Article Text

Abstract
Background: A recent increase in the absolute number of hospitalisations for acute myocardial infarction (AMI) in New Zealand may signal a new epidemic of coronary heart disease (CHD).
Objective: To quantify the impact of factors other than incidence of disease on these national hospitalisation trends.
Methods: A total of 324 663 electronic records of New Zealand public CHD hospitalisations from 1993 to 2005 were examined. Repeat admissions were identified by record linkage using a unique national health identifier for each patient.
Results: Hospitalisations for AMI increased by about 8% a year throughout the 13-year study period. Interhospital transfers increased by 117% over the study period, while readmissions increased by 42%. By 2005 over 60% of all admissions for CHD were readmissions. After accounting for readmissions, hospital transfers and population changes, the age-standardised first AMI hospitalisation rate peaked in 1995 and has since declined by 15%. Reciprocal trends in AMI and angina hospitalisations were seen, indicating changing diagnostic criteria. Overall hospitalisation rates for first CHD events remained relatively steady at about 216.4 events per 100 000 between 1993 and 2000 and subsequently declined by 25% to 162.2 events per 100 000 in 2005.
Conclusion: Recent trends in hospitalisation rates for AMI are significantly influenced by factors other than underlying changes in CHD incidence. Increasing absolute numbers of admissions coded as AMI in New Zealand between 1993 and 2005 can be accounted for by increases in readmissions, increases in interhospital transfers, changes in diagnostic criteria for AMI and in demography.
Statistics from Altmetric.com
Many developed countries have reported falling death rates from coronary heart disease (CHD) over the past 20–40 years.1–6 However, trends in CHD hospitalisation rates, which are sometimes considered to be a proxy for non-fatal CHD incidence, have not paralleled the mortality trends.7–11 A recent report documented rising numbers of hospitalisation for acute myocardial infarction (AMI) in New Zealand and concluded that this may indicate a new epidemic of CHD.7 However, trends in crude AMI hospitalisation rates should be interpreted with caution because they may be influenced by a number of factors such as hospital transfers, readmissions, demographic changes and changes in diagnostic criteria. In this study, we examined CHD hospitalisation rates from 1993 to 2005 in New Zealand and quantified the impact of each of these factors.
METHODS
Study population
All public hospital CHD admissions, as defined below, between 1993 and 2005 in New Zealand were included in the study.
Data sources
These analyses were based on data from the New Zealand National Minimum Dataset (NMDS) from 1988 to 2005 held by the New Zealand Health Information Service. The NMDS is a national collection of public hospitalisation unit records that contain hospital discharge and clinical information. Specific collection and verification methods of hospitalisation data are documented in the National Minimum Dataset dictionary.12 The National Health Index (NHI) number is a unique identifier that is assigned to each health services user in New Zealand and it allows linkage between different health-related data collections contributing to the numerator of the rates presented.13 An encrypted form of the NHI was used in this study to protect privacy of individual subjects. Private hospital admissions were excluded from the study as unit record data was not available for the whole period. However, they represent <5% of all CHD hospitalisations in New Zealand and three-quarters of these patients are coded as chronic CHD with most being admitted for non-acute procedures.14 Denominator data for calculating rates came from the 5-yearly New Zealand Census sourced from Statistics New Zealand. In the 2006 New Zealand census, New Zealand had a population of 4.18 million.15
Definitions
Total CHD admission episodes were defined as all public hospital admissions (including those resulting in deaths after admission) in New Zealand for coronary heart diseases. We included ICD-9 codes 410–414 before 1 July 1999 and ICD-10 codes I20–22, I24 and I25 subsequently, if they were reported in the primary diagnosis field. AMI cases were patients coded as ICD-9: 410 or ICD-10: I21. Interhospital transfers resulting in artefactual double counting of a single CHD episode were identified by an admission source code.
Readmissions among the total admission episodes were identified retrospectively. An admission was labelled as a readmission if a patient had any previous hospitalisation with diagnostic codes of ICD-9: 410–414 or ICD-10: I20–22, I24 or I25 in the primary or secondary diagnosis fields within the past 5 years. The arbitrary “5-year rule” was to ensure consistency and comparability between years. An analysis of 2005 admissions by one of the authors (CW) showed that the “5-year rule” would identify 87% of all previous CHD admissions since 1998. As a result of the “5-year rule”, this study would slightly overestimate first admissions and underestimate readmissions. First admissions refer to any CHD admission episodes that were not readmissions or artefactually double counted as transfers from one hospital to another. Estimated non-fatal incidence was based on the number of people presenting to hospital for the first time with a primary diagnosis of coronary heart disease; out-of-hospital deaths were excluded.
Calculation of hospitalisation rates
First admission and readmission episodes per calendar year were categorised in 5-year age groups by diagnosis from 0 to 85+ years. Age-adjusted rates were calculated using mid-year population estimates from Statistics New Zealand. Rates were standardised using the World Health Organization (WHO) World population as the standard.16 Standard errors (SEs) and 95% confidence intervals for age standardisation are calculated from the formula based on Poisson distribution assumption:

RESULTS
Trends in total CHD hospitalisation counts
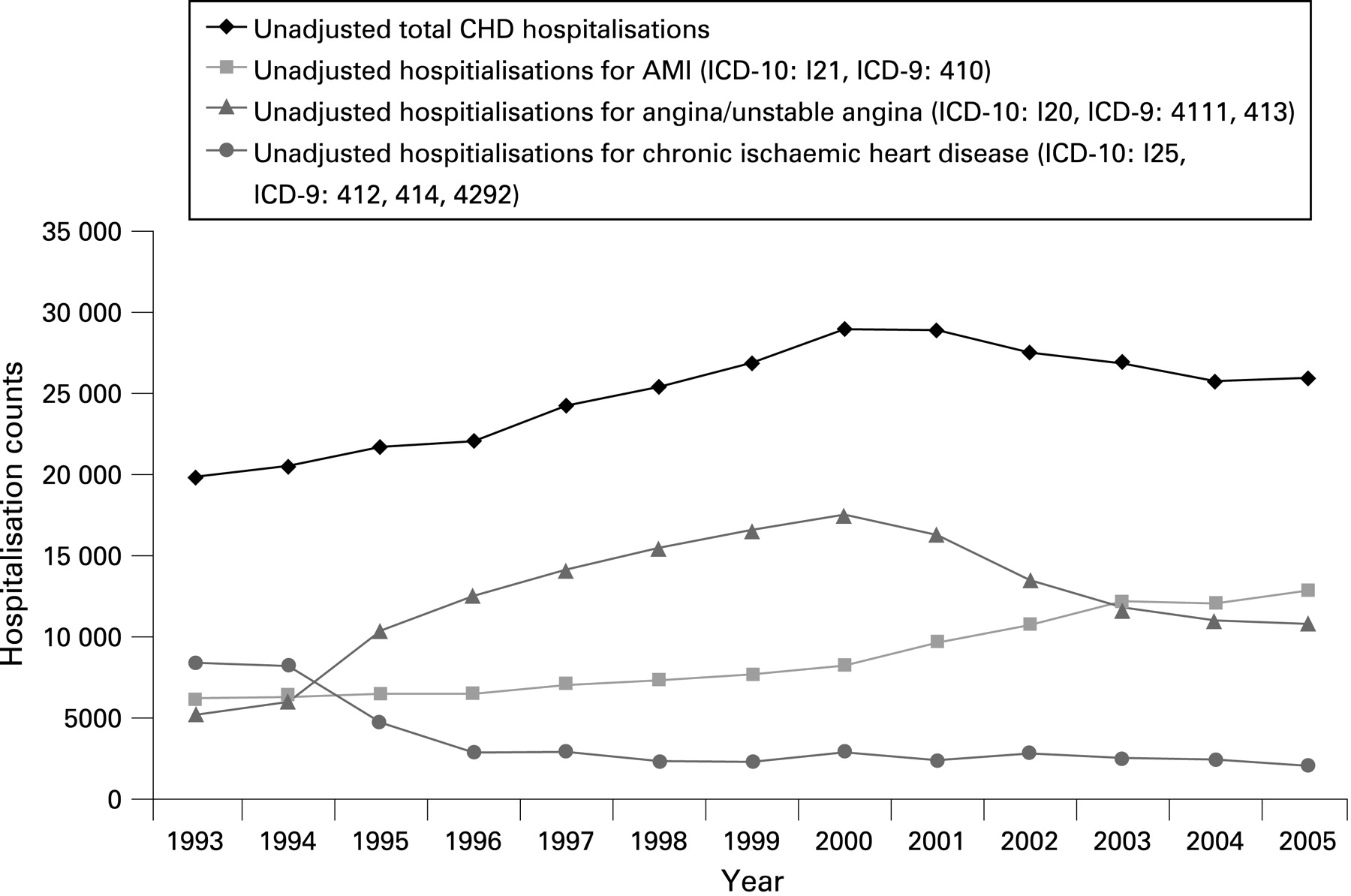
Between 1993 and 2005, there were 324 663 public hospital admissions in New Zealand for CHD (fig 1). There were 19 872 total CHD admissions in 1993, total CHD admissions peaked in 2000 with 28 952 cases and subsequently declined by about 2% a year to 25 963 in 2005.

Trends in hospitalisation counts for diagnostic subcategories of CHD
Between 1993 and 1996, there was a 66% decrease in the numbers of hospitalisations coded as chronic ischaemic heart disease (ICD-9: 412, 414, 4292, ICD-0: I25) from n = 8407 to n = 2881 (fig 1). In the same period, there was a corresponding 141% rise in angina hospitalisations (ICD-9: 4111, 413, ICD-10: I20) from 5205 to 12 526. Chronic ischaemic heart disease hospitalisations were relatively stable after 1996. Hospitalisations for angina peaked in 2000 and subsequently fell by 38% from 17 535 cases in 2000 to 10 801 cases in 2005. There was a reciprocal rise of 56% in AMI (ICD-9: 410, ICD-10: I21) hospitalisations from 8242 to 12 854 cases between 2000 and 2005. Overall AMI hospitalisations increased by 106% (from 6229 to 12 854) over the study period.
Trends in hospital transfers
The number of interhospital transfers for patients with CHD increased by 117% from 1993 (n = 1319) to 2005 (n = 2862) (fig 2). By 2005, double counting of single CHD episodes through hospital transfers accounted for 11% of total CHD hospital admissions. Patients diagnosed with AMI accounted for the majority (74%) of these hospital transfers in 2005.

Trends in first admission and readmission counts
After excluding interhospital transfers, readmissions accounted for the majority of total CHD hospitalisations throughout the study period (fig 2). The proportion of all CHD admissions that were readmissions had increased from 52.6% (n = 9773) to 60.2% (n = 13 908) between 1993 and 2005. Total CHD readmissions peaked in 2000 (n = 16 456) and subsequently fell by 15%. After accounting for hospital transfers and readmissions, the first admissions for CHD also peaked in 2000 with 10 499 cases and had declined on average by 2.5% a year to 9193 in 2005 (fig 2). This fall was mainly attributed to the 31.7% fall in angina/unstable angina from 2000 (n = 5188) to 2005 (n = 3545).
Trends in age-standardised CHD hospitalisation rates
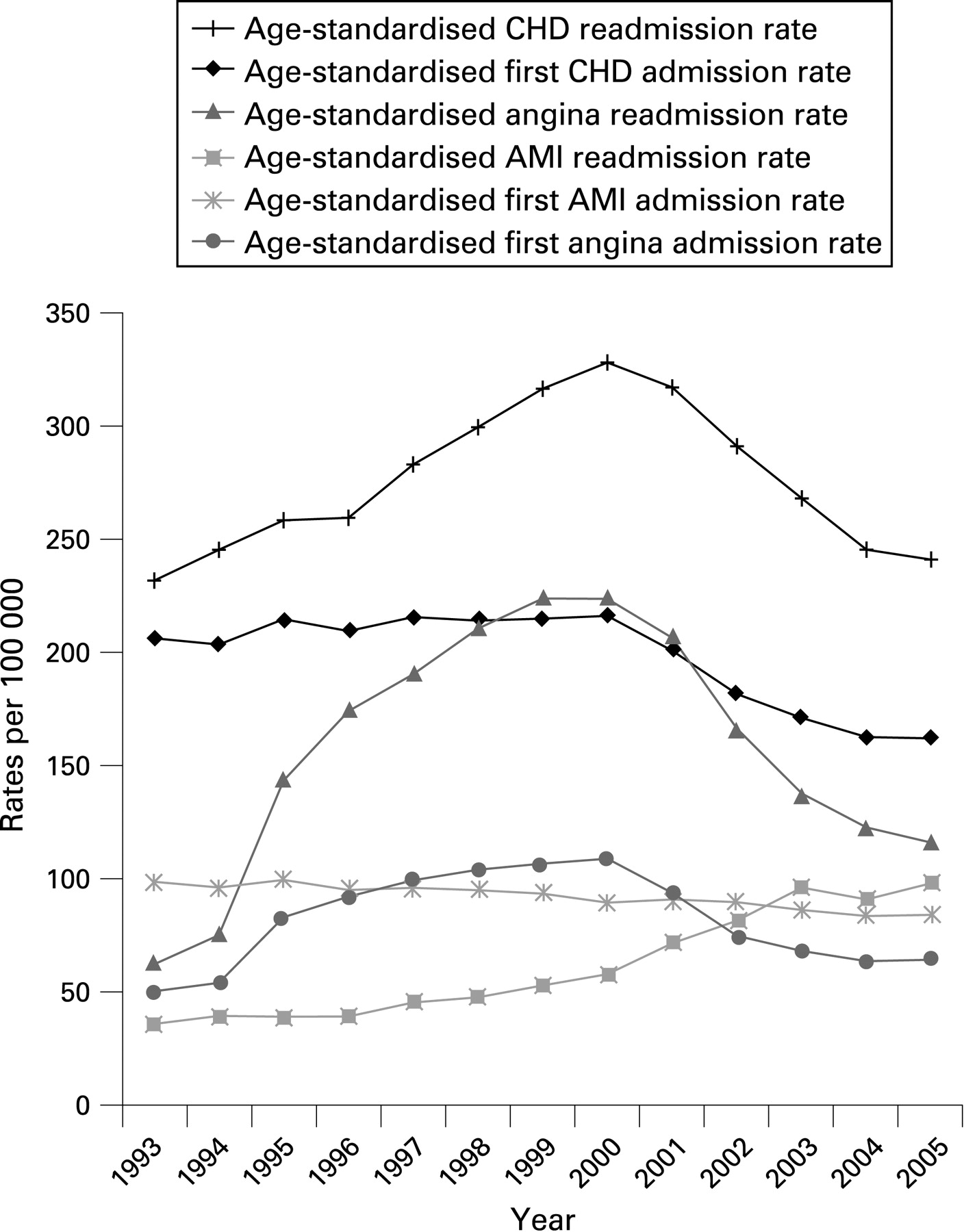
The age-standardised first CHD hospitalisation rate increased by 0.7% a year from 1993 to 2000 (216.4 episodes per 100 000), and since 2000 has declined by an average of 5% a year to 162.2 (95% confidence interval 158.7 to 165.6) episodes per 100 000 in 2005 (fig 3). The age-standardised CHD readmission rate peaked in 2000, with 328.4 episodes per 100 000 and had declined by 26.5% to 241.2 (95% CI 237.0 to 245.4) per 100 000 in 2005. The age-standardised first AMI hospitalisation rate peaked in 1995 with 99.7 episodes per 100 000 and declined steadily by about 15% to 84.2 per 100 000 in 2005 (fig 3). However, there has been a steady increase in the age-standardised AMI readmission rate throughout the study period, rising by 173% from 1993 (n = 36.0 per 100 000) to 2005 (n = 98.2 per 100 000).

{kind=link}
{kind=link}
{kind=link}
Age-standardised rates for first angina admission peaked in 2000 with 109 episodes per 100 000, and had declined by 41% to 64.4 per 100 000 in 2005 (fig 3). The age-standardised rate of readmission with angina after an admission for any form of CHD peaked in 1999 with 224 episodes per 100 000 and had declined by 48% to 116 per 100 000 in 2005.
DISCUSSION
We confirmed a previous report that the total number of AMI hospitalisations has been steadily increasing in New Zealand in recent years.7 The number of AMI admissions more than doubled during the study period (1993–2005). However, this apparently adverse trend can be explained by a number of factors other than an increase in AMI incidence. The rise in total AMI cases was primarily a reflection of the increase in the number of AMI readmissions. The rapid rise in double counting of admissions owing to hospital transfers for AMI cases was also a significant factor, as was the change in diagnostic criteria for AMI. Indeed, after accounting for transfers, readmissions and demographic changes, we demonstrate that the age-standardised first AMI hospitalisation rate has been declining since 1995.
This study examined hospitalisation trends for almost the entire New Zealand population, allowing us to produce age-standardised hospitalisation rates with a high degree of precision. The New Zealand experience, both with the introduction of troponin testing and its subsequent effect on AMI diagnostic criteria, as well as the recent favourable trends in CHD mortality and risk factor prevalence are common to many Western countries,5 17 therefore the findings reported here can probably be generalised to similar populations elsewhere.
While private hospital admissions were excluded, there are few acute admissions to private hospitals in New Zealand. Private hospital admissions accounted for only 4.6% of total CHD hospitalisations in 2002.14 As discussed, all New Zealanders have a unique health identifier—the NHI—enabling the linkage of all admissions for a particular patient and allowing identification of readmissions and hospital transfers. The NHI has been available since 1992.18 The numerator and denominator data analysed here were not NHI-linked and hence the denominators used to calculate hospitalisation rates excluded the small number of non-residents who presented to New Zealand public hospitals but were not counted in the census.
It is unlikely that hospitalisations will capture all non-fatal CHD incidence events occurring in the New Zealand population as some will be either undiagnosed or diagnosed and treated in primary care or in outpatient clinics. The recent establishment of chest pain pathways may have led to more low-risk patients being seen and then sent home from hospital emergency departments rather than being formally admitted. However, patients diagnosed with acute coronary syndrome are seldom treated out of hospital in New Zealand. A population MI register established during the 1980s estimated that <3% of diagnosed MI were treated at home,19 and there is no evidence to suggest this has increased since then.
We were unable to analyse directly the impact of increased availability of new diagnostic and treatment technologies on admission thresholds and the subsequent impact on hospitalisation rates, although our findings undoubtedly reflect this. The introduction and uptake of troponin testing during the period of analysis will have considerably enhanced both sensitivity and specificity of detection of myocardial damage (coded as AMI) and higher risk warranting admission.20 This, along with other diagnostic and triage enhancements, may have influenced CHD admission thresholds in either direction.
The validity of these findings also depends on the validity of the ICD codes. The last published study on New Zealand ICD codes validation was carried out in 1987 and showed that the ICD-9: 410 acute myocardial infarction code had a sensitivity of 86% for identifying definite MI according to World Health Organization (WHO) MONICA study criteria.21 If all CHD codes were used (410–414), sensitivity increased to 95%.
Increasing hospital transfer rates are due to the implementation of agreed national guidelines regarding the desirability of urgent invasive investigation of patients with acute coronary syndromes, especially non-ST elevation myocardial infarction.22 The transfer rate reported from this study is similar to that of a previous study.23 Changes in diagnostic criteria with the introduction of new tests such as troponins have significantly increased the proportion of patients with acute coronary syndromes who are diagnosed as AMI. This is illustrated by the reciprocal increase of AMI counts/readmission rates and corresponding decrease in angina counts/readmission rates from 2000. These findings are consistent with the increases in AMI cases observed in previous studies investigating the impact of the introduction of troponin tests on the number of diagnosed cases of AMI.9–11 The reciprocal fall of hospitalised cases of angina/unstable angina may also be, in part, related to improvement in diagnostic ability, resulting in more patients who are perceived as low risk and subsequently managed as outpatients.24 25 These trends reflect major changes in diagnostic and management practices and illustrate the potential problems of interpreting trends in subcategories of diagnostic groupings.
Although the rapid increase in AMI readmission rates can be primarily explained by the change in diagnostic criteria and improvement in diagnostic modalities, the proportions of overall CHD hospitalisations that are readmissions have also gradually been increasing. The majority (60%) of CHD hospitalisations in New Zealand are now readmissions. This probably reflects a growing prevalent pool of patients with CHD, driven by the marked improvement in case fatality and mortality rates as well as an ageing population.5 26 Therefore, the fall in total CHD admissions since about 2000 is unlikely to have led to a reduced hospital workload, given the greater complexity of disease in prevalent cases.
The observation that 60% of all CHD admissions are readmissions highlights the potential impact of greater targeting of preventive interventions to patients after a first CHD hospitalisation. If the majority of patients hospitalised with CHD undertook cardiac rehabilitation and continued appropriate lifelong treatment and behaviour change, this should lead to a major reduction in readmission rates and therefore total CHD hospitalisations. Many studies have reported that risk factor modification, including uptake of cardiac rehabilitation in patients with prevalent CHD, remains disappointingly poor.27–29
In conclusion, the increasing numbers of AMI hospitalisations in New Zealand do not signal a new epidemic of CHD. The age-standardised first CHD hospitalisation rate, which is the most appropriate routinely available proxy for non-fatal CHD incidence, has been falling in New Zealand since 2000. The presumed fall in incidence has paralleled favourable trends in major cardiovascular risk factors in New Zealand, including smoking, blood pressure and blood cholesterol levels.17 30 Unfortunately, these positive trends are unlikely to lead to a corresponding fall in clinical workload in the short term. The ageing population, the increasing proportion of patients presenting with previous CHD and the increased availability of new diagnostic and treatment options have all placed an increased burden on healthcare services. However, improvements in the provision of cardiac rehabilitation and associated chronic care management for patients who survive a first CHD admission would substantially reduce total hospitalisation rates in the short and medium term.
REFERENCES
Footnotes
Funding: WCC’s masters research was funded by a study grant from New Zealand Population Health charitable Trust.
Competing interests: This article is part of the dissertation for a Master of Public Health undertaken in University of Auckland by WCC. CW is a senior advisor (statistics and epidemiology) working for the Ministry of Health, New Zealand. MT is a public health physician working for the Ministry of Health, New Zealand. SM and RJ have no conflict of interest.
Opinions in the paper are those of the authors and do not necessarily reflect Ministry of Health policy advice.