y.; Tsukahara, T.; Nomiyama, T. Effects of weather variability and air pollutants on emergency admissions for cardiovascular and cerebrovascular diseases. Int. J. Environ. Health. Res. 2012, 22, 416–430. [Google Scholar] [CrossRef] [PubMed]
- Morabito, M.; Crisci, A.; Vallorani, R.; Modesti, P.A.; Gensini, G.F.; Orlandini, S. Innovative approaches helpful to enhance knowledge on weather-related stroke events over a wide geographical area and a large population. Stroke 2011, 42, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Hong, Y.C.; Rha, J.H.; Lee, J.T.; Ha, E.H.; Kwon, H.J.; Kim, H. Ischemic stroke associated with decrease in temperature. Epidemiology 2003, 14, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Gao, C.; Wang, H.; Lang, L.; Yue, T.; Lin, H. Ischemic stroke hospital admission associated with ambient temperature in Jinan, China. PLoS ONE 2013, 8, e80381. [Google Scholar] [CrossRef] [PubMed]
- Atsumi, A.; Ueda, K.; Irie, F.; Sairenchi, T.; Iimura, K.; Watanabe, H.; Iso, H.; Ota, H.; Aonuma, K. Relationship between cold temperature and cardiovascular mortality, with assessment of effect modification by individual characteristics: Ibaraki prefectural health study. Circ. J. 2013, 77, 1854–1861. [Google Scholar] [CrossRef] [PubMed]
- Mostofsky, E.; Wilker, E.H.; Schwartz, J.; Zanobetti, A.; Gold, D.R.; Wellenius, G.A.; Mittleman, M.A. Short-term changes in ambient temperature and risk of ischemic stroke. Cerebrovasc. Dis. Extra 2014, 4, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Breitner, S.; Wolf, K.; Peters, A.; Schneider, A. Short-term effects of air temperature on cause-specific cardiovascular mortality in Bavaria, Germany. Heart 2014, 100, 1272–1280. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.Y.; Barnett, A.G.; Hu, W.; Tong, S. Temperature variation and emergency hospital admissions for stroke in Brisbane, Australia, 1996–2005. Int. J. Biometeorol. 2009, 53, 535–541. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cevik, Y.; Dogan, N.O.; Das, M.; Ahmedali, A.; Kul, S.; Bayram, H. The association between weather conditions and stroke admissions in Turkey. Int. J. Biometeorol 2015, 59, 899–905. [Google Scholar] [CrossRef] [PubMed]
- Basu, R.; Pearson, D.; Malig, B.; Broadwin, R.; Green, R. The effect of high ambient temperature on emergency room visits. Epidemiology 2012, 23, 813–820. [Google Scholar] [CrossRef] [PubMed]
- Green, R.S.; Basu, R.; Malig, B. The effect of temperature on hospital admissions in nine California counties. Int. J. Public Heal. 2010, 55, 113–121. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, S.; Pan, X.; Tong, S.; Jaakkola, J.J.; Gasparrini, A.; Guo, Y.; Wang, S. The effects of ambient temperature on cerebrovascular mortality: An epidemiologic study in four climatic zones in China. Environ. Health 2014, 13. [Google Scholar] [CrossRef] [PubMed]
- Shaposhnikov, D.; Revich, B.; Gurfinkel, Y.; Naumova, E. The influence of meteorological and geomagnetic factors on acute myocardial infarction and brain stroke in Moscow, Russia. Int. J. Biometeorol. 2014, 58, 799–808. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.H.; Kim, H.; Hong, Y.C. Variation in mortality of ischemic and hemorrhagic strokes in relation to high temperature. Int. J. Biometeorol. 2013, 57, 145–153. [Google Scholar] [CrossRef] [PubMed]
- Goggins, W.B.; Woo, J.; Ho, S.; Chan, E.Y.Y.; Chau, P.H. Weather, season, and daily stroke admissions in Hong Kong. Int. J. Biometeorol. 2012, 56, 865–872. [Google Scholar] [CrossRef] [PubMed]
- Stout, R.W.; Crawford, V. Seasonal variations in fibrinogen concentrations among elderly people. Lancet 1991, 338, 9–13. [Google Scholar] [CrossRef]
- Kawahara, J.; Sano, H.; Fukuzaki, H.; Saito, K.; Hirouchi, H. Acute effects of exposure to cold on blood pressure, platelet function and sympathetic nervous activity in humans. Am. J. Hypertens. 1989, 2, 724–726. [Google Scholar] [CrossRef] [PubMed]
- Nawrot, T.S.; Staessen, J.A.; Fagard, R.H.; Van Bortel, L.M.; Struijker-Boudier, H.A. Endothelial function and outdoor temperature. Eur. J. Epidemiol. 2005, 20, 407–410. [Google Scholar] [CrossRef] [PubMed]
- Nitschke, M.; Tucker, G.R.; Bi, P. Morbidity and mortality during heatwaves in metropolitan adelaide. Med. J. Aust. 2007, 187, 662–665. [Google Scholar] [PubMed]
- Vaneckova, P.; Bambrick, H. Cause-specific hospital admissions on hot days in Sydney, Australia. PLoS ONE 2013, 8, e55459. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, M.S.; Ebi, K.L. Temperature extremes and health: Impacts of climate variability and change in the United States. J. Occup. Environ. Med. 2009, 51, 13–25. [Google Scholar] [CrossRef] [PubMed]
- Sueda, Y.; Hosomi, N.; Tsunematsu, M.; Takamatsu, K.; Nomura, E.; Torii, T.; Ohtsuki, T.; Aoki, S.; Mukai, T.; Nezu, T.; et al. Effects of meteorological conditions on the risk of ischemic stroke events in patients treated with alteplase-HEWS-tPA. J. Stroke Cerebrovasc. Dis. 2015, 24, 1500–1505. [Google Scholar] [CrossRef] [PubMed]
- Schobersberger, W.; Schobersberger, B.; Partsch, H. Travel-related thromboembolism: Mechanisms and avoidance. Expert Rev. Cardiovasc. Ther. 2009, 7, 1559–1567. [Google Scholar] [CrossRef] [PubMed]
- Strong, K.; Mathers, C.; Bonita, R. Preventing stroke: Saving lives around the world. Lancet Neurol. 2007, 6, 182–187. [Google Scholar] [CrossRef]
- Urban, A.; Davidkovova, H.; Kysely, J. Heat- and cold-stress effects on cardiovascular mortality and morbidity among urban and rural populations in the Czech Republic. Int. J. Biometeorol. 2014, 58, 1057–1068. [Google Scholar] [CrossRef] [PubMed]
- Xavier, B.; Claudio, S.; Jose, B.-G.; Payam, D.; Jordi, C.; Bart, O.; Jordi, S.; Mercedes, M.-R. Heat waves and cause-specific mortality at all ages. Epidemiology. 2011, 22, 765–772. [Google Scholar]
- Wilkinson, P.; Pattenden, S.; Armstrong, B.; Fletcher, A.; Kovats, R.S.; Mangtani, P.; McMichael, A.J. Vulnerability to winter mortality in elderly people in Britain: Population based study. Br. Med. J. 2004, 329, 647–651. [Google Scholar] [CrossRef] [PubMed]
- Sato, F.; Matsushita, S.; Hyodo, K.; Akishima, S.; Imazuru, T.; Tokunaga, C.; Enomoto, Y.; Kanemoto, S.; Hiramatsu, Y.; Sakakibara, Y. Sex difference in peripheral arterial response to cold exposure. Circ. J. 2008, 72, 1367–1372. [Google Scholar] [CrossRef] [PubMed]
- Eid, A.H.; Maiti, K.; Mitra, S.; Chotani, M.A.; Flavahan, S.; Bailey, S.R.; Thompson-Torgerson, C.S.; Flavahan, N.A. Estrogen increases smooth muscle expression of α2c-adrenoceptors and cold-induced constriction of cutaneous arteries. Am. J. Physiol. Heart Circ. Physiol. 2007, 293, H1955–H1961. [Google Scholar] [CrossRef] [PubMed]
- Bartelink, M.L.; De Wit, A.; Wollersheim, H.; Theeuwes, A.; Thien, T. Skin vascular reactivity in healthy subjects: Influence of hormonal status. J. Appl. Physiol. 1993, 74, 727–732. [Google Scholar] [PubMed]
- Cooke, J.P.; Creager, M.A.; Osmundson, P.J.; Shepherd, J.T. Sex differences in control of cutaneous blood flow. Circulation 1990, 82, 1607–1615. [Google Scholar] [CrossRef] [PubMed]
- Analitis, A.; Katsouyanni, K.; Biggeri, A.; Baccini, M.; Forsberg, B.; Bisanti, L.; Kirchmayer, U.; Ballester, F.; Cadum, E.; Goodman, P.G.; et al. Effects of cold weather on mortality: Results from 15 European cities within the PHEWE project. Am. J. Epidemiol. 2008, 168, 1397–1408. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A.; Armstrong, B.; Kovats, S.; Wilkinson, P. The effect of high temperatures on cause-specific mortality in England and Wales. Occup. Environ. Med. 2012, 69, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Krstic, G. Apparent temperature and air pollution vs. elderly population mortality in Metro Vancouver. PLoS ONE 2011, 6, e25101. [Google Scholar] [CrossRef] [PubMed]
- Li, X.Y.; Yu, X.B.; Liang, W.W.; Yu, N.; Wang, L.; Ye, X.J.; Chen, K.; Bian, P.-D. Meta-analysis of association between particulate matter and stroke attack. CNS Neurosci. Ther. 2012, 18, 501–508. [Google Scholar] [CrossRef] [PubMed]
- Dickersin, K. The existence of publication bias and risk factors for its occurrence. J. Am. Med. Assoc. 1990, 263, 1385–1389. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lian, H.; Ruan, Y.; Liang, R.; Liu, X.; Fan, Z. Short-Term Effect of Ambient Temperature and the Risk of Stroke: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2015, 12, 9068-9088. https://doi.org/10.3390/ijerph120809068
Lian H, Ruan Y, Liang R, Liu X, Fan Z. Short-Term Effect of Ambient Temperature and the Risk of Stroke: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2015; 12(8):9068-9088. https://doi.org/10.3390/ijerph120809068
Chicago/Turabian StyleLian, Hui, Yanping Ruan, Ruijuan Liang, Xiaole Liu, and Zhongjie Fan. 2015. "Short-Term Effect of Ambient Temperature and the Risk of Stroke: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 12, no. 8: 9068-9088. https://doi.org/10.3390/ijerph120809068