Article Text

Statistics from Altmetric.com
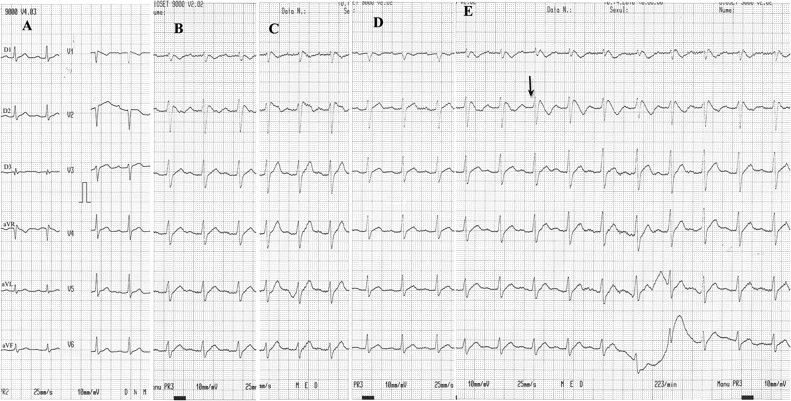
A 40-year-old man without risk factors presented to the emergency department after a recurrent syncope at rest. Despite his excessive abdominal fat, he underwent physical training (2 h every day). Family history disclosed that his father had died suddenly during sleep at the age of 43 years. Laboratory tests were normal. Baseline ECG showed a sinus rhythm of 91 bpm, first-degree atrioventricular block (PR 220 ms), narrow QRS complex (90 ms) with incomplete right bundle branch block morphology and discrete ST-segment elevation of <0.1 in lead V1 (figure 1A). Intravenous ajmaline (1 mg/kg/5 min)1 failed to induce diagnostic ECG changes (figure 1B), even after placement of the right precordial leads in a superior position to the third (figure 1C) and second (figure 1D) intercostal space.1 However, at the end of maximal inspiration a type 1 Brugada pattern was reproducibly observed (figure 1E). The patient received an implantable cardioverter-defibrillator and was discharged. After 6 months he received one shock during sleep for fast ventricular tachycardia degenerating into ventricular fibrillation.
{kind=link}
ECG recordings (25 mm/s) at baseline (A) or during ajmaline challenge (B) fail to show a diagnostic pattern, even after moving the right precordial leads to the third (C) and second (D) intercostal spaces. However, at the end of a deep inspiration (E, arrow) a type 1 Brugada pattern was reproducibly observed.
Regional conduction delays and local activation gradient reduction on the free right ventricle outflow tract wall have been described in Brugada syndrome.2 Deep inspiration may unmask a Brugada ECG owing to diaphragmatic descent with heart counterclockwise axial rotation (exposing the right ventricle outflow tract wall), augmented right ventricular filling (increased wall stress amplifying conduction anomalies) and, possibly, augmented vagal tone. The high incidence of ventricular arrhythmias during sleep may also be explained by the respiratory variations in disease expression during apnoea episodes.
Footnotes
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Clinic Emergency Hospital Bucharest.
Provenance and peer review Not commissioned; not externally peer reviewed.