Article Text

Abstract
Atrial tachyarrhythmias are a common complication of atrial septal defects. The objective was to determine the effect of atrial septal defect closure on pre-existing atrial tachyarrhythmias and to investigate if such an effect is present after either surgical or percutaneous closure. Medline, EMBASE, Cochrane Library, and Google Scholar databases were searched between 1967 and 2009. The search was expanded using the ‘related articles’ function and reference lists of key studies. All studies reporting pre- and post- closure incidence (or prevalence) of atrial tachyarrhythmias in the same patient groups were included. Data were independently extracted by two authors according to a pre-defined protocol. Incongruities were settled by consensus decision. Twenty six studies were identified including 1841 patients who underwent surgical closure and 945 who underwent percutaneous closure. Meta-analysis using a random effects model demonstrated a reduction in the prevalence of atrial tachyarrhythmias following atrial septal defect closure [OR = 0.66 (95% CI 0.57-0.77)]. This effect was demonstrated after both percutaneous [OR = 0.49 (95% CI 0.32-0.76)] and surgical closure [OR = 0.72 (95% CI 0.60-0.87)]. Immediate (<30 days) and mid-term (30 days - 5 years) follow-up also demonstrated a reduction in AT prevalence [ORs of 0.80 (95% CI 0.66-0.97) and 0.47 (95% CI 0.36-0.62) respectively]. Atrial septal defect closure, whether surgical or percutaneous, is associated with a reduction in the post-closure prevalence of pre-existing atrial tachyarrhythmias and atrial fibrillation in the short to medium term.
- Atrial septal defect
- surgical repair
- transcatheter closure
- atrial tachyarrhythmia
- atrial arrhythmias
- atrial fibrillation
Statistics from Altmetric.com
- Atrial septal defect
- surgical repair
- transcatheter closure
- atrial tachyarrhythmia
- atrial arrhythmias
- atrial fibrillation
Introduction
Atrial septal defects (ASDs) are one of the most common congenital cardiac abnormalities in adulthood associated with arrhythmias, right heart failure, stroke and premature death.1 While large ASDs may present in childhood with signs of heart failure, a significant proportion of patients present in the 3rd–4th decade of life.2 Often asymptomatic until the onset of complications, the main cause of morbidity and mortality in ASD patients is attributed to the development of atrial tachyarrhythmia (AT).1 3 4 Approximately 10% of untreated patients with ASD develop supraventricular arrhythmias, especially atrial fibrillation (AFIB) by the age of 40 years,3 5 and the incidence continues to increase with age (reported incidence for older patients is 20–50%).6–8
Initially, all ASDs were closed surgically but percutaneous techniques first described in 1974 by King and Mills9 have become established alternatives. According to the National Institute of Clinical Excellence and the Joint American Heart Association/American College of Cardiology guidelines, percutaneous techniques are now considered ‘acceptable treatment’ (for ostium secundum ASD).10 Sinus venosus, coronary sinus, or ostium primum ASD, however, are unsuitable for percutaneous closure and thus need to be closed surgically.11 Previous studies have examined the impact of ASD closure on AT,12 suggesting that closure may initiate or discontinue AT,6 but comprehensive analysis has not been performed to quantitatively review the available evidence. To date, there is no randomised trial comparing surgical and percutaneous closure and now that percutaneous management has become widely established, this is unlikely to occur.
Consequently the specific aims of this study were: (a) to determine the potential antiarrhythmic effect of ASD closure on pre-existing AT; (b) to determine whether evidence for an antiarrhythmic effect is seen following both surgical and percutaneous ASD closure; and (c) to determine whether any antiarrhythmic effect is time dependent.
Methods
Literature search
A multilayer literature search was performed using Medline, EMBASE, Cochrane Library and Google Scholar databases for all relevant studies until 2009 using the following MeSH search headings: ((Atrial Septal Defect (ASD) or ASD closure or ASD Repair) and (Cardiac Surgery or Cardiothoracic surgery or Trans-catheterisation) and (Rhythm or Atrial (Tachy) Arrhythmia or Atrial Fibrillation (AFIB) or Flutter)). The search was expanded using the ‘related articles’ function and by considering reference lists of the key studies. Abstracts from the American Heart Association were also searched. All the review articles whose subject was ASD closure, as well as their reference lists were also screened (figure 1).

Search strategy and selection of studies (PRISMA statement compliant).
Outcomes
The primary outcome measure is change in the prevalence of AT following ASD closure. In this analysis, papers were included which referred to ‘atrial tachyarrhythmia’, ‘atrial fibrillation’, ‘atrial flutter’, ‘atrial tachycardia’, ‘left atrial tachycardia’, ‘atrio-ventricular nodal re-entry tachycardia’, ‘junctional tachycardia’, ‘Wolff-Parkinson-White’ and ‘supraventricular tachycardia’. Secondary analysis of studies which referred only to ‘atrial fibrillation’ was also performed.
Inclusion and exclusion criteria
We included all studies reporting the incidence (or prevalence) of AT before and after ASD closure (only patients with pre-existing AT within studies were included). All studies reporting an adult population in which the mean/median age was at least 18 years prior to intervention were included. Studies of both surgical and percutaneous closure including all ASD types (sinus venosus, ostium primum and ostium secundum) were included. Studies describing patent foramen ovale closure, those not written in English and those failing to differentiate between new-onset AT and a diminution in the prevalence of pre-closure AT were excluded.
Data extraction
Two reviewers (SS and JV) independently extracted data according to a predefined search protocol. This included study design, type of ASD and AT, number of patients, age of patients, and closure type. The prevalence of AT and AFIB was recorded pre-closure, post-closure and at latest follow-up. In the case of discrepancy, consensus decision was achieved by discussion, and where necessary adjudication by a third reviewer (TA) (tables 1 and 2).
Studies comparing the prevalence of atrial tachyarrhythmia/fibrillation between pre-closure and post-closure groups in a generalised population
Prevalence of atrial tachyarrhythmia (AT) during follow-up period
Quality scoring
Qualitative data to assess study comparability and enable quality scoring were also extracted. These data were split into two sections: variables previously highlighted to predispose surgical patients to AFIB (age, gender, hypertension, diabetes, ejection fraction, chronic obstructive pulmonary disease, left main stem disease and three vessel coronary artery disease); and variables known to positively affect the incidence of post-closure AT in patients with AT (right atrial dilatation, right ventricular dilatation and pulmonary hypertension).15 36 Table 3 summarises the distribution of these risk factors. The individual inclusion and exclusion criteria utilised by the studies analysed are shown in the Appendix.
Distribution of risk factors for atrial tachyarrhythmia within patient groups
Statistical analysis
Meta-analysis was conducted according to PRISMA, MOOSE and Cochrane Collaboration guidelines.37–39 The OR was used as the summary statistic. An OR <1 suggested that the prevalence of AT was lower following ASD closure. The OR was considered statistically significant at the p<0.05 level if the 95% CI did not include the value 1.
Aggregation of the overall rates of the primary and secondary outcomes was performed with the Mantel–Haenszel method.40 We used a random-effects model which assumes that there is variation between studies as this model better accounts for heterogeneity between studies.41 42 Analysis was conducted using Review Manager V.5.2 (The Cochrane Collaboration, Software Update, Oxford, UK).
Assessment of data validity and heterogeneity
Several quantitative and graphical methods were used to assess, explain and account for important determinants of meta-analytical validity—heterogeneity and bias.
Bias exploration: publication bias and risk of bias analysis
Publication bias was assessed graphically with funnel plots to assess for asymmetry and evidence of outliers. The assessment of risk of bias was conducted in line with recommendations from the Cochrane guidelines.37 We performed a ‘domain-based evaluation’ in which critical assessments were made separately for different domains where each domain type assessed a specific bias type. Adequate sequence generation, allocation concealment and blinding were not considered as we were not directly comparing two interventions, and we only considered the effect of selective reporting, incomplete outcome data and other sources of bias.
Sensitivity analysis through examination of subgroups
Sensitivity analysis was performed through examination of a number of subgroups—surgical ASD closure, percutaneous ASD closure, post-closure AFIB prevalence, post-closure AT prevalence—during follow-up (immediate (<30 days), mid-term (30 days–5 years), late (>5 years)) and study quality. To quantify the study quality, we devised a scoring system. We attributed a point to each study when compliant with 10 specified factors (table 3). This generated a median of 2. The range was then divided into thirds which were scored from 1 to 3. Ten studies qualified for the ‘top’ third (4–5 matched factors) and these studies were analysed separately.
Heterogeneity assessment through the I2 statistic
Heterogeneity of treatment effects between studies was assessed using the I2 statistic. This represents the proportion of total variation observed between the trials attributable to differences between trials rather than sampling error or chance. The degree of heterogeneity was graded as low (I2<25%), moderate (I2=25–75%) or high (I2>75%).43
Results
Selected studies
Literature search identified 575 manuscripts. On screening the abstracts 480 were excluded. A further 69 were excluded after full text review. This resulted in a final study group of 26 studies published between 1967 and 2009 being selected for the meta-analysis. In total 2786 patients were included from 3 prospective observational and 23 retrospective studies (figure 1).2 4 7 13–35 Table 1 shows characteristics of individual studies included.
Meta-analysis
Four of the 26 studies showed a statistically significant reduction in the prevalence of AT following ASD closure.7 15 17 23 Meta-analysis of all 26 studies showed a significant reduction in the prevalence of AT (figure 2A), with an OR of 0.66 (95% CI 0.57 to 0.77) and an I2 of 0% indicating non-significant heterogeneity. Seventeen of 26 studies reported the prevalence of AFIB as a subset of overall AT prevalence.2 13 16 19–23 25 26 28–32 34 35 The calculated OR for AFIB was 0.77 (95% CI 0.63 to 0.95), with an I2 of 0% throughout (figure 3).

Meta-analysis of studies comparing prevalence of atrial tachycardia pre- and post-closure. (A) All studies. (B) Percutaneous closure studies only. (C) Surgical closure studies only.

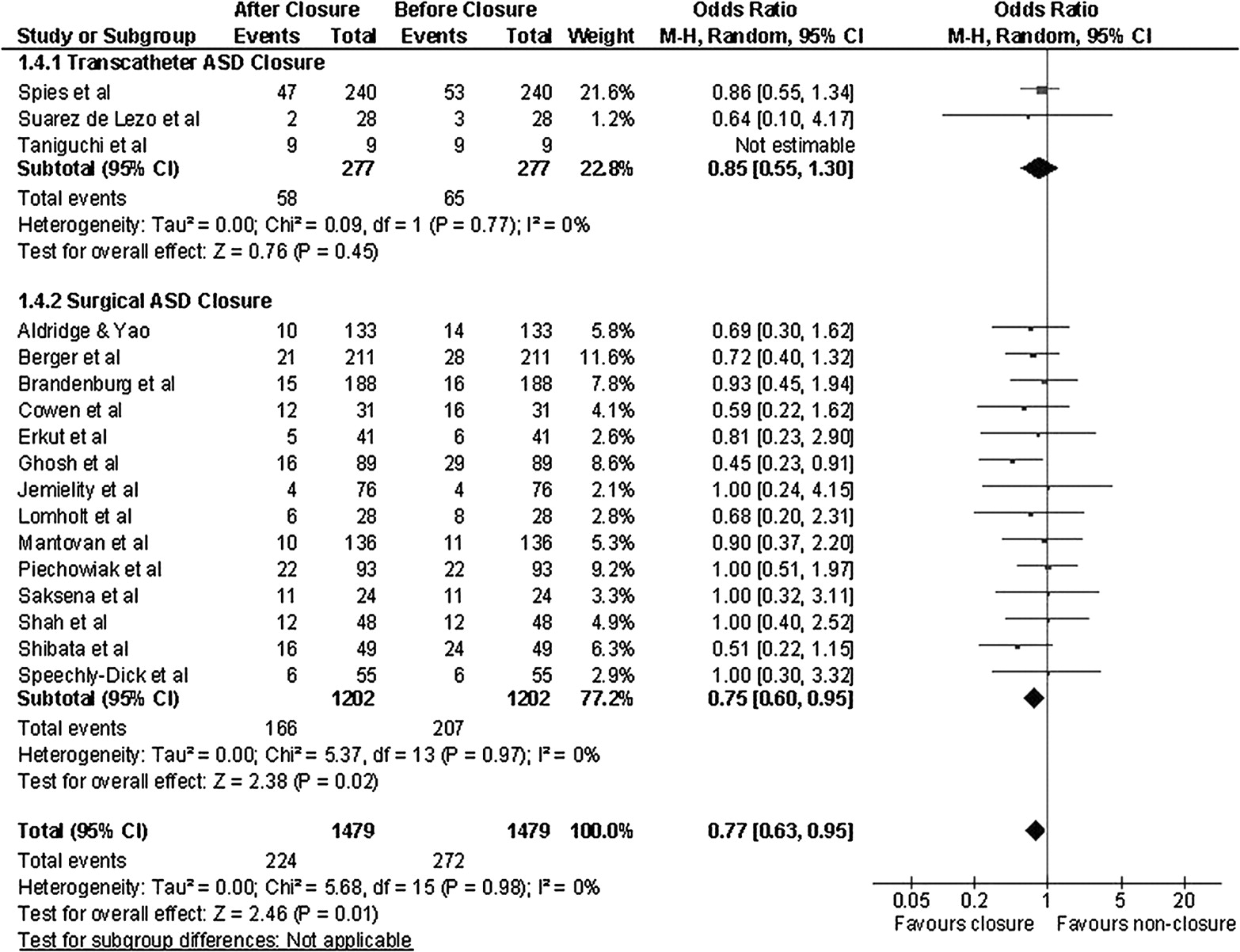
Meta-analysis of studies comparing prevalence of atrial fibrillation pre- and post-closure.
Sensitivity analysis
Effect of closure method
Seven studies reported percutaneous ASD closure.13–19 An OR of 0.49 (95% CI 0.32 to 0.76) was calculated, with a moderate heterogeneity I2 of 45% (figure 2B). Similarly when analysis of the 19 studies reporting surgical ASD closure was performed, the calculated OR was 0.72 (95% CI 0.60 to 0.87), with a non-significant I2 heterogeneity of 0% (figure 2C).2 4 20–35 44 The results were similar in the surgical group when only AFIB was considered with an OR of 0.75 (95% CI 0.60 to 0.95). However, in the percutaneous closure group, while the OR was similar (OR 0.85), this did not reach statistical significance (95% CI 0.55 to 1.30).
Duration of effect
Fifteen studies2 7 14 16 18–21 26 29–31 33–35 reported AT prevalence immediately after the procedure (<30 days), with an OR for ASD closure of 0.80 (95% CI 0.66 to 0.97). Eleven studies7 13–20 23 29 30 32 reported AT prevalence at mid-term follow-up (30 days–5 years), with an OR of 0.47 (95% CI 0.36 to 0.62). Eleven studies4 21 22 25–28 31 33 34 reported the results of long-term follow-up (>5 years). In these, the effect of ASD closure on AT prevalence was not significant (OR 0.84, 95% CI 0.65 to 1.07).
Study quality
Table 3 shows the number of risk factors for post-closure AT that are matched in each study. This table also shows the ‘quality score’ assigned, based on the number of factors matched. Ten studies matched ≥4 factors scoring 3 points for quality.13 16 17 20 21 23 25 27 34 35 In this group the OR for prevalence of post-closure AT was 0.70 (95% 0.51 to 0.97).
Publication bias and risk of bias
Publication bias was explored with a funnel plot (figure 4A) which shows mild asymmetry with one outlier.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Publication bias and risk of bias assessments. (A) Funnel plot test exploring publication bias. (B) Methodological quality graph: review authors' judgements about each methodological quality item presented as percentages across all included studies. (C) Methodological quality summary: review authors' judgements about each methodological quality item for each included study.
Risk of bias was presented as methodological quality graphs. Figure 4B represents the risk of bias in which each methodological quality domain is presented as a percentage across all included studies. Figure 4C is a methodological quality summary depicting the scoring for each domain across all the included studies, demonstrating mixed potential risk of bias.
Discussion
This study shows that ASD closure, whether surgical or percutaneous, reduces the post-closure prevalence of pre-existing AT in the short to mid term (OR 0.66, 95% CI 0.57 to 0.77). A similar effect is also seen in the surgical but not the percutaneous group, when only AFIB was considered (OR 0.77, 95% CI 0.63 to 0.95), but does not seem to persist when studies with longer-term follow-up are analysed.
Interpretation
The presence of an ASD alone has been shown to be associated with the development of AT in 10% of patients by the age of 40 years. Preclosure incidence of AT is estimated to be approximately 20%.3 6 7
AT in patients with ASD is the result of cardiac remodelling secondary to longstanding haemodynamic overload. Sizeable ASD results in increased atrial size and stretch,7 12 45–50 right ventricular dilatation and dysfunction,7 elevation in pulmonary arterial pressure7 and tricuspid and mitral regurgitation.51
Atrial remodelling results in interstitial fibrosis and endo-epicardial dissociation which predisposes to arrhythmias (electrophysiological and structural remodelling).45 48 Electrophysiological remodelling manifests as non-uniform changes in the atrial effective refractory periods, conduction delays at the crista terminalis and impaired sinus node function.45 48–50 In addition, specific ion channel expression profiles representing ion channel remodelling have been demonstrated in AFIB.52–54
The effect of ASD closure on the risk of arrhythmia is likely to be the result of negative remodelling of the atria and right ventricle, which occurs after repair. Dramatic changes such as a reduction in right atrial and ventricular volume, an increase in right ventricular ejection fraction and an increase in left ventricular volume have been described following ASD closure.55 56 As ASD closure appears to result in partial or complete reversal of the associated haemodynamic changes, it is possible that it may also initiate reverse remodelling processes, and may explain the antiarrhythmic effect of ASD closure. Ion channel expression has been shown to revert in those who electrically cardiovert,52 53 and reversal of electrical remodelling is known to occur sooner than structural reversal,57 with animal studies showing almost immediate electrical reverse remodelling but persistent structural remodelling at four months.58 This is supported by our finding of a larger effect of ASD closure on AT at mid-term follow-up (OR 0.47, 95% CI 0.36 to 0.62) compared to the immediately post-repair period (OR 0.80, 95% CI 0.66 to 0.97), when remodelling has not yet occurred.57 60 However, the effect of ASD repair was lost at longer follow-up, suggesting that other mechanisms are in action (eg, ageing). We propose that such changes may be associated with the type of structural remodelling which is not reversible. This is with the acknowledgement that the long term data was not available for the majority of the larger and higher quality studies. This may have had a consequential statistical effect, so this interpretation is proposed with caution.
Care should also be exercised when comparing results from these different populations as studies with longer follow-up periods were more likely to include patients who underwent surgical closure, and had larger defects and more long-lasting ATs. In fact 29% of patients undergoing ASD closure have persistently increased right ventricular dimensions late after repair.7 56 This is likely to be due to incomplete reverse remodelling and could account for the persistence of AT in numerous patients.
A reduction in the prevalence of AT was seen after both surgical and percutaneous closure. This is consistent with previous studies which have not demonstrated any difference in remodelling between closure methods.56
Strengths and limitations
This study is the first systematic review and quantitative analysis of the evidence on the antiarrhythmic effect of ASD closure. As the best available evidence was evaluated within a robust statistical framework, this study provides accurate estimates of treatment effects in a clinical group in which adequately powered experimental studies are impossible due to the low prevalence of this condition and the established role of ASD closure in the management of these patients, which would not allow randomisation to a non-repair (placebo) arm.36 60
The validity of any meta-analytical review can potentially be compromised by heterogeneity in patient characteristics, therapeutic intervention or design between studies. The pathophysiological complexity of AT makes reviews in this area particularly prone and vulnerable to heterogeneity. We could not compare the outcomes for specific ASD sizes or types. Moreover, the duration of AT is known to affect the response to therapy, but this information was not available and the analysis may have included heterogeneous patient groups. Arrhythmia intervention prior to or during surgical intervention is also not uncommon nowadays and will certainly influence the risk of arrhythmia after repair. It was not possible to report on the pre- or post-closure antiarrhythmic pharmacological regimes used or their impact, since only two studies (Gatzoulis et al and Giardini et al) provided detailed and specific descriptions of this.
Variation in clinical end-points, their definitions, monitoring and reporting can also introduce error. Gatzoulis et al, for example, excluded asymptomatic patients who had non-sustained AFIB on Holter monitoring.7 Most of the studies did not report the monitoring methods used for AT and none specified the duration of each AT. Only four studies used the same AT monitoring method before and after closure. Furthermore, significant intraoperative factors exist which are known to potentially influence postoperative arrhythmia outcome, such as differing surgical practice and variation in the incidence and management of postoperative complications.
A random-effects model was used to better account for the inevitable clinical and methodological heterogeneity, however we were unable to demonstrate significant statistical heterogeneity This can be interpreted in two ways: either the various sources of heterogeneity ‘cancel each other out’ and the absence of statistical heterogeneity is merely an artefact of the analysis; or the antiarrhythmic effect that we demonstrate following ASD closure is readily generalisable to most ASD populations and closure methods. Examination of the study characteristics (table 1) suggests the latter.
Implication for further research
Several questions are raised by this study. First, it is important to establish if the lack of significant statistical heterogeneity among studies with different patient characteristics, therapeutic interventions and study designs truly represents the generalisability of the antiarrhythmic effect of ASD closure or whether it is merely an artefact of the analysis. This could take the form of retrospective analysis of the primary data of included studies, or a well designed experimental study.
Second, we found that a significant proportion of patients have persistent AT following ASD closure. The optimum management of these patients needs to be established. Ablation for chronic AFIB at the time of surgical ASD closure is well visited in the literature.7 12 51 61 Giamberti et al describe a series of 15 patients who were treated with concomitant radiofrequency ablation during surgical ASD closure, achieving a 93% reduction in pre-closure AT.62 Joint American Heart Association/American College of Cardiology guidelines recommend consideration of concomitant Maze procedures in those with intermittent or chronic AT.11 The experience with concomitant surgical ablation and ASD closure suggests that ablation may have a role in patients with persistent AT after ASD closure. However, further research is required to delineate what should be the indications and timing, especially given the findings in the literature, supported by this study, which suggest that reverse remodelling processes are active and that these may not achieve their maximal effect until some time following ASD closure.
Third, this study suggests that reverse remodelling processes may have a tangible clinical effect on AT caused by ASD when the haemodynamic changes resulting from ASD are reversed. The impact of these reverse remodelling processes on the cessation of AT at a molecular and cellular level needs to be better understood and characterised as this could yield novel therapeutic approaches for AT.
Finally, this study does not provide any evidence of a differential efficacy in surgical and percutaneous closure techniques for the termination of AT. As the anatomical indications for both techniques are different and well defined, further comparison of the antiarrhythmic effect of these interventions cannot be justified.11
Conclusions
ASD closure, whether surgical or percutaneous, is associated with a decrease in the post-closure prevalence of pre-existing AT. A similar effect was seen in patients after surgical ASD closure when only AFIB was considered. Further research is required to establish whether this effect is seen in all patient groups, to better understand the mechanisms that underlie this treatment effect and particularly to investigate the role of concomitant adjunctive antiarrhythmic interventions around the time of closure.
References
Footnotes
Funding This work was supported by the National Institute of Health Research Biomedical Research Centre and British Heart Foundation (RG05/009).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.