Article Text

Abstract
Background Calcified aortic valve stenosis (AVS) is a disease found in the elderly which is often complicated by severe co-morbidities.
Aims To assess the survival of conservatively treated patients >75 years with severe AVS compared to patients with non-severe AVS but who have a similar clinical risk profile; and to identify risk factors affecting prognosis.
Methods and results From 2002 to 2006, 161 patients (mean age 86±7.7 years) were studied: 79 with aortic valve area (AVA) <1 cm2 (group A), 82 with AVA ≥1 cm2 (group B). Cumulative mortality rates were 77.5% in group A, and 44.4% in group B. Survival rates at 6, 12, 18 and 24 months in groups A and B were: 70.9% versus 98.8%, 65.8% versus 84.1%, 49.4% versus 69.5% and 41.8% versus 59.8%, respectively. Independent predictors for death in group A were pulmonary artery pressure (PAP), the STS-PROM score, serum creatinine and diabetes. PAP >30 mm Hg identified patients at high mortality risk. In group B the predictive variables were ejection fraction, PAP, serum creatinine, and treatment with β-blockers or ACE inhibitors.
Conclusion Severe aortic valve stenosis is a medical condition with limited short-term survival in patients over the age of 75 years at high surgical risk. Clinical variables rather than symptomatic status were able to predict the patients' outcome. Patients with the highest surgical risk have the worst prognosis if AVS is not treated.
- Aortic valve stenosis
- prognosis
- aortic valve replacement
- perioperative mortality
- surgery-valve
- old age
- epidemiology
- aortic valve disease
Statistics from Altmetric.com
- Aortic valve stenosis
- prognosis
- aortic valve replacement
- perioperative mortality
- surgery-valve
- old age
- epidemiology
- aortic valve disease
Introduction
Aortic valve stenosis (AVS) is the most common valvular lesion in Europe and North America. Primarily, calcified aortic stenosis is present in 2–7% of the population aged >65 years,1 and its prevalence increases with age and concomitant cardiovascular disease.2 According to current knowledge, the prognosis of patients who are diagnosed with symptomatic AVS is relatively good but worsens significantly after the onset of symptoms, with an average survival of only 2–3 years.3 4 The only effective therapy for AVS is aortic valve replacement (AVR).5 Nonetheless, data from retrospective studies indicate that only one third of patients where severe AVS is present undergo surgical treatment.6 Those patients often have multiple co-morbidities, increasing perioperative mortality risk, and have symptoms which may not unequivocally relate to valvular heart disease. Complex risk calculation models like the Euro-SCORE (logistic or numeric)7 8 and the STS-PROM score have been established to guide clinical decision making when planning cardiovascular surgery. It is unclear whether those scores can help to define the outcome of medically treated patients.
In recent years, transcatheter aortic valve insertion (TAVI) has emerged as an alternative to surgical valve replacement for patients considered to be at very high operative risk. However, since 30-day mortality rates after TAVI have been reported to be 10%, rising to 22.1% after 8 months,9 there is a debate about whether elderly, multi-morbid patients do actually benefit from TAVI in terms of prolonged survival.
The aims of this prospective cohort study were, therefore: (i) to assess the survival of patients aged >75 years where severe AVS was present, conservative treatment was used and who were at high surgical risk, as compared to a control group with non-severe AVS; and (ii) to identify risk factors affecting the prognosis of those patients.
Patients and methods
Patient population
During the years 2002–06 all patients referred to our hospital for evaluation of the severity of their AVS were screened. Patients with severe AVS (defined as aortic valve area (AVA) <1 cm according to the AHA recommendations5) who were not referred for AVR because of high surgical risk10 11 were prospectively added to the study (group A). If patients were transferred for AVR during the follow-up period, they were subsequently excluded from the study. The control group consisted of patients with different stages of aortic valve calcification but non-severe AVS (group B). The control group was matched against the study group for age and baseline demographic and clinical variables. All patients received complete clinical and echocardiographic evaluation on entry to the study. Medical therapy was left to the discretion of the physicians in attendance; the aim was for all patients to receive optimised medical therapy using diuretics, ACE inhibitors and β-blockers if possible.
At the initiation of the study, owing to its observational type neither ethical approval procedure nor signed patient informed consent were stipulated by the German Drug Law12 or by regulatory bodies. Before study participation however, all patients were informed by the investigators about the aims and scope of the study and the fact that participation did not change the treatment in any way; all patients had to provide written informed consent for data collection and analysis. Data protection was fully ensured.
Echocardiography
All patients underwent a comprehensive two-dimensional and Doppler echocardiographic evaluation with commercially available ultrasound systems. Left ventricular mass and interventricular septal diameter were assessed from M-mode measurements of changes in left ventricular cavity and wall dimensions in the parasternal long-axis view. The apical long axis and four chamber view was used to calculate the left ventricular volume and ejection fraction following Simpson's rule and corrected compared to visual assessment of left ventricular function.13 Continuous-wave Doppler was used at multiple windows to obtain the maximal jet velocity over the aortic valve.14 The maximal instantaneous pressure gradient across the aortic valve was calculated by a modified Bernoulli equation. In patients with atrial fibrillation, velocities from several acquisitions were averaged. The aortic valve area was derived from the continuity equation. The maximal pulmonary artery pressure was calculated using continuous-wave Doppler over the tricuspid regurgitation in a modified four chamber view focusing on the right heart cavities. The degree of aortic valve calcification was scored according to previously described criteria.15
Follow-up
Patients were observed prospectively after the initial examination. Minimum follow-up time was 2 years. In order to acquire relevant information from all participating patients, a simple follow-up strategy was chosen: every 6 months after study entry all patients were contacted by telephone. The follow-up information was obtained from interviews with the patients, relatives or attending physicians. In those cases where a patient had died, the death certificates were reviewed after contacting the responsible authorities, which ruled out any uncertainties.
Mortality data and prognostic variables
The primary objective of this study was to investigate the cumulative mortality of medically treated severe AVS during the follow-up period as compared to a control group with similar clinical risk profile but non-severe AVS. Additionally, we aimed to identify risk factors affecting the patients' outcomes.
Documentation
The following parameters were documented on standardised electronic case report forms (eCRFs): initials, gender, age, medication, concomitant diseases (arterial hypertension, coronary heart disease, diabetes mellitus, chronic heart failure, history of arterial embolism/ stroke, chronic pulmonary disease) and AVS related symptoms. The echocardiographic parameters at initial presentation were collected as well as the predefined outcome data and medication during follow-up. The data sheets were designed to allow calculation of the Euro-SCORE and STS-PROM score based on the information obtained.
Statistics
Comparison of numerical variables was performed with the Student t test or Wilcoxon rank sum test, depending on variable distribution. The χ2 test or Fisher's exact test was used to compare qualitative variables. Comparison between groups was analysed with one-way analysis of variance (ANOVA) with Bonferri's post-tests. A Cox multivariate analysis including all variables with p<0.2 in the Cox univariate analysis was used to determine the predictive factors of cumulative late mortality. Survival rates up to 5 years were presented as Kaplan–Meier curves, and the log-rank test was used for comparison between groups. Differences were considered statistically significant at p<0.05. The data were analysed with SPSS 17.0.1 (for Windows, Chicago, Illinois).
Results
Baseline characteristics
Between the years 2002 and 2006, 171 patients were included in the study. Ten of these patients underwent surgical aortic valve replacement during the follow-up period and were subsequently excluded from the study. The final study group consisted of 161 patients, 79 with AVA <1 cm2 (group A), and 82 with AVA ≥1. The mean age of patients in the study group was 86±7.7 years; creatinine clearance was 38.1±15.7 ml/min, ejection fraction 49.8±10.3%; BMI 26.2±4.8 kg/m2 and follow-up time 25.0±17.4 months. Overall, 332.8 follow-up years were reviewed for the occurrence of death within the study groups (group A, 142.6 years; group B, 190.2 years). Using a simple follow-up strategy, it was possible to obtain outcome information in all cases. Patients with severe AVS did not differ significantly from the control group with respect to the baseline demographic data, the incidence of concomitant cardiovascular disease and functional status (table 1).
Baseline characteristics and demographic data
Survival analysis
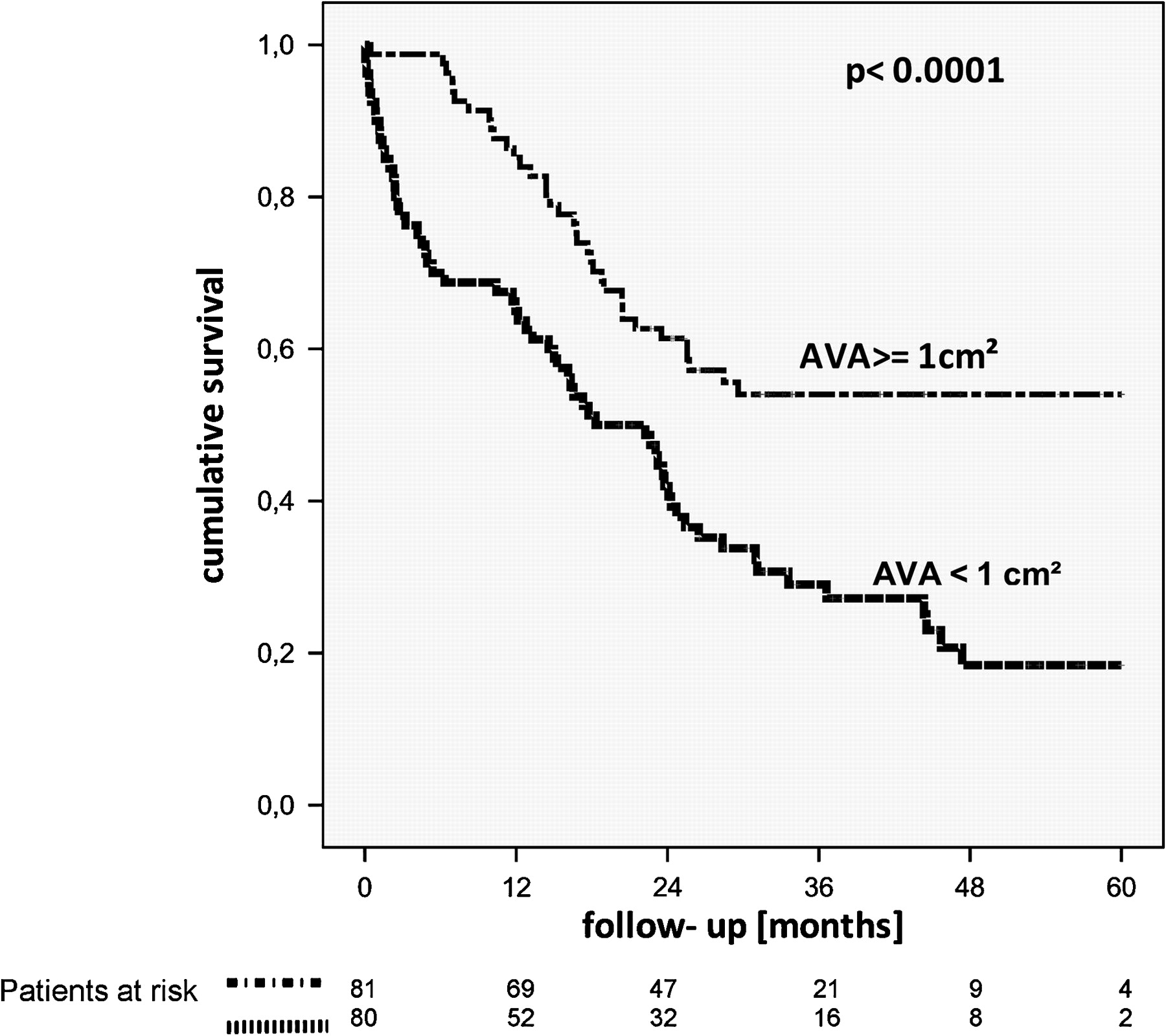
Overall 60.9% of the patients died during follow-up. The cumulative mortality rate in patients with severe AVS (group A) was 77.5%, with a mean survival time of 16.4±16.1 months (10 days to 73.5 months); 44.4% of patients with non-severe AVS died during follow-up (OR 4.3, 95% CI 2.2 to 8.5, p<0.0001; figure 1).
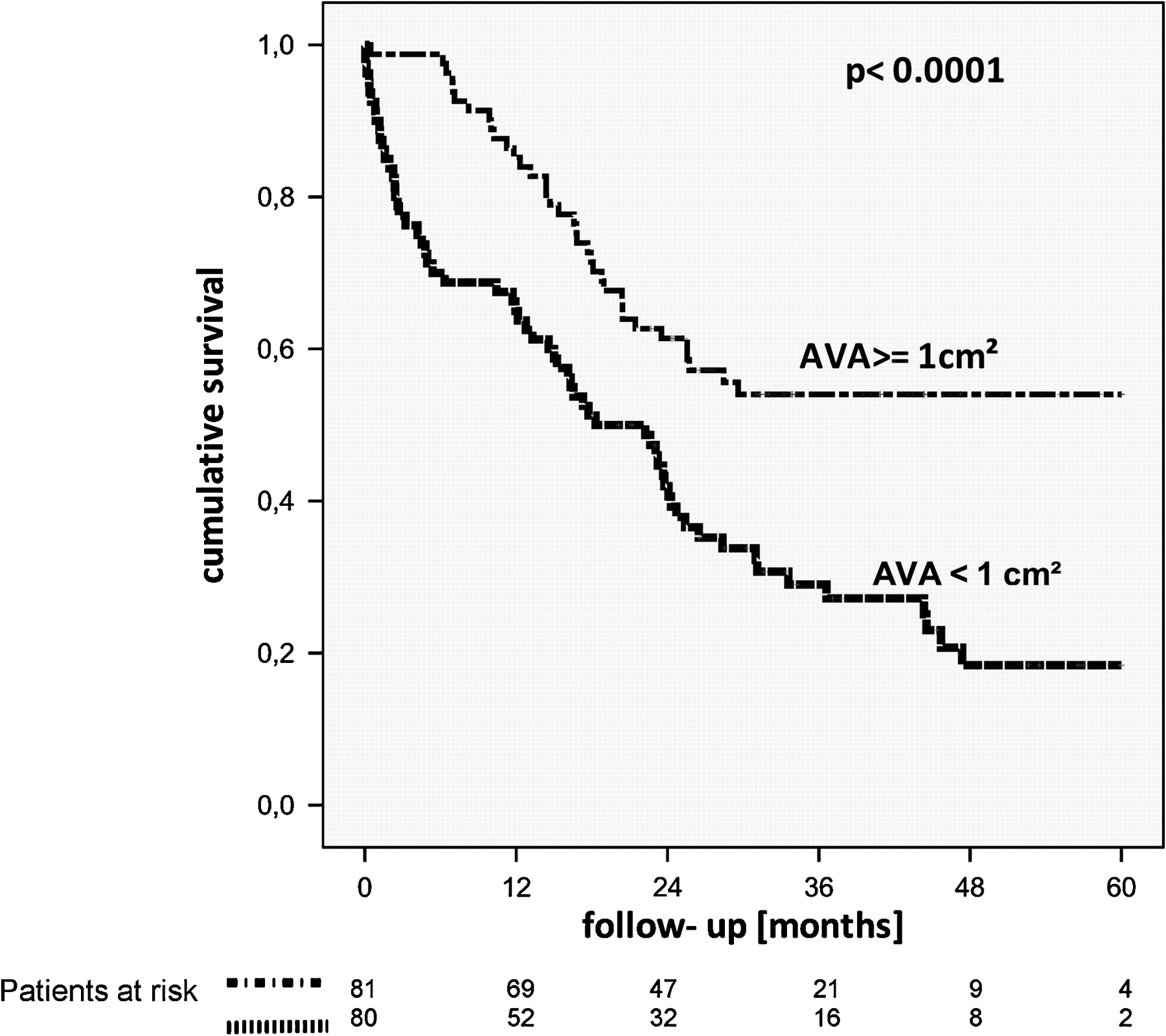
Kaplan–Meier curves of mortality rates within the study population depending on the severity of aortic valve stenosis. AVA, aortic valve area.
Survival rates at 6, 12, 18 and 24 months between groups A and B were 70.9% and 98.8% (OR 34.28, 95% CI 4.50 to 260.89, p<0.0001), 65.8% and 84.1% (OR 3.09, 95% CI 1.44 to 6.67, p=0.003), 49.4% and 69.5% (OR 2.49, 95% CI 1.30 to 4.77, p=0.006), and 41.8% and 59.8% (OR 2.18, 95% CI 1.16 to 4.09, p=0.01), respectively.
Outcome variables
Multivariate regression analysis identified increasing PAP, the STS-PROM score, serum creatinine and diabetes as independent predictors for death in patients with severe AVS (table 2a).
Multivariate regression analysis of predictors for overall mortality in patients with severe and non-severe aortic valve stenosis (AVS)
As the most predictive single variable, PAP ≥30 mm Hg identified patients with severe AVS at high mortality risk (OR 15.4, 95% CI 4.4 to 54.2, p<0.0001; figure 2). When comparing patients with PAP <30 mm Hg from group A to patients without relevant AVS, the difference in survival was no longer statistically significant (p=0.32; figure 3).

Kaplan–Meier curves of cumulative mortality rates depending on measured pulmonary artery pressure (PAP) during echocardiography. PAP <30 mm Hg distinguished patients with severe aortic valve stenosis and relatively good prognosis from those with higher mortality rates.

Kaplan–Meier curves of cumulative survival rates of patients with severe aortic valve stenosis (AVS) and pulmonary artery pressure (PAP) <30 mm Hg compared to patients with non-severe AVS. AVA, aortic valve area.
We plotted receiver operating characteristic (ROC) curves to visualise the sensitivity and specificity of single variables to predict cumulative mortality rates in patients with severe AVS (figure 4A–D). ‘Classical’ clinical risk factors like age, severity of symptoms or incidence of syncope failed to predict any adverse outcome for patients in group A, and medical treatment did not relevantly influence patient survival.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A–D) Receiver operating characteristic curves to determine the sensitivity and specificity of single variables to predict cumulative mortality rates of patients with severe aortic valve stenosis. AUC, area under the curve; PAP, pulmonary artery pressure.
In group B the variables predicting mortality were PAP, ejection fraction and serum creatinine, whereas medical therapy with β-blockers and ACE inhibitors had a beneficial effect on survival (table 2b).
Discussion
To the best of our knowledge, this is the first prospective study aiming to investigate the outcome of medically treated patients over the age of 75 years with severe AVS at high surgical risk compared to a control group with a similar clinical risk profile. The number of patients with severe AVS, who completed a minimum of 24 months follow-up is significantly higher than in other studies dealing with this topic. Of note, this is the only study on elderly patients with relevant co-morbidities in whom AVR has been denied.
Available data
Several well designed studies have been published investigating the outcome of asymptomatic patients with severe AVS. A consistent message has emerged, that the prognosis of truly asymptomatic individuals is relatively good.13 15–17
On the other hand current data are rare concerning the outcome of medically treated severe AVS at high risk for surgery. Chizner et al reported on poor survival rates of 12 patients with a mean age of 58.2±9.2 years who had severe, symptomatic AVS. Mortality rates increase significantly after the onset of AVS-related symptoms, with an average survival of only 57% after 3 years.18
Hostkotte et al showed in 55 patients, aged 66±12 years with severe AVS refusing AVR, that untreated AVS has a high short term mortality, with an average survival of only 23 months after diagnosis and a 5-year probability of survival of 28%.19 Schwarz et al showed in 144 patients, of whom 19 (aged 47.1±12.1 years) refused surgery, that AVR increased survival substantially after 3 years (87% vs 21%).20 Only Iivanainen et al included a small number of patients (13) with severe AVS aged over 75 years; they reported a sixfold increased risk of death as compared to patients undergoing AVR.21
These studies were published between the years 1980 and 1996. Due to the demographic development over the last few years, AVS has become a disease of the elderly in whom relevant co-morbidities are present and where recent data on this patient group are lacking.
Varadarajan et al showed more recently in a retrospective analysis of patient files, that only 38% of elderly patients with either symptomatic or asymptomatic severe AVS receive AVR; the survival of medically treated patients at 1, 5, and 10 years was 62%, 32% and 18%, respectively.6
The survival rates in our group with severe AVS were similar, with 70.9% at 1 year and 41.8% at 2 years. In contrast to the available data, the mean age in our study group was significantly higher (86±7.7 years), and all patients were considered at high surgical risk.
Current guidelines
Current guidelines give a class IA recommendation on surgical treatment in patients with symptomatic severe AVS, emphasising that AVR is the only reasonable therapy for this medical condition. There are no explicit restrictions for AVR related to age itself or co-morbidities.
Since recent data on conservatively treated patients with severe AVS are lacking, these recommendations are based on early landmark studies.5 13 However, due to demographic development over the last few decades, physicians are confronted with new challenges complicating clinical decision making in patients with severe AVS. Calcified AVS is a disease of the elderly which is frequently complicated by relevant co-morbidities. Clinical decision-making should take into account the patients' life expectancy and quality of life regardless of AVS.5 13 Only limited data have been published as to whether elderly patients at high surgical risk do still benefit from AVR in terms of prolonged survival, or whether AVR is just a perilous and costly way to improve the quality of life of those who survive surgery.
In recent years TAVI has emerged as an alternative to surgical valve replacement for patients considered at very high operative risk.11 22 The percentage of patients undergoing TAVI instead of surgical AVR is constantly increasing, even if current guidelines do not give explicit recommendations on patient selection for these newer methods.
In this context our data are very important as they show: (i) severe AVS remains an important risk factor for death in elderly, multi-morbid patients, when compared to a control group with a similar clinical risk profile; (ii) cumulative survival is predominantly affected by high short-term mortality; and (iii) patients at highest estimated surgical risk (as defined by the STS-PROM score or raised PAP) have the worst prognosis if AVS is not treated.
Risk assessment
In our patient cohort the ‘classical’, clinical risk factors (functional NYHA class, angina pectoris or onset/frequency of syncope) failed to predict the patients' outcome. This is due to several reasons: (i) some of these patients present after onset of AVS related symptoms and clinical risk factors have not been tested to sub-specify outcome in those patients; (ii) AVS related symptoms often do not occur in the elderly when functional capability is restricted due to other reasons; and (iii) it is often difficult to distinguish AVS related symptoms from concomitant ‘cardiorespiratory’ illnesses. Therefore, the need for impartial outcome variables in those high-risk, but ‘real-life’ patients is obvious. Our results indicate that objective risk assessment using clinical variables alone, or in combination with established risk scores, identifies patients at high mortality risk. Interestingly, the determination of PAP during echocardiography was extremely helpful in distinguishing patients with AVS with a relatively good prognosis from those with a worse outcome.
Reasons for non-surgical treatment
Several studies indicate that a relevant proportion of elderly patients with either symptomatic or asymptomatic severe AVS do not receive AVR, even if current guidelines clearly indicate that AVR is the only reasonable therapy for those patients independent of the patient's age or co-morbidities.6 23 The reasons for this discrepancy are unclear since it has not been systematically investigated.
Our study included elderly patients with severe AVS and complicating co-morbidities. An average Euro-SCORE of 25.37±18.29 and an STS-PROM score of 10.1±4.3 indicate a high surgical risk if those patients undergo surgical valve replacement. The reasons why these patients were not referred to surgery were as follows. Six patients (7.5%) presented with critical medical conditions; in those cases surgery was denied by the patients' relatives, attending physicians and surgeons. In 41 cases (51.25%), the patients themselves declined surgery immediately after diagnosis of AVS, or after contacting their relatives and/or referring physician. Those cases were never discussed with a surgeon because of the patients' wish to avoid open heart surgery. Nineteen patients (23.75%) were evaluated for surgery and considered to be at very high surgical risk due to complicating co-morbidities. In those cases surgery was declined by surgeons. In 14 cases (17.5%) surgery was declined by cardiologists after evaluating the patients' surgical risk or because of compelling indications (eg, disabling stroke, dementia, physical debility); those patients' cases were also not discussed with a surgeon.
In summary, most patients refused AVR because they wanted to avoid extensive open heart surgery and/or the patients were concerned about the operative mortality risk. However, when taking into account the limited prognosis of untreated AVS, especially in patients considered at high surgical risk, attending physicians should make greater efforts to increase the number of patients referred to AVR. Future studies will show whether less invasive methods of TAVI will help to increase the number of patients undergoing AVR.
Limitations
This study is limited by the single site data collection. We cannot exclude decision bias from the referring physicians. In our study follow-up was carried out by telephone calls which helped to minimise the drop-out rate in our extremely elderly patients; nonetheless, we had no chance to perform additional transthoracic echocardiographies (TTEs) or subsequent clinical examinations. The predictable value of the identified prognostic variables must be tested prospectively before a validated risk score can be established.
Conclusion and clinical implications
Our data provide information on survival in patients with severe AVS who decline operative treatment; there is a limited short term survival in patients over the age of 75 years who are at high surgical risk. Clinical variables rather than symptomatic status were able to predict outcome. Patients at highest surgical risk have the worst prognosis if AVS is untreated.
References
Footnotes
RS and CH contributed equally to the article and the conduct of the study.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.