Article Text

Abstract
Objective: To assess the relative influence of contractile reserve and inducible ischaemia on subsequent left ventricular volume changes after myocardial infarction.
Design: Left ventricular end diastolic and end systolic index volumes were calculated prospectively at discharge and at six months in 143 patients referred for early postinfarction dobutamine stress echocardiography. On the basis of their responses to this test, patients were divided into three groups: scar (n = 48; group 1); contractile reserve (n = 36; group 2); inducible ischaemia (n = 59; group 3).
Results: At six months, the left ventricular end diastolic index volume decreased in group 2 (mean (SD), −3.9 (9.4) ml/m2) and increased in both group 1 (+2.8 (10.6) ml/m2, p = 0.009 v group 2) and group 3 (+7.5 (11.4) ml/m2, p < 0.0001 v group 2). The end systolic index volume decreased in group 2 (−4.9 (7.3) ml/m2) and increased in both group 1 (+1.3 (8.3) ml/m2, p = 0.0015 v group 2) and group 3 (+2.8 (8.9) ml/m2, p = 0.0002 v group 2). In multivariate analysis, the contractile reserve (hazard ratio 0.19, 95% confidence interval (CI) 0.14 to 0.47), inducible ischaemia (5.86, 95% CI 1.54 to 29.7), and end systolic index volume at discharge (1.04, 95% CI 0.99 to 1.11) were independent predictors of an increase in end diastolic index volume of ⩾ 15 ml/m2 at six months.
Conclusions: Contractile reserve and inducible ischaemia, as detected by early dobutamine stress echocardiography, identify patients with differences in long term left ventricular remodelling after acute myocardial infarction.
- remodelling
- myocardial infarction
- stress echocardiography
Statistics from Altmetric.com
The development of left ventricular dilatation following myocardial infarction is the main finding in the complex process named ventricular remodelling, and it is one of the major determinants of a poor outcome.1 In previous studies, left ventricular remodelling occurred in patients with a larger infarct size2,3 and with persistent occlusion of the infarct related artery.4–6 Moreover, the transmural extent of necrosis and the presence of surviving myocardium within the infarct area were found, respectively, to be directly and inversely related to the early infarct zone expansion process.7–9 The presence of viable myocytes—generally located in the outer layers of the ventricular wall and in the peripheral areas of the infarct area—may therefore contribute to preventing left ventricular enlargement by limiting infarct expansion.
Few studies have investigated the influence of postinfarction contractile reserve on left ventricular volume changes. The favourable effect of infarct zone viability on left ventricular enlargement, as detected by early dobutamine stress echocardiography (DSE), has been shown in a population with successful primary coronary angioplasty,10 and the relative role of contractile reserve, inducible ischaemia, and their combination on left ventricular postinfarct dilatation has recently been investigated.11 However, definitive data on patients with their first uncomplicated myocardial infarction treated by a conservative approach are still lacking.
DSE is considered to be the stress test of first choice in patients with recent infarction, as it simultaneously provides reliable information on left ventricular volume and function, infarct zone contractile reserve, and residual ischaemia.12,13 Our aim in this study was to investigate the relative influence of contractile reserve and inducible ischaemia, as assessed by DSE, on postinfarction left ventricular remodelling in a general population suffering their first uncomplicated myocardial infarct and referred for conventional treatment.
METHODS
Patients and protocol
We prospectively investigated 178 patients with their first acute myocardial infarct, selected from among 224 consecutive patients admitted to the coronary intensive care unit between January 1995 and December 1996. The inclusion criteria were as follows: typical chest pain lasting more than 30 minutes; ST segment elevation in more than two leads; creatine kinase elevation to more than twice the upper limit of normal for our laboratory; segmental wall motion abnormalities on discharge; and informed written consent provided for the study. Exclusion criteria were: age more than 75 years; clinical signs of heart failure or cardiogenic shock in the first week after the infarct; predischarge angina or infarction extension; atrial fibrillation at the time of echocardiographic examination; life limiting non-cardiac diseases; and anticipated difficulties with the six month outpatient evaluation.
Of the 178 patients selected for the study, 16 (9%) were excluded because of inadequate quality of the echocardiographic examination. Later exclusions in the first six months after discharge were because of death (five patients), non-fatal reinfarction (four patients), and aortocoronary bypass procedures (five patients). Finally, five patients did not adhere to the follow up protocol. Thus 143 patients (125 men, 18 women; mean (SD) age, 58 (9) years, range 32–75 years) completed the study protocol.
The research protocol was approved by the hospital’s ethics committee. Patients received conventional medical treatment prescribed by the attending physician according to their individual needs.
All patients had a predischarge cross sectional baseline echocardiogram and DSE, on average 8 (2) days after the onset of symptoms (range 5–9 days). A follow up echocardiogram was available in all patients at a mean of 25 weeks (range 23–26 weeks) after discharge.
Echocardiographic examination
The baseline echocardiogram and DSE were done using a commercially available imaging system (HP 77020, Sonos 1500 system; 2.5 and 3.5 MHz transducers; Hewlett–Packard Inc, Andover, Massachusetts, USA). All patients underwent stress echocardiography while taking their prescribed drug treatments. Images (parasternal long and short axis views, apical four chamber and two chamber views) were displayed in real time and recorded on a high definition 0.5 inch SVHS cassette recorder. All baseline and stress images were digitally stored in quad screen format. A reference ECG signal was available on the screen during the whole examination.
First, a complete cross sectional examination was done at baseline. During continuous echocardiographic monitoring, an intravenous infusion of dobutamine (5 μg/kg body weight per minute) was started with an electronic infusion pump. This was continued for three minutes and then increased to 10 μg/kg per minute for another three minutes. After this, the dobutamine dose was increased by 10 μg/kg per minute with three minute interval steps (20, 30, and 40 μg/kg). If the heart rate was less than 85% of the age predicted limit, 0.5–1.0 mg of atropine was given and infusion of 40 μg/kg of dobutamine was maintained for three further minutes. The criteria for stopping dobutamine infusion were as follows: a heart rate exceeding 85% of the age predicted limit; hypotension (a decrease in systolic or diastolic blood pressure of more than 30 mm Hg); hypertension (systolic blood pressure above 220 mm Hg, diastolic pressure above 130 mm Hg); intolerable angina; supraventricular tachycardia; ventricular tachycardia (more than three consecutive beats); and significant ST segment depression (more than 3 mm) or ST segment elevation (more than 2 mm) in non-infarct leads.
Two experienced investigators blinded to the clinical data interpreted all the DSE results. Discrepancies were resolved by consensus. At six months, a complete baseline cross sectional echocardiogram was repeated and recorded under resting conditions.
Echocardiographic measurements
Left ventricular end diastolic and end systolic index volumes were calculated on the end diastolic and end systolic frames using the modified biplane Simpson’s rule algorithm from orthogonal apical long axis projections (four and two chambers views). The mean values of at least three measurements of the technically best cardiac cycles were taken from each examination and body surface index values (ml/m2) derived. End diastolic and end systolic index volumes at six months were compared with the values assessed at discharge to calculate the volume changes. Two expert observers analysed the left ventricular end diastolic and end systolic volumes at discharge and at six months in all patients. Thirty randomly selected echocardiographic studies were reanalysed to evaluate intraobserver and interobserver variability in calculations of left ventricular volumes.
The left ventricular ejection fraction was obtained from the following equation:

Wall motion analysis was done using a 16 segment model of the left ventricle.14 Particular attention was paid to systolic thickening in the central portion of each segment. For each segment, wall motion was scored as 1 (normal), 2 (hypokinetic), 3 (akinetic), or 4 (dyskinetic). The left ventricular wall motion score index (wall motion score/16) was calculated at baseline, during DSE, and at the follow up examination. The infarct zone was identified by segments with resting dysfunction.
DSE analysis
Contractile reserve was defined as an improvement in resting wall motion score by more than two grades during low dose dobutamine infusion (5–10 μg/kg/min). Inducible ischaemia was defined as a deterioration in wall motion score by more than two grades during DSE, either within or outside the infarct zone. Akinesis becoming dyskinesis during high dose DSE was not considered to represent inducible ischaemia. Based on the presence or absence of contractile reserve and inducible ischaemia, the DSE responses were classified as follows:
-
scar: absence of contractile reserve and inducible ischaemia
-
improvement: contractile reserve in the absence of inducible ischaemia
-
worsening: inducible ischaemia—the presence of contractile reserve at low dose in this group was defined as a “biphasic response”.
Statistical analysis
Results are expressed as mean (SD). The 95% confidence interval (CI) is given when appropriate. Differences were compared using the χ2 test for multiway frequency tables for categorical variables, and the unpaired t test for continuous variables. The left ventricular end diastolic and end systolic index volumes, ejection fraction, and wall motion score index at baseline and at follow up were compared for mean values and changes over time, using one way repeated measures analysis of variance (ANOVA), with time being the within-subject variable. Among groups, differences in the interval change of left ventricular volumes were analysed using the covariance method, adjusting each follow up measurement for the baseline values. A probability value of p < 0.05 was considered significant.
Multivariate regression analysis was done to assess the influence of basic clinical variables, resting echocardiographic data, and DSE responses on a left ventricular end diastolic volume increase of 15 ml/m2 or more at six months (15 ml/m2 is the value corresponding to the mean end diastolic volume increase in the overall population +1 SD). The variables considered were: age (continuous variable); male sex (yes/no); anterior infarction (yes/no); thrombolysis (yes/no); angiotensin converting enzyme (ACE) inhibition at discharge (yes/no); peak creatine kinase activity values (continuous variable); baseline end diastolic index volume (continuous variable); baseline end systolic index volume (continuous variable); baseline ejection fraction (continuous variable); baseline wall motion score index (continuous variable); contractile reserve at DSE (yes/no); wall motion score index decrease of more than 0.25 during low dose DSE (yes/no); inducible ischaemia at DSE (yes/no); scar at DSE (yes/no); and wall motion score index at the peak of DSE (continuous variable). Statistical analysis was done using SPSS for Windows version 8.0 (SPSS Inc, Chicago, Illinois, USA).
RESULTS
Patient characteristics and DSE responses
Patients were divided into three groups based on their DSE response. Forty eight patients were classified as having scar (group 1); 36 showed contractile reserve without subsequent inducible ischaemia and were classified as having improvement (group 2); 59 showed inducible ischaemia during the stress test and were classified as having worsening (group 3) (29 (49%) with a biphasic response). In four patients from group 3 (7%), ischaemia was induced outside the infarct zone, while in 12 (20%) the ischaemic response involved both the infarct zone and remote areas.
Revascularisation procedures (coronary angioplasty) during the follow up period were done in 15 of the 59 patients with inducible ischaemia (25%), in three of the 36 patients with contractile reserve (8%; group 3 v group 2, p = 0.073), and in seven of the 48 patients with scar (15%; group 3 v group 1, p = 0.301).
The main characteristics of these three subsets are presented in table 1. There were no significant differences in age, sex, infarct location, thrombolysis, peak creatine kinase activity, or β blockade or ACE inhibition at discharge.
Baseline clinical characteristics of the patients and the three patient groups
Mean left ventricular volumes and function
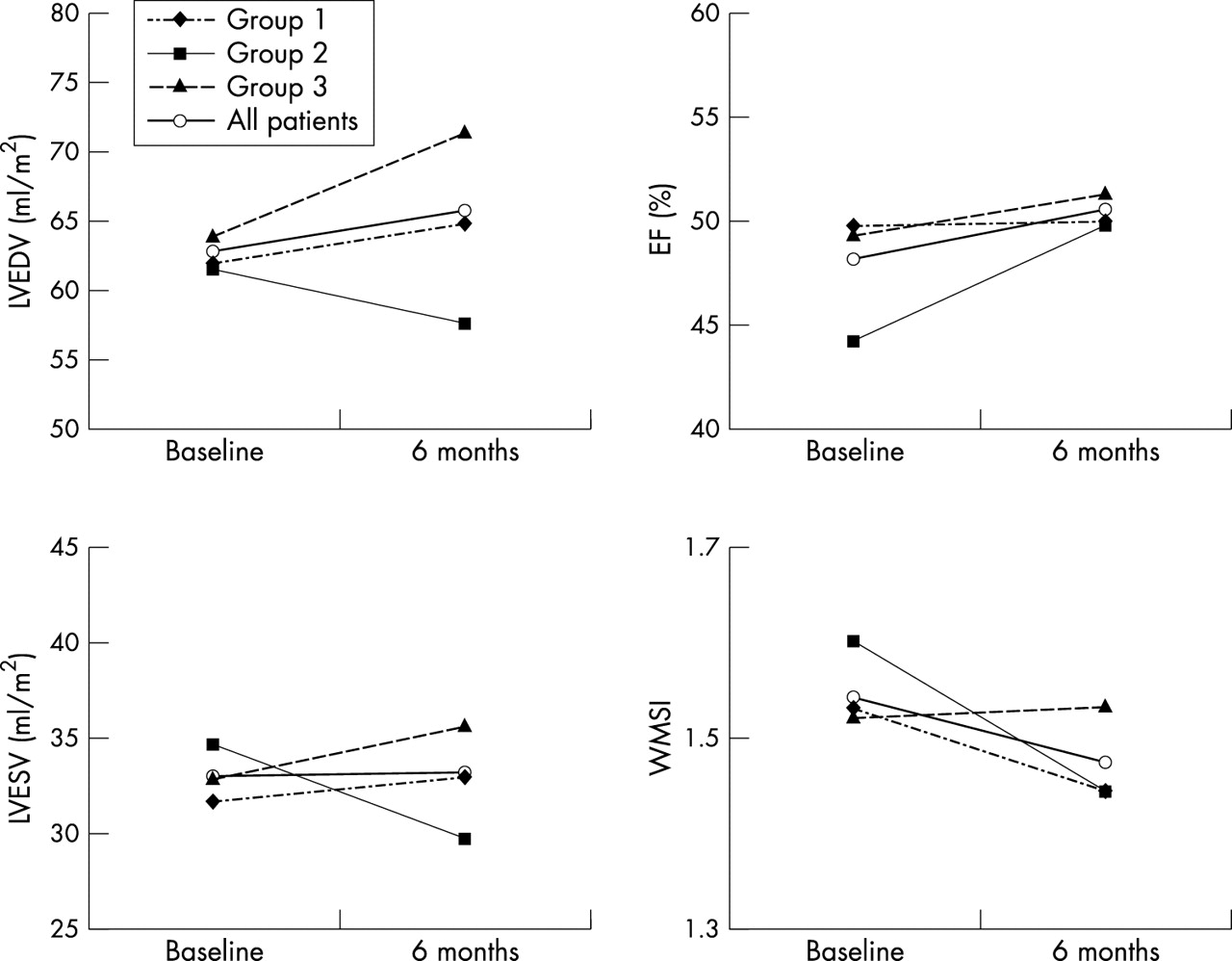
These results are shown in table 2 and fig 1. On discharge, mean left ventricular volumes, ejection fraction, and wall motion score index were comparable in the three study groups.
Baseline and six months left ventricular index volumes, ejection fraction, and wall motion score index for all patients and for the three patient groups

Left ventricular end diastolic index volume (LVEDV), left ventricular end systolic index volume (LVESV), left ventricular ejection fraction (EF), and wall motion score index (WMSI) in the overall population and in the three patient groups. The data are mean values at baseline and six months after myocardial infarction.
At six months, mean end diastolic index volume was significantly lower in the patients in group 2 than in those in group 3 (p = 0.0004), and a borderline difference was also present between the patients in group 2 and the patients in group 1 (p = 0.060). The end systolic index volume was significantly lower in the patients in group 2 than in those in group 3 (p = 0.026), while the values were comparable in the patients in groups 1 and 2. End diastolic and end systolic index volumes were comparable in the patients in groups 1 and 3 at six months.
Ejection fraction and wall motion index were comparable at six months in the three study groups.
Changes in left ventricular volumes
These results are shown in table 3. In the overall study population, the left ventricular end diastolic index volume increased at six months (p = 0.04). In contrast, the end systolic index volume remained unchanged during the observation period (p = 0.32).
Changes at six months in left ventricular index volumes, ejection fraction, and wall motion score index in all patients and in the three patient groups
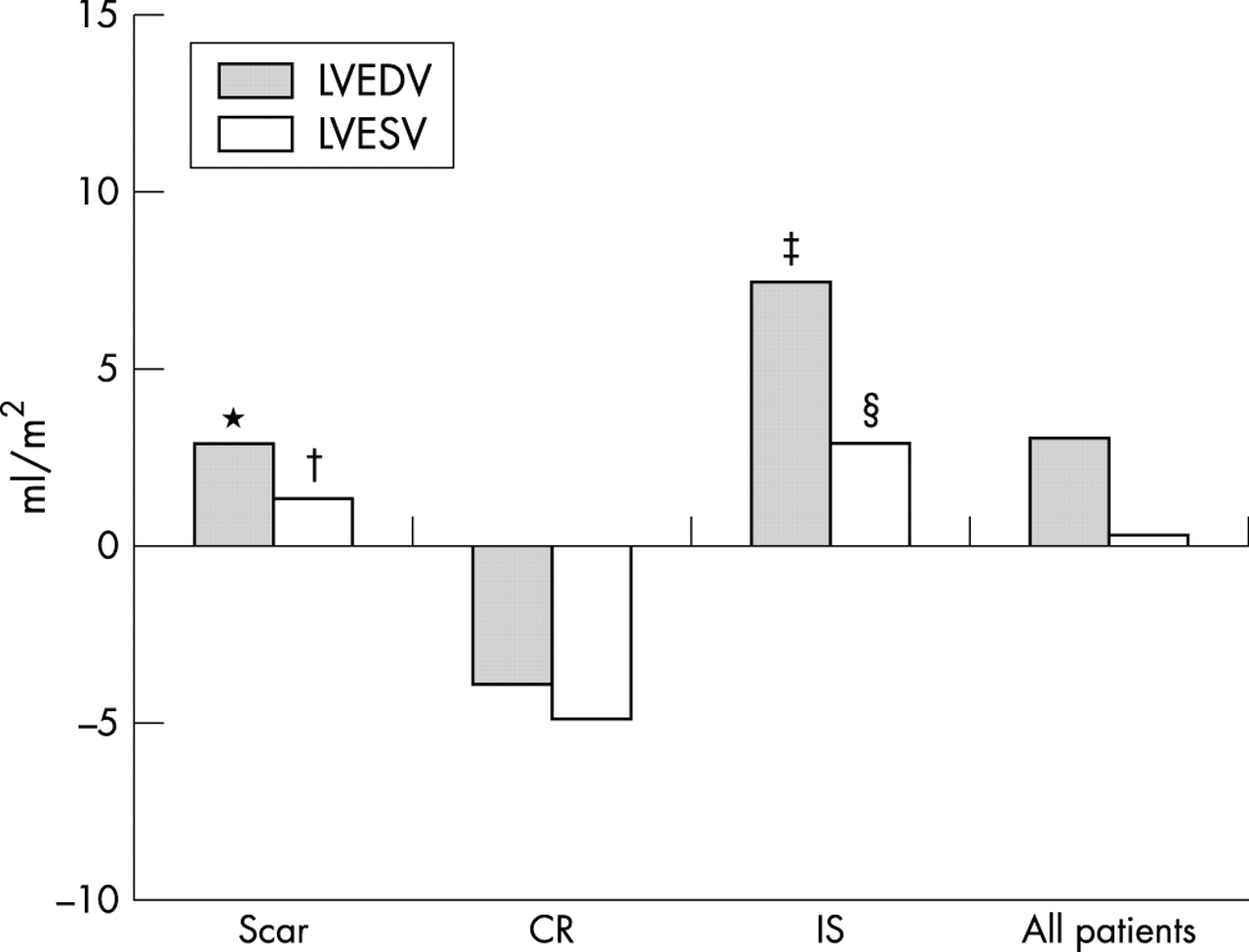
The end diastolic index volume decreased at six months in the patients in group 2, while it increased in the patients in group 1 (group 2 v group 1: p = 0.009) and in the patients in group 3 (group 2 v group 3: p < 0.0001). Similarly, the end systolic index volume decreased in group 2 and increased in group 1 (group 2 v group 1: p = 0.0015) and group 3 (group 2 v group 3: p = 0.0002). The changes in both end diastolic and end systolic index volumes were comparable in groups 1 and 3 (fig 2).

Changes (in ml/m2) at six months in left ventricular end diastolic index volume (LVEDV) and left ventricular end systolic index volume (LVESV) in the overall population and in the three patient groups. CR, contractile reserve; IS, inducible ischaemia. *p = 0.009, group 1 v group 2; †p = 0.0015, group 1 v group 2; ‡p < 0.0001, group 3 v group 2; §p = 0.0002, group 3 v group 2.
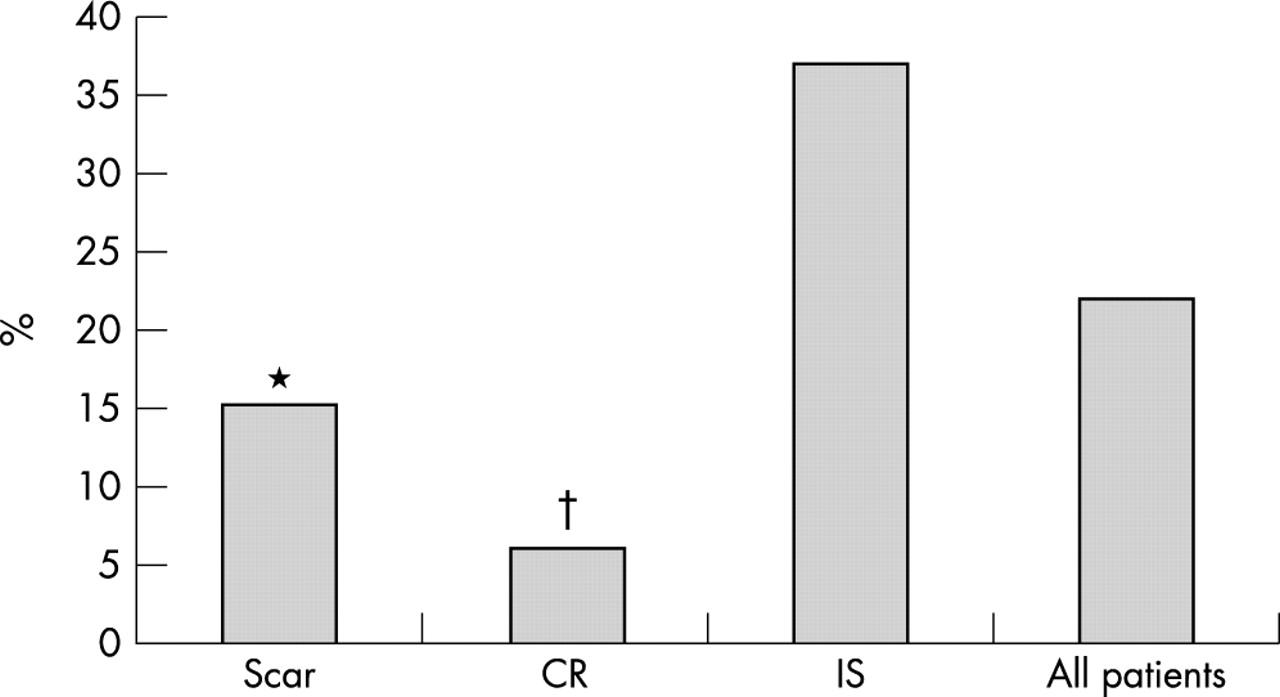
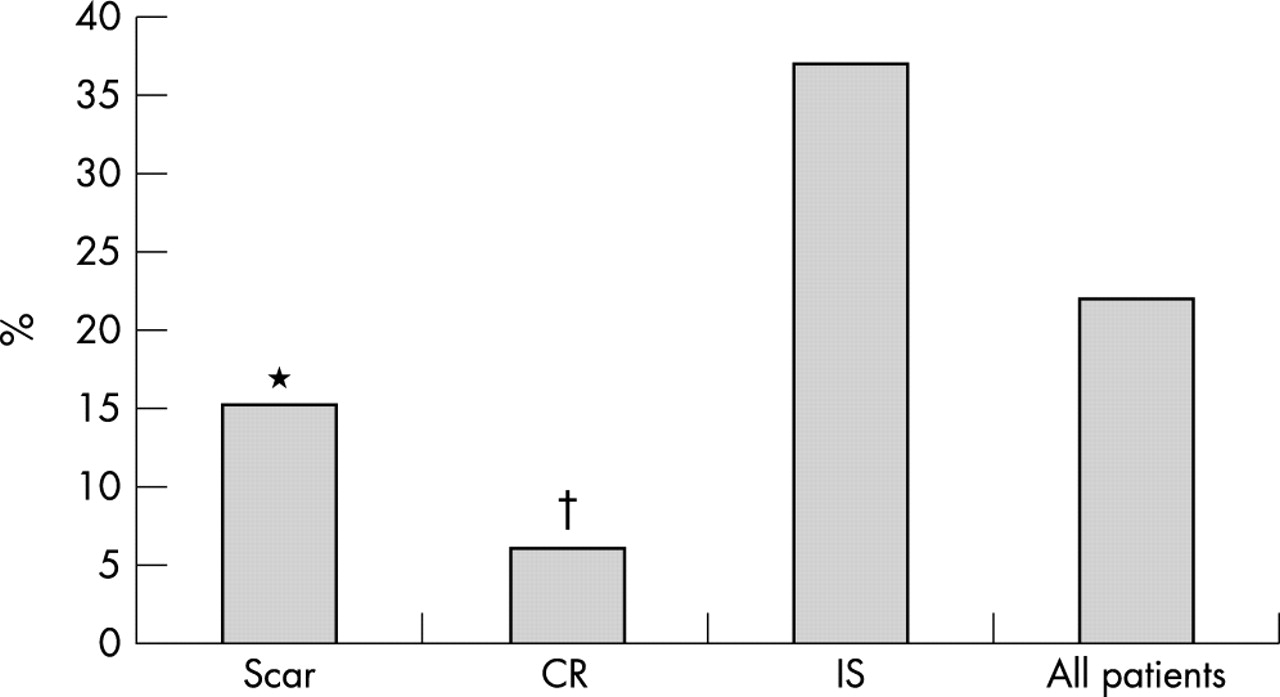
A left ventricular end diastolic volume increase of 15 ml/m2 or more was observed in seven patients in group 1 (15%), in two patients in group 2 (6%; group 2 v group 1: p = 0.344), and in 22 patients in group 3 (37%; group 3 v group 1: p = 0.020; group 3 v group 2: p = 0.002) (fig 3).
{kind=link}
{kind=link}
{kind=link}
Proportion of patients with left ventricular end diastolic index volume increase of ⩾ 15 ml/m2 at six months in the overall population and in the three patient groups. CR, contractile reserve; IS, inducible ischaemia. *p = 0.020, group 1 v group 3; †p = 0.002, group 2 v group 3.
Changes in left ventricular function indices
These results are shown in table 3. At six months, the ejection fraction increased in the overall population (p = 0.031). The wall motion index decreased slightly but not significantly (p = 0.18).
The ejection fraction improved more in group 2 than in group 1 (p = 0.025), but no differences were found between group 2 and group 3 (p = 0.17) or between group 1 and group 3 (p = 0.19). The wall motion index decreased more in group 2 than in group 1 (p = 0.003) or group 3 (p = 0.0011). Changes in wall motion score index were comparable between groups 1 and 3 (p = 0.23).
Multivariate regression analysis
On multivariate regression analysis, contractile reserve (hazard ratio 0.19, 95% CI 0.14 to 0.47), inducible ischaemia (hazard ratio 5.86, 95% CI 1.54 to 29.7), and the end systolic volume at discharge (hazard ratio 1.04, 95% CI 0.99 to 1.11) were the variables independently related to a final left ventricular end diastolic index volume increase of more than 15 ml/m2.
Reproducibility of data analysis
There was low variability (percentage difference in values) between left ventricular volume measurements made by a single observer at two time points (intraobserver variability) for left ventricular end diastolic (3.6 (4.0)) and end systolic (4.4 (3.8)) index volume calculation. When measurements were made by two independent observers (interobserver variability), analogous percentage values for variability were obtained for left ventricular end diastolic (4.2 (4.4)) and end systolic (4.8 (5.1)) index volume calculations.
DISCUSSION
In this prospective study we show that left ventricular dilatation did not occur at six months postinfarction in those patients with their first uncomplicated myocardial infarct in whom infarct zone contractile reserve was detected by predischarge DSE. Patients with improvement in contractility on DSE showed a mild decrease in left ventricular volume at six months, while those with dobutamine inducible ischaemia had significant left ventricular diastolic and systolic enlargement. Multivariate regression analysis confirmed that contractile reserve and inducible ischaemia identified by DSE at discharge were, respectively, inversely and directly related to a major left ventricular diastolic volume increase at six months. Patients with scar (neither contractile reserve nor inducible ischaemia) showed intermediate left ventricular enlargement at six months in comparison with the other two study groups. Finally, a greater improvement in ejection fraction and wall motion score index was observed at six months in patients with contractile reserve in comparison with the two other study groups. Left ventricular volumes and functional indices and the use of ACE inhibitors at discharge were comparable among the study groups; thus their influence on the results of this study should have been negligible.
Determinants of remodelling
Left ventricular remodelling is a complex process characterised by changes in shape and global dimensions of the cavity, caused by a disproportionate response to postinfarction expansion and a subsequent chronic increase in filling pressure. Infarct size,2,3 perfusion of the infarct zone,4,5 microvascular integrity,15 and a restrictive diastolic filling pattern16 interact to determine infarct expansion and remodelling.17 Conversely, the protective effect of the ACE inhibitor treatment against postinfarction left ventricular dilatation has been demonstrated in cases of delayed18,19 or early administration,20 with clinical benefits in terms of survival, heart failure prevention, and the occurrence of ischaemic events.21 The effectiveness of ACE inhibition in patients with large myocardial infarcts and impaired left ventricular function is undoubted22; however, benefits of ACE inhibition have also been shown in relation to preservation of function and limitation of infarct area.23 Several pathophysiological mechanisms seem to interfere with left ventricular remodelling, and their identification could help provide a more effective intervention strategy after acute myocardial infarction. In a recent study, different stages in the left ventricular remodelling process were shown over time, and the possibility of a long term decrease in left ventricular volume after discharge was shown in a large population with acute myocardial infarction in the GISSI III.24
Contractile reserve and remodelling
The role of infarct zone myocardial viability was convincingly demonstrated by Bolognese and colleagues in a population with successful primary angioplasty.10 In their study the presence of contractile reserve during DSE identified a lower probability of diastolic and systolic left ventricular dilatation at the one and six month assessments, and the protective effect against subsequent dilatation was unrelated to the infarct area. In another study, absent or minor contractile reserve was shown in patients with left ventricular dilatation, while a significant recruitment of regional wall motion during the DSE test was present in patients without postinfarction remodelling.25 Recently, the protective effect of contractile reserve—identified by low dose dobutamine echocardiography—against left ventricular remodelling was confirmed in 103 patients evaluated three months after acute myocardial infarction.26
The relative roles of contractile reserve and inducible ischaemia, as assessed by predischarge DSE, have been evaluated in 30 patients with their first myocardial infarct.11 In that study, the absence of contractile reserve was an independent predictor of postinfarction remodelling, whereas residual ischaemia was equally present in patients with or without left ventricular dilatation.
The results of the present study confirm the protective effect of contractile reserve in patients with infarct zone stunning, according to the meaning of the sustained improvement in contractility during DSE.13 The infarct area reperfusion in these patients was not demonstrable because of the lack of coronary angiography, but the significant wall motion score index decrease observed in patients with contractile reserve supports the view that myocardial stunning was prevalent.
Inducible ischaemia and remodelling
The role of exertional ischaemia in determining left ventricular remodelling has been shown in patients with anterior myocardial infarction and poor left ventricular function.27 As with residual exertional ischaemia, worsening of contractility during DSE indicates the presence of viable myocardium in jeopardy.13 In these patients a progressive loss of viable myocytes can occur over time, determining delayed infarct expansion and consequent long term left ventricular dilatation. Absence of remodelling was demonstrated after revascularisation of totally occluded infarct related arteries, whereas left ventricular dilatation was observed in patients with patent though stenosed infarct related arteries.28
In our study, the occurrence of inducible ischaemia during DSE after uncomplicated myocardial infarction clearly identified patients with left ventricular enlargement at six months, and with a higher risk of major end diastolic volume increase (> 15 ml/m2) (fig 3).
Changes in function indices
In a previous report, changes in left ventricular diastolic and systolic volumes over the time determined higher ejection fraction values at one and six months in patients with contractile reserve.10 In our study, both left ventricular ejection fraction and wall motion score index improved slightly at six months in the overall population, but this favourable change was particularly evident in patients with contractile reserve. A definite relation between long term left ventricular remodelling and systolic function after myocardial infarction remains controversial and further prospective studies are necessary to fully clarify this question.
Clinical implications
A positive DSE response for the presence of inducible ischaemia should be considered not only in the light of a more aggressive anti-ischaemic strategy, but also in relation to the effect of residual ischaemia on subsequent left ventricular remodelling. To avoid further left ventricular enlargement, patients with inducible ischaemia referred for medical treatment or with unsuccessful revascularisation procedures should be considered for full dose ACE inhibition, whereas patients with scar or with contractile reserve at DSE are at a minor or even absent risk of remodelling. Thus DSE at discharge helps clinicians not only to optimise anti-ischaemic treatment on an individual basis but also to prevent the remodelling process in these high risk patients.
Limitations of the study
Our study had some methodological limitations. Infarct related coronary flow status is considered to be one of the major determinants of postinfarction remodelling, and the long term persistence of perfusion in the infarct zone is related to the presence of hibernating or non-ischaemic myocardium, depending on the entity of flow. In our study we did not undertake coronary angiography as part of the protocol, because the population was representative of the wide range of clinical presentations occurring with small uncomplicated myocardial infarcts. In such patients, systematic predischarge and six month coronary angiography would have been unethical and expensive. The purpose of the study was to evaluate the role of predischarge contractile reserve and inducible ischaemia as detected by non-invasive methods, and DSE has been shown to be a safe and accurate diagnostic tool in this group of patients, reliably discriminating the presence of stunning and hibernation in the infarct area.29
The referring physician was not blinded to the DSE results, so a higher proportion of patients with inducible ischaemia was referred for coronary angiography and angioplasty during the first six months after myocardial infarction. This interfered with the results of the study, probably reducing the occurrence of long term left ventricular dilatation in patients with mechanically restored infarct related coronary blood flow. However, a greater degree of left ventricular dilatation was shown in patients with inducible ischaemia, although this group was comprised of those referred for coronary artery angioplasty.
Data on the long term (later than six months) volume response in the population of our study are lacking for logistic reasons. To investigate the long term role of residual contractile reserve and inducible ischaemia in patients with myocardial infarction could give valuable information, but the interference of further clinical events, such as new acute coronary syndromes or revascularisation procedures, increases with time and thus greatly reduces the sample population. A six month interval seemed a fair compromise to establish the extent of left ventricular remodelling in patients with coronary artery disease, considering the characteristics of the disease.
Conclusions
After a first uncomplicated myocardial infarct, the presence of contractile reserve on predischarge dobutamine stress echocardiography predicts the absence of left ventricular enlargement or even a volume reduction at six months, whereas an ischaemic response identifies patients with a subsequent left ventricular volume increase. Thus by using a relatively simple diagnostic tool such as DSE one can determine the individual risk of left ventricular remodelling. DSE appears to provide clinical information that is relevant in tailoring treatment to reduce the risk of further ischaemia and remodelling in patients with recent myocardial infarction.
REFERENCES
Linked Articles
- Miscellanea