Article Text

Abstract
Objective: To determine whether cardiac rehabilitation influences plasma levels of angiogenic cytokines and their correlation with myocardial blood flow (MBF).
Design: Randomised controlled study.
Setting: Tertiary cardiac centre.
Patients: 39 postinfarction patients randomised to either a 3-month training group (n = 20) or a non-training group (n = 19), and 19 normal controls.
Interventions: Cardiac rehabilitation.
Main outcome measures: MBF by cardiac magnetic resonance imaging, and plasma levels of stem cell factor (SCF), stromal-derived factor-1 (SDF-1), and vascular endothelial growth factor (VEGF) measured at enrolment and at 3 months after randomisation.
Results: At baseline, when compared with the healthy subjects, postinfarction patients had a lower MBF in the infarcted myocardium during dipyridamole-induced stress (1.65 (0.58) vs 2.77 (0.78) ml/min/g, p<0.001) but higher plasma levels of VEGF (3.65 (0.75) vs 2.77 (0.59) pg/ml, p<0.001 expressed as the natural logarithm) and SDF-1 (2113 (345) vs 1869 (309) pg/ml, p = 0.009). Only SDF-1 was inversely associated with stress MBF in both remote (r = −0.39, p = 0.03) and infarcted myocardium (r = −0.62, p<0.001). After 3 months, the training group’s stress MBF had increased by 33% in the remote (p<0.001) and 28% in infarcted myocardium (p = 0.02), while VEGF decreased by 9% (p = 0.01), and SDF-1 decreased by 11% (p = 0.02). The change in SDF-1 was inversely correlated with the change in stress MBF in both remote (r = −0.40, p = 0.01) and infarcted myocardium (r = −0.50, p = 0.001). In the non-training group, MBF and cytokines were unchanged.
Conclusion: Cardiac rehabilitation improves stress MBF in postinfarction patients, with an inverse decrease in circulating angiogenic cytokines.
Statistics from Altmetric.com
Cardiac rehabilitation reduces coronary event rate and increases exercise capacity1–3 in patients with a prior myocardial infarction (MI). For such patients, a lack of perfusion at the microvascular levels is related to worse prognosis.4 Therefore, improved myocardial perfusion to the heart muscle would be a highly desirable outcome of cardiac rehabilitation. In fact, we have shown that improvements in exercise capacity are accompanied by increased myocardial perfusion reserve after exercise training.5 A deeper question is whether these clinical benefits are associated with angiogenic cytokines.
Angiogenic cytokines such as vascular endothelial growth factor (VEGF), stromal-derived factor-1 (SDF-1) and stem cell factor (SCF) are known to increase the formation of new vessels at ischaemic sites and thus enhance myocardial perfusion. Their levels in peripheral blood increase in response to endothelial damage,6 vascular trauma,7 acute MI8 and heart failure.9 On the other hand, chronic exercise does not raise plasma cytokine levels; rather, there appears to be a trend towards lowering them.10 Collectively, these studies suggest that angiogenic cytokines play a role in the training-induced improvement of myocardial perfusion. A better understanding of the role of surrogate markers of angiogenesis in chronic myocardial infarction and cardiac rehabilitation will provide clues to understanding the bigger issue of selecting patients for training in general. In this study, we investigated whether cardiac rehabilitation influences plasma levels of angiogenic cytokines in postinfarction patients. The secondary aim was to assess the relationship between plasma angiogenic cytokines and myocardial blood flow (MBF), especially in the infarcted myocardium.
METHODS
Study design
This prospective randomised controlled study was approved by the ethics committee of the National Taiwan University Hospital. The detailed study protocol and myocardial perfusion reserve results of the study have been reported previously.5 In brief, male patients ⩽65 years old were eligible if they were admitted within 12 h after the onset of symptoms from a first ST-segment elevation MI, had undergone successful percutaneous coronary intervention with stent implantation of the infarct-related artery with residual stenosis ⩽30% of the vessel diameter, demonstrated a clinically stable course for at least 3 months after discharge, and showed no evidence of myocardial ischaemia on initial and follow-up exercise testing. The exclusion criteria were effort angina, atrial fibrillation, sustained ventricular arrhythmia, New York Heart Association functional class IV symptoms, exercise-limiting diseases, severe pulmonary or renal disease, an implanted pacemaker or claustrophobia.
Eligible patients who provided written informed consent were randomly assigned to the training group, which underwent a 3-month cardiac rehabilitation programme, or the non-training group in which patients continued their usual lifestyle. At baseline and the 3-month follow-up, all patients underwent a functional evaluation that included clinical evaluation, exercise testing, cardiac MRI and measurements of plasma angiogenic cytokines levels. Both groups were receiving stable and optimal pharmacological treatment supervised by their physicians. For comparison of myocardial perfusion and angiogenic cytokines, age-, weight- and height-matched subjects without cardiovascular risk factors were selected as healthy controls. This study complies with the Declaration of Helsinki.
Training protocol
The cardiac rehabilitation programme included health education and exercise training.11 Exercise sessions were performed three times a week for 12 weeks at 55% to 70% of the peak oxygen uptake (Vo2) measured in the initial exercise test and a perceived exertion rating of 12 to 13 (fairly light to somewhat hard) on the Borg scale.12 Each session consisted of a 5 min warm-up period, a 20 min bicycle-ergometer exercise, and a 5 min cool-down period. The exercise session was supervised by a physical therapist, and heart rate and blood pressure were monitored during exercise. Patients in the non-training group received educational support and continued their medications but had no exercise training during the study period.
Exercise testing
Symptom-limited graded exercise testing was conducted with a cycle ergometer (Ergotests; Erich Jaeger, Würzburg, Germany).13 Continuous electrocardiographic monitoring and analysis of expired gases were performed during exercise testing. The workload was 10 W for the first 3 min to make subjects familiar with the exercise equipment and exercise techniques, and thereafter the workload was increased by 10 W every minute. The pedalling cadence was maintained between 50 and 70 rpm. Breath-by-breath analysis of expired gas was performed using an automated system (System 2000, Medical Graphics Corporation, St Paul, Minnesota). The mean value of peak Vo2 was determined from the final 20 s of the test and was expressed in ml/kg/min.
Cardiac MRI
All patients were examined in a 3-Tesla MRI scanner (Trio; Siemens, Erlangen, Germany), and balanced steady-state free precession cine images were acquired in two long-axis and seven to nine short-axis views. After cine imaging was complete, an intravenous bolus dose of 0.025 mmol/kg gadodiamide was administered at a flow rate of 4 ml/s. First-pass perfusion imaging was acquired with contrast injection, using an electrocardiogram-gated non-slice-selective 90° saturation-recovery preparation turbo fast low-angle shot pulse sequence. The acquisition lasted for 80 heart beats, yielding 80 time frames for each level at a temporal resolution of one R-to-R interval. Perfusion studies were performed at rest and during the stress induced by a 4 min infusion of dipyridamole at a concentration of 0.14 mg/kg of body weight per minute. After the perfusion studies, patients received a third dose (0.15 mmol/kg) of contrast agent (cumulative dose of 0.20 mmol/kg). Ten minutes later, the late gadolinium enhancement images were acquired with the use of an inversion-recovery prepared, segmented turbo fast low-angle shot pulse sequence.
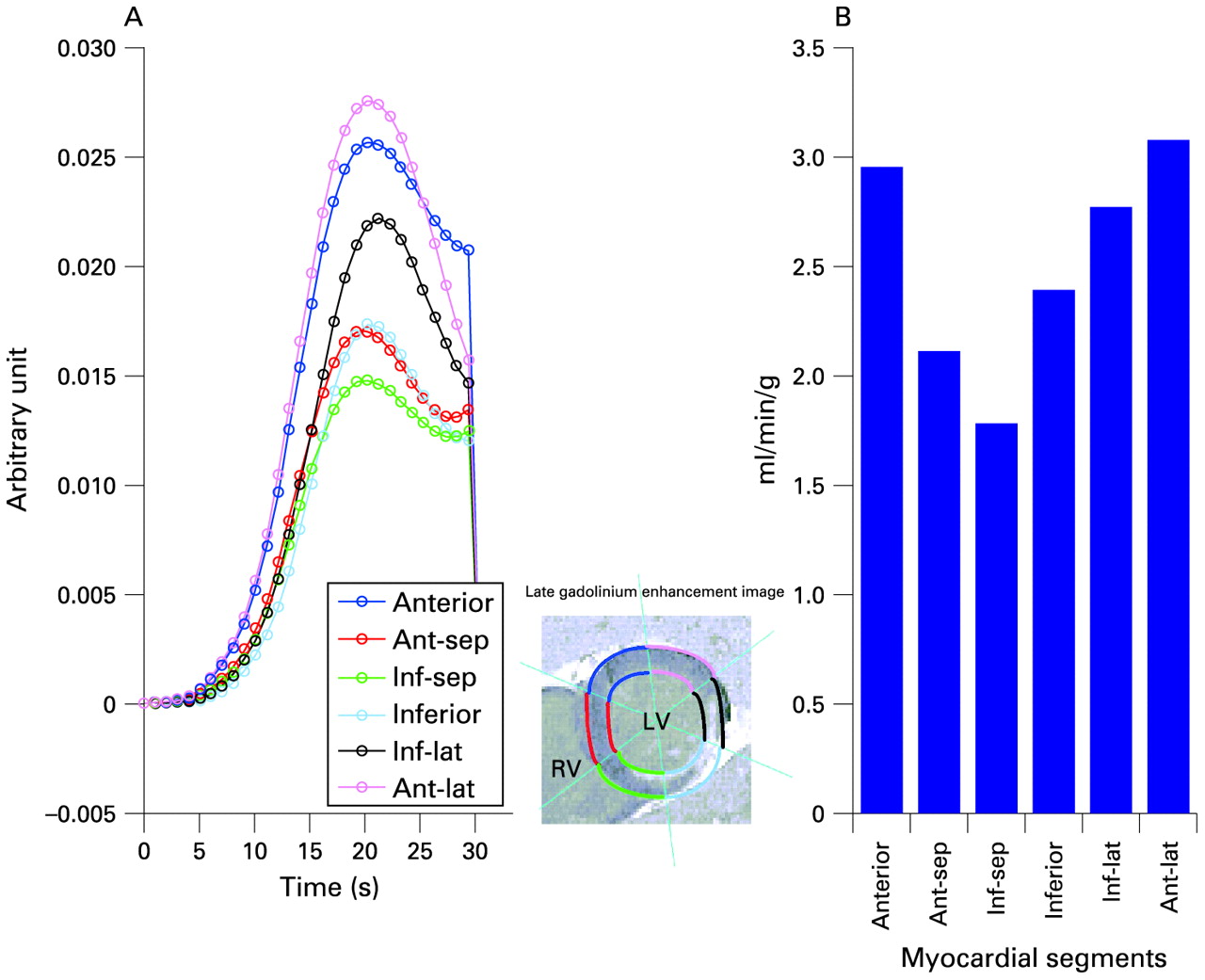
To determine absolute MBF values at rest and stress status, we adopted a model-independent deconvolution method proposed by Jerosch-Herold et al, a method that was previously validated in experimental animal studies by comparison with blood-flow measurements with radiolabelled microspheres.14 Perfusion analysis started with alignment of the first-pass contrast-enhanced images followed by surface coil signal correction and myocardial segmentation. The left-ventricular (LV) myocardium at three short-axis levels was divided into 16 equiangular segments according to the American Heart Association’s standardised myocardial segmentation, with each segment being assigned to a coronary artery territory, excluding the apical cap.15 In each segment (fig 1), MBF was determined in units of ml/min/g by a deconvolving signal-time curve and was computed segment by segment. These segments were further defined as infarcted myocardium if the supplying coronary artery was an infarct-related artery; otherwise, they were defined as remote myocardium. To assess infarct size, we detected late gadolinium enhancement and quantified it using a signal intensity threshold greater than two standard deviations above the mean signal intensity in the remote myocardium.16 Infarct size was expressed as grams of infarcted myocardium or as a percentage of LV mass. Results of perfusion studies and late enhancement were analysed using the Mathematica software package (Wolfram Research, Champaign, Illinois). The intraobserver variability in the perfusion results was 6% and 3% in the LV volume results.17

Measurements of myocardial blood flow (MBF) in a patient with an old inferior wall myocardial infarction (shown in the late gadolinium enhancement image). After image registration, surface-coil intensity correction and segmentation, we obtained the signal-time curve of the segments in the LV myocardium by the model-independent deconvolution method, which represents the measured response (A). Then, MBF was readily determined by the initial height of the response (B). Ant, anterior; Inf, inferior; Lat, lateral; RV, right ventricle; Sep, septal.
Measurements of angiogenic cytokines
To rule out any effect of short-term exercise on cytokines levels,18 blood samples were always taken after at least 72 h of physical inactivity and overnight fasting when the subject had rested in the sitting position for at least 10 min. The plasma samples were immediately frozen and stored at −70°C. High-sensitivity enzyme-linked immunosorbent assay kits (Bender MedSystems, R&D) were used to measure plasma levels of SCF, SDF-1 and VEGF according to the manufacturer’s protocols. SDF-1 levels were assayed in platelet-depleted plasma samples (centrifuged at 11 000 g for 10 min at 4°C). Each assay was replicated twice, and a mean value was reported. In 19 age- and sex-matched healthy volunteers, there were no significant interval differences in angiogenic cytokines over a 3-month period. The values at baseline and at the 3-month follow-up for SCF levels were 524 (193) pg/ml and 506 (194) pg/ml, for SDF-1 levels were 1869 (309) pg/ml and 1812 (306) pg/ml and for the log-transformed values of VEGF levels 2.77 (0.59) pg/ml and 2.66 (0.49) pg/ml, respectively. Intra-assay and interassay variabilities were <5%.
Statistical analysis
Primary endpoint was the change from baseline in stress MBF in the infarcted myocardium at 3 months’ follow-up. We calculated that we would need 18 patients in each group to achieve a power of at least 80% to detect a 20% difference in MBF change between study groups, with a two-sided significance level of p<0.05, and a 20% increase for the stress MBF change from baseline to 3 months’ follow-up. All data are presented as the mean (SD) for continuous data and as proportions for binary data. If the data were not distributed normally, natural logarithmic transformation would be used for analysis. Baseline characteristics were compared using an unpaired Student t test for continuous data and χ2 analysis for binary data. We used analyses of covariance to compare MBF changes in the two study groups with training treatment as the main factor and MBF at baseline as a covariate. To estimate the training effect, differences in least-squares means and corresponding 95% CI were calculated based on the model of analyses of covariance. The consistency of the training effect on MBF change was assessed across preliminary defined subgroups of angiogenic cytokines. Median values of the patient population were used to create subgroups of equal size. The correlations between angiogenic cytokines and clinical and MRI measures were assessed with the Pearson correlation coefficient. All statistical tests were two-sided with a significance level of p<0.05. Statistical analyses were performed using the software package SPSS version 12.02 (SPSS, Chicago).
RESULTS
Clinical characteristics
Between August 2004 and December 2005, 91 patients were informed about the trial. Thirty-seven refused to participate, and 15 did not meet the inclusion criteria. The remaining 39 patients were enrolled in the study and randomised to either the training group (n = 20) or the non-training group (n = 19). Nineteen subjects without cardiovascular risk factors that were matched by age, weight and height were selected as healthy controls. Table 1 shows the comparison of demographic data between the 39 post-MI patients and 19 healthy subjects. Compared with the healthy subjects (table 1), peak Vo2 and stress MBF in the infarcted myocardium were lower (both p<0.01), while plasma levels of SDF-1 and VEGF were higher in the post-MI patients (both p<0.01). However, there were no significant differences between the patients’ data and the healthy subjects’ reference values with respect to resting MBF in the infarcted myocardium, resting or stress MBF in the remote myocardium, and plasma SCF level.
The mean time from the onset of MI to initial evaluation was 8.3 (3.4) months (table 1). In about 60% of MI patients, the infarct-related artery was the left anterior descending artery. No significant differences between the training and non-training groups were observed in terms of age, cardiac structures and functions, infarct size, duration after MI or risk factors. The groups did not differ in medication taken. All patients maintained their own drug plan throughout the study. No patients died, were hospitalised for coronary intervention or had worsening symptoms during the 3-month study period.
Effects of cardiac rehabilitation on myocardial blood flow
Compared with the non-training group (table 2), patients in the training group had increased stress MBF in the remote myocardium (+33%, p<0.001) and infarcted myocardium (+28%, p = 0.02) at 3 months. The effects of cardiac rehabilitation on the change in stress MBF in the infarcted myocardium at the 3-month follow-up were consistent among all investigated subgroups (fig 2). Besides, patients with higher cytokine levels before training showed a greater MBF improvement. In contrast, resting MBF was not affected by cardiac rehabilitation. No significant differences in MBF between baseline and follow-up levels were seen in the non-training group.

Subgroup analyses of changes in stress myocardial blood flow (MBF) in the infarcted myocardium from baseline at 3-month follow-up. *Median values of the patient population were used to create subgroups of equal size. Oval dots show differences in least-squares means between groups; horizontal bars show the 95% confidence interval. SDF, stromal-derived factor-1; VEGF, vascular endothelial growth factor.
Effects of cardiac rehabilitation on angiogenic cytokines
Compared with the non-training group, patients in the training group had decreased VEGF (−9%, p = 0.01) and SDF-1 (−11%, p = 0.02) at 3 months (table 2). In contrast, the plasma SCF level was not significantly affected by cardiac rehabilitation. No significant differences in plasma angiogenic cytokines between baseline and follow-up levels were seen in the non-training group.
Clinical and cardiac MRI measures and angiogenic cytokines
At baseline, significant associations were found among SDF-1, exercise capacity and MBF (table 3). Plasma SDF-1 was significantly inversely associated with peak Vo2 (r = −0.45, p<0.01), resting MBF in the infarcted myocardium (r = −0.32, p = 0.04) and stress MBF in the remote (r = −0.39, p = 0.03) and infarcted myocardium (r = −0.62, p<0.001). A positive correlation was also found between SDF-1 and VEGF levels (r = 0.33, p = 0.02). In contrast, neither VEGF nor SCF was found to be associated with exercise capacity or MBF. Plasma levels of angiogenic cytokines were not associated with age, body surface area, cardiac contractility and infarct size.
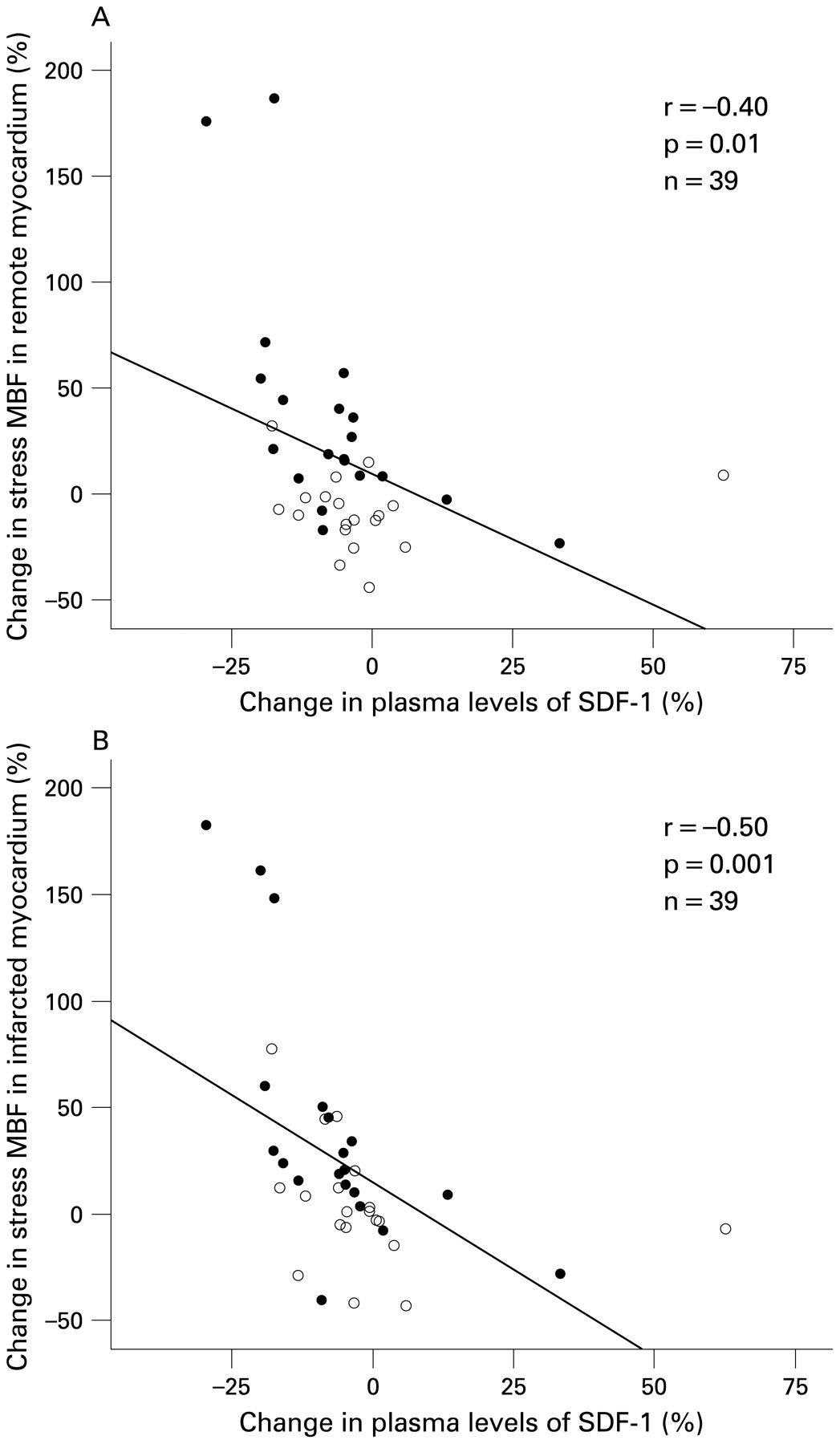
After 3 months, the percentage change in plasma levels of SDF-1 was inversely correlated not only with the change in peak VO2 (r = −0.38, p = 0.02) but also with the change in stress MBF in the remote myocardium (r = −0.40, p = 0.01; fig 3) and infarcted myocardium (r = −0.50, p = 0.001; fig 3). The percentage change in VEGF levels was inversely correlated with the change in peak Vo2 (r = −0.40, p<0.01). However, there was no association between the percentage change in VEGF and the change in MBF, at rest or at stress, in the remote or infarcted myocardium. There was no association between the percentage change in SCF and the change in MBF or exercise capacity.

{kind=link}
{kind=link}
{kind=link}
Relation between the percentage change in the plasma levels of stromal-derived factor-1 (SDF-1) and the percentage change in the stress myocardial blood flow (MBF) in the remote myocardium (upper panel) or infarcted myocardium (lower panel). Patients in the training group are represented by a closed circle, and those in the non-training group an open circle.
DISCUSSION
The present study investigates the effect of cardiac rehabilitation on angiogenic cytokines and their relationships with absolute MBF in the postinfarction patients, where there are three main findings. First, we report that in the late postinfarction period, higher plasma levels of angiogenic cytokines exist with a lower value of stress MBF in infarcted myocardium. Among the angiogenic cytokines measured in this study, only SDF-1 was significantly inversely associated with stress MBF, especially in the infarcted myocardium. Second, we show that cardiac rehabilitation reduces the cytokines levels and concordantly improves stress MBF in the whole myocardium. Finally, we demonstrate that a reduction in plasma SDF-1 is associated with an increase in stress MBF, especially in the infarcted myocardium. Thus, for the first time, this study has identified SDF-1 as a molecular marker that may reflect stress MBF and may be used to predict the outcome after cardiac rehabilitation.
To the best of our knowledge, the present study is the first study to concurrently examine the relationship between angiogenic cytokines and myocardial perfusion serially with a validated quantitative MRI technique over the course of cardiac rehabilitation. In our previous report,5 an increase in stress perfusion index in the infarcted myocardium after cardiac rehabilitation was considered to be the result of the functional recovery of resistant vessels because other major contributors for myocardial hypoperfusion, such as wall stress and infarct size, were not affected by cardiac rehabilitation. In animal studies, long-term exercise training sensitises resistance arteries for the vasodilatory effects of adenosine19 and increases the total vascular bed cross-sectional area in heart.20 Sequentially, vascular resistance decreases and maximal MBF rises under adenosine- or dipyridamole-induced stress. However, the mechanisms that mediate the increase of coronary vascularity after cardiac rehabilitation are under investigation. Among the possible directions of research, an angiogenic cytokine, such as SDF-1 or VEGF, can regulate several crucial aspects of adult vasculogenesis and blood-vessel development and, as such, qualifies as one of the major research targets.
In the present study, postinfarction patients had higher levels of plasma VEGF and SDF-1 than healthy subjects. Both VEGF and SDF-1 are known to play a significant role in the atherosclerosis. These two cytokines are highly expressed in smooth muscle cells, endothelial cells and macrophages in human atherosclerotic plaques,21 22 and their plasma levels are higher in patients with stable coronary artery disease, suggesting that they might be a biomarker for the plaque growth and progression. Besides, they are involved in the process of angiogenesis and mediate neovascularisation.23 24 Myocardial ischaemia is known to stimulate an elevation in myocardial and plasma levels of VEGF and SDF-1.25 26 In the present study, we showed an inverse relationship between SDF-1 levels and MBF in post-MI patients, suggesting that a high plasma level of SDF-1 might be a marker of myocardial hypoperfusion. Beyond being atherosclerotic contributors and angiogenic cytokines, both SDF-1 and VEGF are chemokines that are involved in the recruitment of stem cells or endothelial progenitor cells to the injured organ. In fact, upregulation of SDF-1 in the injured myocardium, and consequently in the circulation, is a prerequisite first step in initiating mobilisation and recruitment of stem cells to the injured heart.27 Taken together, it is tempting to speculate that higher plasma levels of angiogenic cytokines after MI may represent a plaque burden in pre-existing coronary artery disease or may signal an ischaemic myocardium, which increases demand for stem-cell mobilisation to the heart for neovascularisation or repair.
Another cytokine, SCF, is known to interact synergistically with VEGF to mobilize stem cells and improve chronic myocardial ischaemia in an animal study.28 Although no relation with MBF was observed in this study, post-MI patients tended to have higher plasma SCF levels. Since we used the plasma of venous samples to measure the concentration of cytokines, and since this type of plasma is subject to the influence of washout dilution from ischaemic tissue to systemic circulation, the relationship might not necessarily be demonstrated.
Acute bouts of exercise or ischaemic exercise training may raise plasma levels of angiogenic cytokines.29 However, in the resting steady-state condition, there appears to be a trend towards lower circulating angiogenic cytokine levels after subischaemic exercise training,10 a finding confirmed in the present trial. The present study shows that cardiac rehabilitation decreases plasma levels of VEGF and SDF-1, and that the extent of their diminution is related to the increase in stress MBF and exercise capacity. Following the discussion above, the influence of cardiac rehabilitation on the angiogenic cytokines could be attributed to improved myocardial perfusion by the regression of coronary atherosclerosis or the augmentation of vascular bed. Few data address whether exercise slows progression of atherosclerotic plaque. A 6-year randomised, controlled trial demonstrates that regular physical exercise at low to moderate intensity can attenuate progression of carotid atherosclerosis in men, but the effect is not seen until the 3-year exercise.30 Thus, the former viewpoint is less likely to be true in this 3-month rehabilitation programme. The latter viewpoint is supported by several recent reports that short-term exercise training induced mobilisation of endothelial progenitor cells from bone marrow to peripheral blood31 and thereby may improve endothelial regeneration and collateral formation into ischaemic myocardium.32 The present study demonstrates that a reduction in plasma SDF-1 in the training group correlates with an increase in stress MBF, suggesting a feedback regulation of SDF-1 due to increased blood supply to the myocardium after cardiac rehabilitation. Thus, a serial assay of plasma SDF-1 levels appears to be a valuable method to evaluate the clinical outcome of cardiac rehabilitation.
Study limitations
Several study limitations should be considered when interpreting these findings. First, in view of the small size of our trial, our findings must be considered with caution. Even though this was a prospective randomised controlled study, our results need to be confirmed in a larger cohort. With this limitation in mind, it is noteworthy that the patient number in each group was larger than the predetermined sample size by power analysis. Second, these results are applicable only for male patients ⩽65 years old with ST-segment elevation MI after successful percutaneous coronary intervention. Further studies should also be performed on female patients. Third, the source of the measured plasma concentration of angiogenic cytokines cannot be elucidated. SDF-1 is produced in almost all organs, but most abundantly in the bone marrow and ischaemic organs. Although we demonstrate a moderate association between plasma SDF-1 and myocardial perfusion in the post-MI patients, fig 3 demonstrates that the relationship does not appear to be linear. In this type of analysis where the number of data points is relatively small, and the relationship is not actually linear, the slope of the regression line can be heavily influenced by only a couple of data points. This observation further highlights the weak correlation between these variables. Further studies using blood samples from coronary sinuses and in a larger cohort may ascertain this relationship more firmly.
Conclusion
This study suggests that postinfarction patients with elevated SDF-1 levels are more likely to have clinical benefits after cardiac rehabilitation, but the study was too small to allow meaningful subgroup analyses. A large prospective study is needed to determine whether including serial measurements of SDF-1 during follow-up improves the ability to detect myocardial hypoperfusion and thereby allows early cardiac rehabilitation.
Acknowledgments
We are grateful to C-L Cheng, for assistance with patient enrollment and follow-up, S-F Hsiao, for assistance with the cardiac rehabilitation programme and C-H Chen, for assistance with biochemistry analysis.
REFERENCES
Footnotes
Funding: The study was supported by Grant 95-2745-B-002-005 from National Science Council, Taiwan.
Competing interests: None.
Ethics approval: Ethics approval was provided by the National Taiwan University Hospital, Taipei, Taiwan.
Patient consent: Obtained.