Article Text

Statistics from Altmetric.com
Carotid artery surgery for neurological symptoms was first reported by Eastcott and colleagues in 1954 following earlier recognition that extracranial atheroma was associated with ischaemic stroke.1 Carotid endarterectomy rapidly established itself as one of the most frequently performed procedures in the USA, largely based on surgery for asymptomatic atherosclerosis or a carotid bruit. Practice in the UK was more cautious, awaiting the results of European and US trials to clarify management of symptomatic disease with carotid stenosis of over 70%.
DIAGNOSIS OF CAROTID ARTERY DISEASE
Atherosclerosis is a generalised disease, and while symptoms may be site specific, inevitably disease elsewhere will influence the overall management of a patient. The risk of stroke is increased during coronary artery surgery for angina in the presence of asymptomatic carotid disease; conversely the risks of carotid endarterectomy are higher in patients with silent myocardial ischaemia. Early carotid artery wall disease is a predictor for coronary atherosclerosis and subsequent coronary vascular events.2
The primary symptoms of carotid atherosclerosis are neurological events and amaurosis fugax caused by embolisation from a plaque. Neurological events include transient ischaemic attacks and stroke and must be related to the contralateral side of the body from that of the stenosis. Events may be sensory, motor, or combined and on occasion are confined to intermittent dysarthria. Classically transient ischaemic attacks last less than 24 hours with full recovery. The 24 hour watershed is an epidemiological tool and does not necessarily imply the absence of permanent brain damage. Imaging by computed tomographic scan has demonstrated multiple cerebral infarcts in patients showing full recovery after transient ischaemic attacks. The frequency of attacks is variable and weeks or months may elapse between events. Multiple events within a timescale of hours (crescendo transient ischaemic attacks) carry a high risk of stroke as they may precede carotid artery thrombosis. Loss of consciousness, vertigo, diplopia and bilateral symptoms should not be attributed to carotid stenosis which is more likely to be a coincidental finding.
Within the population there is a high prevalence of asymptomatic carotid stenosis, often coincidental to other causes of neurological events. Disorders producing neurological events, transient or permanent, include:
-
intracerebral arteriovenous malformations
-
demyelinating disease
-
lacunar infarcts
-
intracranial tumours
-
arrhythmias
-
systemic hypotension.
Arterial embolisation cannot be assumed to originate from atherosclerosis of the carotid bifurcation. Alternative sources of emboli include:
-
cardiac mural thrombosis and valve disease
-
atrial fibrillation
-
left atrial myxoma
-
aortic and great vessel atherosclerosis
-
paradoxical embolus from the lower limb
-
intracranial atherosclerosis, particularly in the carotid siphon.
Symptoms of amaurosis fugax consist of intermittent loss of vision in one eye or part of an eye. They have the appearance of a mist or curtain obscuring vision.
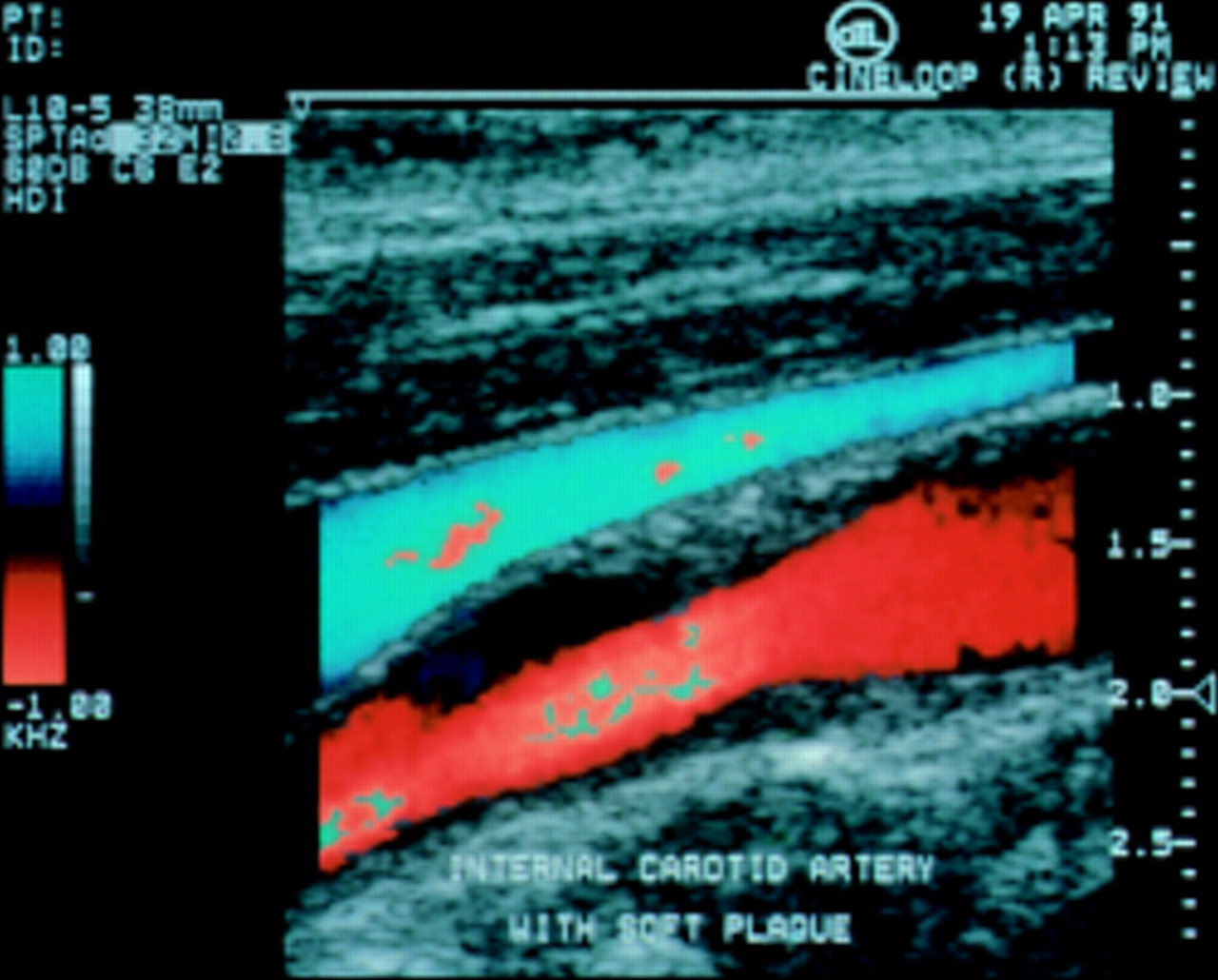
The presence of a carotid bruit is not an accurate determinant of either carotid stenosis or prognosis. It merely implies the presence of turbulence of flow together with the probability of atherosclerosis. Tight arterial stenoses may allow insufficient flow to produce a bruit. Imaging of the carotid bifurcation in patients with suspected carotid artery disease is performed using colour duplex scan which is accurate and sensitive, providing information on the degree of stenosis and plaque morphology (fig 1). Ulcerated plaque and intraplaque haemorrhage carry a poorer prognosis than endothelialised stenosis. Duplex scanning measures stenosis according to peak velocity of blood flow, but the technique can also measure arterial diameter from an image. Although it does not give the same detailed information on proximal or intracranial disease as angiography, in patients with appropriate symptoms further imaging is not required before surgery. Duplex scanning may not differentiate between a tight stenosis (95%) with “trickle flow” and an occluded carotid artery. In these cases magnetic resonance angiography provides an accurate alternative to arteriography (fig 2). There is no indication for surgery on an occluded carotid artery as the risk of embolisation has disappeared and re-establishment of flow may propel distal thrombus into the brain. There is little need in modern practice for formal intra-arterial angiography. As well as local complications at the site of arterial puncture, there is a small but significant risk of stroke even without selective carotid catheterisation. Intravenous digital angiography has proved disappointing in providing sufficient resolution of the carotid bifurcation. Carotid imaging at the time of coronary angiography should be reserved for cases where proximal arterial or intracranial disease is suspected as a cause for symptoms.
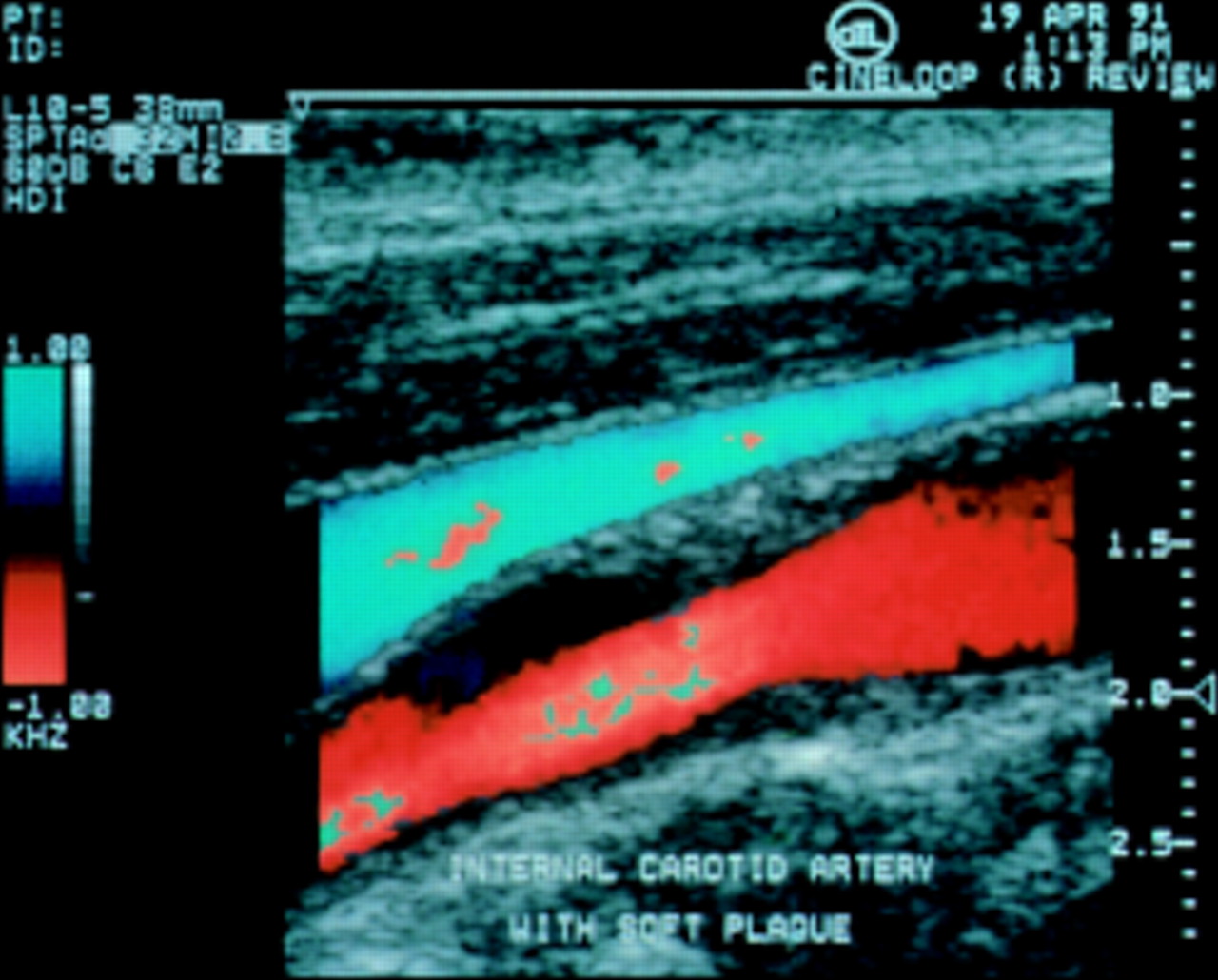
Colour duplex image showing internal carotid artery in red with a moderate stenosis characterised as soft plaque.
Characterisation of plaque may be of prognostic value.
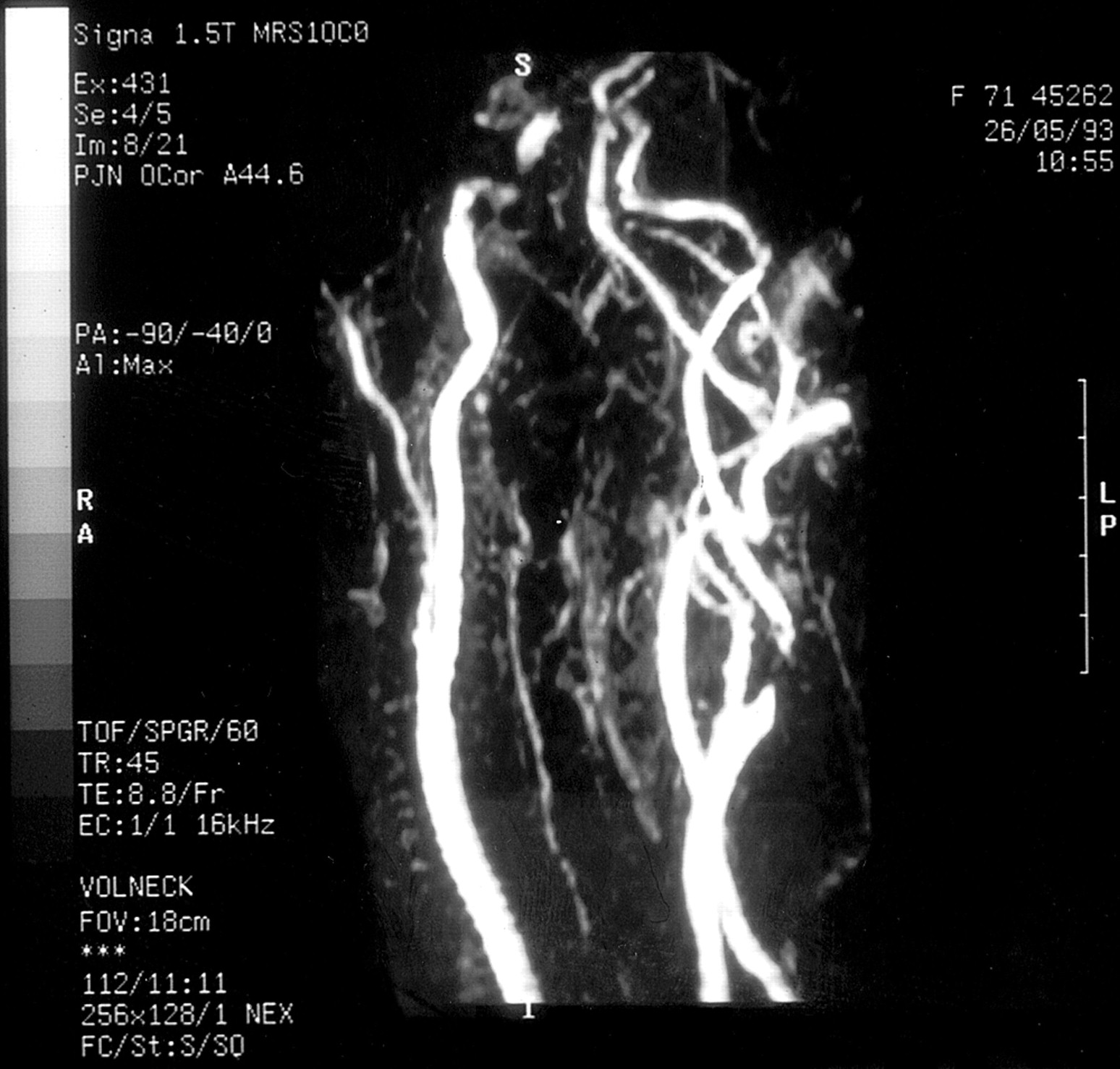
Magnetic resonance angiogram with a critical stenosis of the origin of the internal carotid artery on the right.
Duplex scan
-
No complications
-
Outpatient investigation
-
No information on intracerebral circulation
-
Requires operator expertise
-
Provides information on plaque morphology
-
May be inaccurate with `trickle flow'
-
Consider magnetic resonance angiography for tight stenoses
MANAGEMENT OF THE DISEASE PROCESS
Atherosclerosis should be treated by correction of risk factors such as hyperlipidaemia, smoking, hypertension, diabetes, and polycythaemia. In the presence of classic symptoms and appropriate carotid stenosis a decision to intervene can be based on duplex scan alone. Unless there is a contraindication, aspirin 300 mg/day will significantly reduce the incidence of further neurological events. The role of new antiplatelet agents such as clopidogrel and ticlopidine have not been subjected to trial. Anticoagulants are unproven and carry significant side effects, but may be useful when other treatment modalities have failed.
CAROTID INTERVENTION
Carotid endarterectomy under general anaesthetic carries a low mortality in fit patients. Cardiac disease was responsible for 49% of deaths in one large series of patients undergoing carotid endarterectomy with mortality due to myocardial infarction.3 Those with severe cardiac or respiratory dysfunction can be treated under cervical block or local anaesthetic, which has the advantage that neurological events are immediately identified and corrected by shunting. There is a requirement for the patient to remain immobile for the procedure which may not be tolerated, although in one series 97% of 449 patients were successfully treated under local anaesthesia.4 In one randomised controlled trial the rate of myocardial ischaemia in those treated under local anaesthetic was half that of general anaesthetic, although the results did not reach significance. The dilemma should be resolved by the multicentre general or local anaesthesia for carotid endarterectomy (GALA) trial. Carotid angioplasty is technically possible and subject to clinical multicentre trial. While the cranial nerve injuries associated with surgery are avoided, distal embolisation following carotid mobilisation can produce stroke, although this may be prevented by synchronous distal balloon occlusion of the artery. In a multicentre study of 504 patients randomised to surgery or angioplasty the combined stroke and mortality rate at 30 days was 10% for both surgery and angioplasty.5 There has been criticism of the high stroke rate in the surgical arm of this trial. Modern interventional techniques, including the use of stents together with cerebral protection devices, require further long term evaluation.
SURGERY FOR SYMPTOMATIC CAROTID STENOSIS
Symptomatic carotid stenosis carries a stroke risk of approximately 15% in the year following a motor or sensory neurological event, with the sequelae of amaurosis fugax having a more benign prognosis. While antiplatelet treatment will reduce the risk of further events to 8% per year, before 1992 the evidence for efficacy of carotid endarterectomy was not scientifically sound. Publications were based on personal series with poor classification of degree of stenosis, presence or absence of symptoms, use of antiplatelet medication, and duration of follow up.
Indications for surgery
Two multicentre randomised controlled trials have demonstrated an advantage of carotid endarterectomy combined with aspirin, compared to aspirin alone, in the prevention of stroke following a neurological event in patients with over 70% carotid stenosis. In a North American trial, patients with stroke or transient ischaemic attack within three months of entry, combined with symptomatic carotid stenosis of over 70%, were randomised to carotid endarterectomy or aspirin 1300 mg/day. The cumulative stroke risk for the surgical arm of the trial was 9% compared to 22% for medical treatment.6 A multicentre European trial, in 80 centres, randomised patients with symptomatic carotid stenosis of over 70% to surgery or best medical treatment. The qualifying neurological event for entry into the trial had to have occurred within six months previously. The cumulative risk of stroke was 12.3% for surgery compared to 21.9% for medical treatment, although the 30 day combined stroke and mortality rate for surgery was considered high at 7.5%. This may be due to some centres performing only low numbers of carotid endarterectomies.7 Despite minor differences between these two trials in terms of assessment of the carotid stenosis and time interval from qualifying event, the conclusions were that surgery has an advantage over medical treatment in symptomatic carotid stenoses of 70% or over. Pre-occlusive lesions are considered high risk for stroke although this has recently been challenged.
Transient ischaemic attack
-
Correct risk factors for atherosclerosis
-
Duplex scan
-
Add antiplatelet treatment
-
Consider surgery for carotid stenosis over 70%
-
Angioplasty acceptable in high risk patients
-
Intervention should be performed urgently
-
Carotid restenosis is rarely symptomatic
The role of surgery in patients with moderate stenosis of between 50–69% is unclear, but should be considered if symptoms are uncontrolled by conventional treatment and maximum perioperative death and disabling stroke rate of 2% can be achieved.8 Occasionally embolisation can originate from a deep ulcerated plaque in the absence of stenosis (fig 3). While endothelial remodelling may occur, surgery should be considered if antiplatelet medication fails to control symptoms.

{kind=link}
{kind=link}
{kind=link}
Digital subtraction carotid angiogram revealing a deep ulcerated plaque in the left carotid bulb and a severe irregular stenosis of the internal carotid artery on the right. Biplanar views are required to confirm the degree of stenosis on the right. The vertebral artery is filled on the left.
Complications of surgery
The success of carotid endarterectomy to prevent stroke depends on the perioperative stroke and death rate, which should be less than 3%. Factors that increase the risk of perioperative stroke include transient ischaemic attacks rather than amaurosis fugax, contralateral carotid occlusion, and irregular or ulcerated plaque at the side of surgery. There is no significant effect of age above or below 65 years on stroke rate.9 Patients must be provided with balanced information on the perioperative stroke rate and risk of damage to cranial nerves compared to non-operative management, in order to enable informed participation in their own management. An analysis of the North American symptomatic carotid endarterectomy trial revealed an overall perioperative stroke and death rate of 6.5%, with permanently disabling stroke combined with death of 2.0%. The risk of cranial nerve injuries was 8.6%, affecting the facial, hypoglossal, and vagus nerves, although the majority were described as mild in severity.9
MANAGEMENT OF ASYMPTOMATIC CAROTID STENOSIS
Asymptomatic carotid stenosis carries a stroke risk of approximately 2% per year. This stroke risk appears related to the severity of stenosis and remains constant with time, unlike the risk following a neurological event in a symptomatic carotid stenosis.2 A trial comparing surgery to aspirin for asymptomatic carotid stenosis showed no benefit from surgery although randomisation was incomplete.10 In a multicentre trial of 1662 patients (asymptomatic carotid atherosclerosis study, ACAS) with over 60% asymptomatic carotid stenoses randomised to surgery or medical treatment, at five years the combined stroke and mortality rate for surgery was 5.1% compared to 11% for medical treatment.3 Although all centres were validated for low surgical morbidity, the stroke rate associated with arteriography was considered to be high at 1.2%. There should be caution when applying the results of this trial to a wide body of surgeons, especially as the absolute risk reduction for stroke was 1% per year. While surgery carries an advantage over antiplatelet medication, 20 patients have to undergo carotid endarterectomy to prevent one stroke in every five years.3 This compares with four endarterectomies to prevent one stroke a year in symptomatic patients.6 Surgery for asymptomatic disease may not be appropriate when many healthcare systems are critically examining cost and benefit. Application of the ACAS criteria would lead to a 10 fold increase in rates of carotid endarterectomy; to put this in perspective, it is estimated that in Scotland 40 000 people would have an appropriate stenosis. The ACAS trial did not address asymptomatic stenoses in patients over 79 years old, and although many series have shown that surgery can be performed safely in octogenarians, their low life expectancy may preclude benefit from carotid endarterectomy.
CAROTID ENDARTERECTOMY IN PATIENTS UNDERGOING CORONARY ARTERY SURGERY
Coronary artery surgery carries an overall risk of stroke of 1.6% and this is increased in reoperative surgery, presence of carotid stenosis, and in those over 75 years of age.11,12 In certain subgroups the incidence is 9% and even higher in those undergoing valve surgery. Additionally, there is an excess of late neurological events following cardiovascular surgery in the presence of uncorrected carotid stenosis.13 The coexistence of symptomatic coronary artery disease and significant carotid artery stenosis ranges from 3.4–22% of the population.14 Screening for carotid artery disease in patients undergoing coronary artery surgery indicated a prevalence of 8.7% stenoses of over 75%, leading to a perioperative stroke rate of 14.3% in these patients.15 Stenoses of less than 75% were associated with a postoperative neurological deficit in 2%. Causes of stroke in the perioperative period include embolisation from the heart and great vessels, global brain ischaemia caused by hypoperfusion, air embolus, and intracranial bleeding precipitated by intraoperative anticoagulation, in addition to emboli originating from the carotid bifurcation. Increased use of off-pump coronary artery bypass may reduce the incidence of carotid related events. A prospective study of 582 patients attempted to differentiate between global and focal ischaemic events.16 Of the 12 postoperative strokes, carotid stenosis of over 50% or occlusion was significantly associated with five of seven hemispheric events but none of the five global events. Unilateral stenosis of over 80%, bilateral stenosis of over 50% or unilateral occlusion with contralateral stenosis of over 50% was associated with a 5.3% risk of hemispheric stroke. No strokes occurred in patients with unilateral 50–79% stenosis.
Although unilateral occlusion is considered of poor prognostic significance, asymptomatic patients derived no benefit from ipsilateral carotid endarterectomy compared with medical treatment alone when analysed as part of the ACAS trial. The advantage of prophylactic carotid endarterectomy in patients with over 80% carotid stenosis was shown to be significant in a retrospective non-randomised series of 68 patients undergoing synchronous or staged coronary artery surgery.17 Synchronous bilateral carotid endarterectomy was performed with 6.1% mortality, unrelated to primary cardiac or cerebrovascular events, in an unselected series of urgent and elective patients undergoing coronary artery surgery, but the number of cases was small and further studies are required.13
In patients with a primary indication for coronary revascularisation, carotid endarterectomy can be carried out safely at the time of coronary artery surgery. A retrospective analysis of 206 cases revealed a stroke or neurological deficit incidence of 3.5%.18 In 1998 Darling and colleagues demonstrated a neurological event rate of 2.9% and operative mortality of 2.4% in a prospective series of 470 patients undergoing synchronous procedures.19 A randomised trial of synchronous versus staged procedures revealed a higher stroke rate when carotid surgery followed coronary surgery. Conversely, the low morbidity and mortality of carotid endarterectomy alone in patients with coronary artery disease may not justify synchronous coronary revascularisation where this is not indicated primarily. Carotid endarterectomy under local anaesthesia or regional block may further reduce the cardiac risk in patients with coronary artery disease unsuitable for revascularisation, but needs confirmation by a randomised trial.
Patients requiring coronary revascularisation with symptomatic carotid disease that fulfil the indications for surgery should undergo carotid endarterectomy. In the absence of randomised trials, asymptomatic patients should be managed recognising the high stroke risk associated with carotid stenosis of over 80% and carotid occlusion. There is a need for randomised trials to clarify the need for carotid endarterectomy at the time of coronary artery surgery.
Acknowledgments
We are grateful for the advice of Dr Liam Penny (consultant cardiologist) and Professor Mark Wiles (professor of neurology) in the preparation of this article.
REFERENCES
Supplementary materials
WEBSITE REFERENCES FOR FURTHER READING
Akins CW. Combined carotid endarterectomy and coronary revascularisation operation. Ann Thorac Surg 1998;66:1483-4.
Baker WH, Howard VJ, Howard G, et al. Effect of contralateral occlusion on long-term efficacy of endarterectomy in the asymptomatic carotid atherosclerosis study (ACAS). Stroke 2000;31:2330-4.
Bernstein EF (Ed). Amaurosis Fugax. Springer-Verlag 1987 New York. ISBN 0-387-96601-3.
Brown MM. Identification and management of difficult stroke and TIA syndromes. J Neurol Neurosurg Psychiatry 2001;70(suppl 1):i17-i22.
Harrison MJ. Neurological complications of coronary artery bypass grafting: diffuse or focal ischaemia? Ann Thorac Surg 1995;59:1356-8.
Hertzer NR, Loop FD, Beven EG, et al. Surgical staging for simultaneous coronary and carotid disease: a study including prospective randomisation. J Vasc Surg 1989;9:455-63.
Jahangiri M, Rees GM, Edmondson SJ et al. A surgical approach to coexistent coronary and carotid artery disease. Heart 1997;77:164-7.
Mackey WC. Carotid and coronary disease: staged or simultaneous management? Semin Vasc Surg 1998;11:36-40.
Mackey WC, Khabbaz K, Bojar R, et al. Simultaneous carotid endarterectomy and coronary artery bypass: perioperative risk and long-term survival. J Vasc Surg 1996;24:58-64.
Mills SA. Risk factors for cerebral injury and cardiac surgery. Ann Thorac Surg 1995;59:1296-9.
Palerme LP, Hill AB, Obrand D, et al. Is Canadian cardiac surgeons� management of asymptomatic carotid artery stenosis at coronary artery bypass supported by the literature? Can J Surg 2000;43:93-103.
Rothwell PM, Warlow CP. Low risk of ischaemic stroke in patients with collapse of the internal carotid artery distal to severe carotid stenosis: Cerebral protection due to low post-stenotic flow? Stroke 2000;31:622-630.
Sbarigia E, DarioVizza C, Antonini M, et al. Locoregional versus general anesthesia in carotid surgery: is there an impact on perioperative myocardialischemia? Results of a prospective monocentric randomised trial. J Vasc Surg 1999;30:131-8.