Article Text

Abstract
Background Corrective surgery for congenital heart disease may be life-saving, but its utilisation depends upon several social and economic factors. Girls with cardiac defects may not receive equitable care in India, but this has not been systematically studied.
Methods In this prospective study, parents or guardians of 405 consecutive children aged up to 12 years (mean±SD age 3.43±3.44 years; 271 boys) who had been advised to undergo elective paediatric cardiac surgery were interviewed using a validated questionnaire. The status of the patients was reviewed after a year and the factors associated with non-compliance with treatment were analysed. In a qualitative sub-study the parents of 20 children who had not undergone surgery were interviewed. Qualitative data were analysed using an inductive analytical approach.
Results Of the 405 patients studied, 44% (59/134) of girls had undergone surgery at 1 year compared with 70% (189/271) of boys (χ2=24.97; p<0.001). Independent predictors for non-compliance with surgery included female gender (OR 3.46, 95% CI −2.06 to 5.80; p<0.0001), lower socioeconomic classes (lower-middle: OR 18.62, 95% CI −2.14 to 161.8, p=0.008; upper-lower: OR 34.27, 95% CI −3.72 to 316.0, p=0.002) and higher cost of surgery (OR 1.92, 95% CI −1.06 to 3.47, p=0.03). In the in-depth interviews, apprehensions about future matrimonial prospects of girls and lack of social support emerged as the major factors responsible for delays in undergoing surgery.
Conclusions Female gender is an important determinant of non-compliance with paediatric cardiac surgery. Deep-seated social factors underlie this gender bias.
- Surgery-paediatric
- paediatric surgery
Statistics from Altmetric.com
What this paper adds
Gender inequality exists in the utilisation of healthcare services in India.
The magnitude has not been prospectively studied.
Significant gender bias exists in the acceptance of paediatric cardiac surgery.
Out of 100 boys and girls with congenital heart defects it can be estimated that, for 70 boys who have an operation, only 22 girls undergo surgery.
Qualitative study suggests that deep-seated social factors underlie this gender bias.
Corrective measures are urgently needed to correct this disparity.
Introduction
In India approximately 180 000 children are born with congenital heart disease (CHD) each year, of whom 60 000–90 000 require early intervention.1 However, the actual number of children undergoing surgery is far lower. This is attributable to various reasons including limited healthcare resources and sociocultural factors.2 Considering that serious CHD among boys and girls is equally common,3 4 it would be expected that the number of girls and boys undergoing surgery is comparable. However, gender disparity in healthcare is widely prevalent, including in the developed world,5–10 and may be more pronounced in India and in other developing countries. Gender bias is likely to be a particularly important factor in the provision of healthcare in India, given the general lack of empowerment of women and the preference for boys in the country.11 The presence and magnitude of gender bias in the Indian healthcare system have not been quantified in prospective studies.
Early diagnosis and timely corrective surgery is essential in children with serious CHD, and has led to an increasing population of adults with treated congenital defects.12 However, in the developing countries the burden of adults with CHD largely includes unoperated CHD. Denying paediatric cardiac surgery leads to worse outcomes and delaying may have an impact on patient safety and outcomes.13
The aim of the present study was to quantify gender bias and to study the other socioeconomic factors governing compliance with paediatric cardiac surgery in India.
Methods
Parents or guardians of 405 consecutive children aged <12 years who had been recommended surgery within 3 months for a congenital heart defect were interviewed during a 4-month period from 1 February to 31 May 2009. Informed consent was obtained from the parents or guardians of the children. Exclusion criteria included unwillingness of parents or guardians to participate, previous cardiac surgery, need for emergency cardiac surgery, the presence of comorbid conditions, multiple congenital anomalies and congenital syndromes that may influence the outcome. The study protocol was approved by the ethics committee of the All India Institute of Medical Sciences.
Questionnaire development and administration
The interviews were conducted using a predesigned questionnaire (additional appendix 1) by either of two interviewers (RK, SJ). Socioeconomic class was assigned to the family according to the modified Kuppuswamy scale 2007.14 This scale is validated for use in the Indian population and takes into account the occupation of the head of the household, his/her education and the monthly income of the family from all sources. The scale includes five socioeconomic classes (highest to lowest: upper, upper-middle, lower-middle, upper-lower and lower classes).
The initial questionnaire was designed following focus group discussions with paediatric cardiologists, cardiac surgeons, medical social workers and clinical psychologists. The questionnaire was originally designed in English and was translated into the local language (Hindi). The vernacular questionnaire was back-translated to English by an expert and was found to be consistent with the original version. Pretesting of the questionnaire was done on 30 subjects. The inter-rater variability was acceptable on re-interviewing the 15 parents by two interviewers on separate occasions. Reproducibility was established by re-interviewing the 15 parents after 7 days. The three most common concerns expressed by the parents were identified and formulated into questions for the questionnaire of the main study. These included whether a surgical scar on the chest of the child was a problem for the family, fear that the surgery might dampen the future matrimonial prospects of the child, and the need to conceal the illness of the child from others. The questions were standardised by a clinical psychologist both before and after the pretest. An average interview lasted nearly 10 min. The interview was conducted in the vernacular language, in a quiet room where the subjects' responses could not be overheard by anyone else and complete confidentiality of individual information was ensured.
After 1 year from the last interview, the surgical status of the patients was recorded by a medical record review and telephone confirmation. Deaths, if any, during the period of follow-up were also recorded from the hospital records and telephone contact with the child's parents (see appendix 2 available from the corresponding author).
Qualitative analysis
The qualitative study included a semi-structured interview session with the parents or guardians of the children by a certified clinical psychologist (SK) after obtaining written informed consent. Guiding questions for patient interviews were developed through two focus group discussions following the initial quantitative study, one with paediatric cardiologists and the other with medical social service officers of our department. Semi-structured recorded interviews were held with purposively selected parents of 20 children who had not undergone surgery 1 year after recommendation. Of the 22 parents who were approached, only two refused to participate.
In the 60–90-min interviews the respondents gave their views on reasons for the delay in surgery, the social/monetary support in handling child's illness, the barriers in accessing and utilising paediatric cardiac healthcare services and concerns about future prospects of operated children. All interviews were transcribed and validated against the recorded material by the interviewer. The transcribed interviews were analysed inductively and thematically. Emerging themes from concurrent inductive analysis were explored and challenged in later interviews. Two group discussions were done to review themes and clarify facts. We report only themes that were mentioned by at least three respondents.
Statistical analysis
We assumed that the number of boys and girls eligible for cardiac surgery would be equal. Assuming that 90% of boys would undergo surgery as recommended, 416 children would need to be recruited to detect a 10% absolute reduction in compliance with surgery among girls with 90% power and 5% α error. Data are presented as number (%) or mean±SD/median (range) as appropriate. Univariate analysis was done using the Student t test or Wilcoxon rank-sum test for continuous data and the χ2 test or Fisher exact test for categorical variables. To determine the predictors of non-compliance with paediatric cardiac surgery, a univariate logistic regression analysis followed by a multivariable logistic regression method were used. In the final prediction model, all the variables thought to be clinically important (age and sex of the patient, education of the head of the household, socioeconomic class of the family, religion, domicile, number of children, birth order, diagnosis of the cardiac condition, type of surgery planned, the cost of surgery and willingness to get the surgery done in the first visit) were included and the results reported as adjusted OR with 95% CI. We also evaluated the predictors of non-compliance with surgery among girls separately using a univariate logistic regression model. p Values <0.05 were considered significant. All analyses were performed using Stata 9.0. Qualitative data were analysed using Nudist software.
Results
Of the 405 patients studied, 271 were boys and 134 were girls, a sex ratio of 2:1. The mean age at enrolment was 3.4 years and was similar for both boys and girls; 45% (n=184) of the patients were <2 years of age and 22.5% (n=91) were aged <6 months. The demographic and baseline clinical characteristics of the patients are summarised in table 1. Most of the patients came from rural areas and belonged to the lower socioeconomic classes (table 1). Notably, however, none of the patients belonged to the lowest class (ie, the ‘lower’ class). Ventricular septal defect was the most common CHD seen in patients (24%), followed by tetrology of Fallot (22%) and atrial septal defect (10%). The mean duration of symptoms of the cardiac condition was 24.9 months, while the duration since diagnosis of a cardiac condition was 17.9 months. Definitive repair was recommended in 83% of cases, and in 17% palliative surgery was offered. The palliative surgery recommended included Blalock–Taussig shunt (7%), pulmonary artery banding (4%), Glenn (3%) and Fontan operation (1%). The cost of surgery recommended for most of the patients was around INR 55 000 (approximately $1200).
Demographic and clinical characteristics of study subjects
Factors affecting compliance with surgery
Significantly more boys than girls had undergone the recommended cardiac surgery at 1 year (70% vs 44%, p<0.0001). The univariate factors affecting compliance with the recommended surgery at 1 year of follow-up are presented in table 2. A difference was also seen across socioeconomic classes: >80% of children in the ‘upper’ and ‘upper-middle’ classes had undergone surgery compared with <60% of patients in the ‘lower-middle’ and ‘upper-lower’ classes (p<0.0001). A higher educational status of the head of the household was associated with better compliance with recommendation for surgery. The total number of siblings and the order of the patient among them were also significant univariate predictors of delay. Religion and rural or urban status were not predictive of delay. State of residence of the patient as categorised by EAG (Empowered Action Group), the eight socioeconomically backward states and geographical location of the state were also not predictive of a delay. Similarly, the diagnosis of the condition and the type of surgery did not have any bearing on the acceptability of surgery, but there was a difference in the surgery status with respect to the cost of surgery. When the surgical cost was ≤INR 50 000, 70% of children underwent the recommended surgery compared with 58% if the cost of surgery was >INR 50 000.
Factors affecting status of surgery on univariate analysis
On multivariate logistic regression analysis, female sex (p<0.0001), ‘lower-middle’ (p=0.008) and ‘upper-lower’ (p=0.002) socioeconomic classes (which are the lowest classes included in the study group) and cost of surgery >INR 50 000 (p=0.03) were independent factors influencing the surgery status of the patients (figure 1).
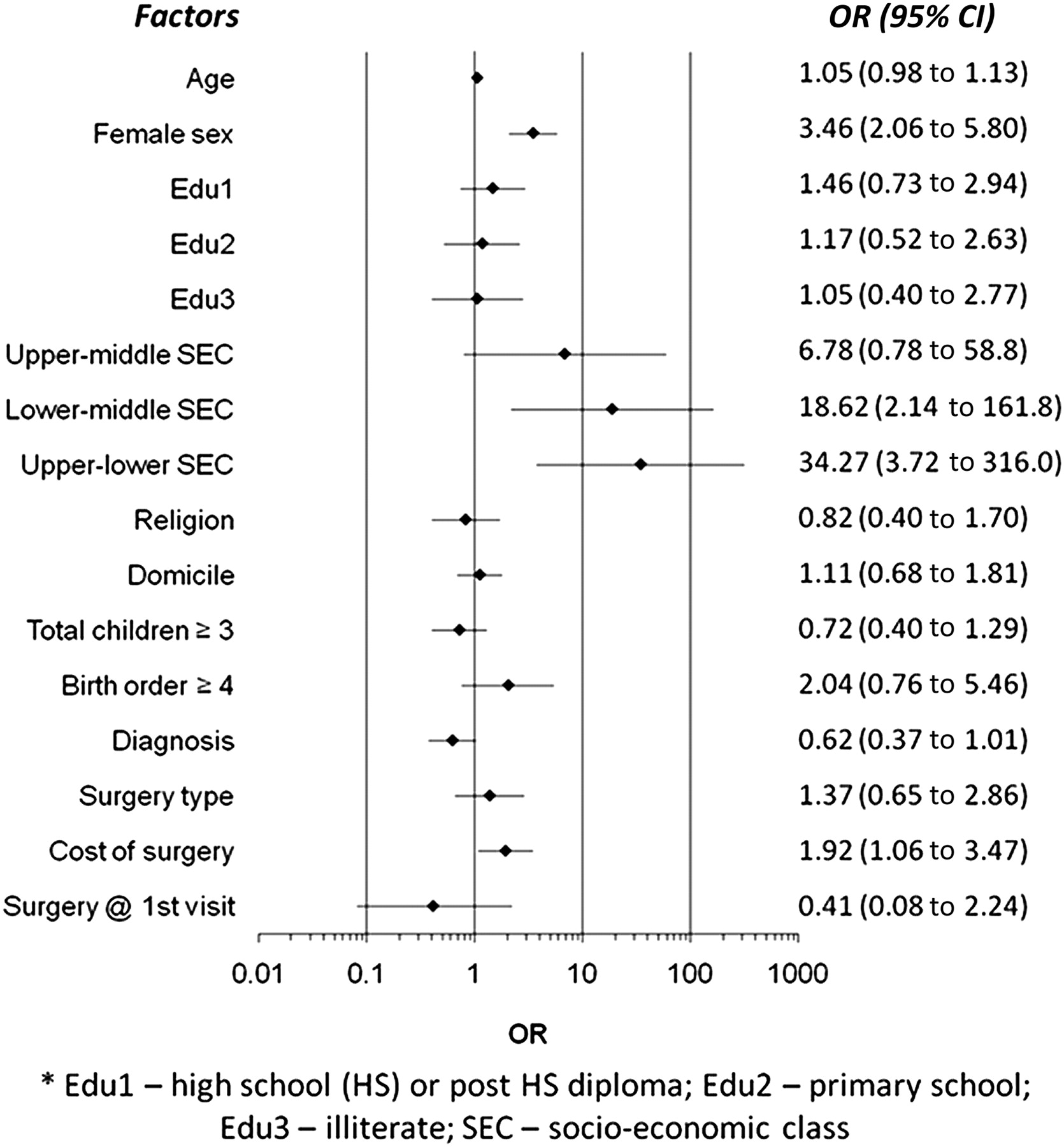
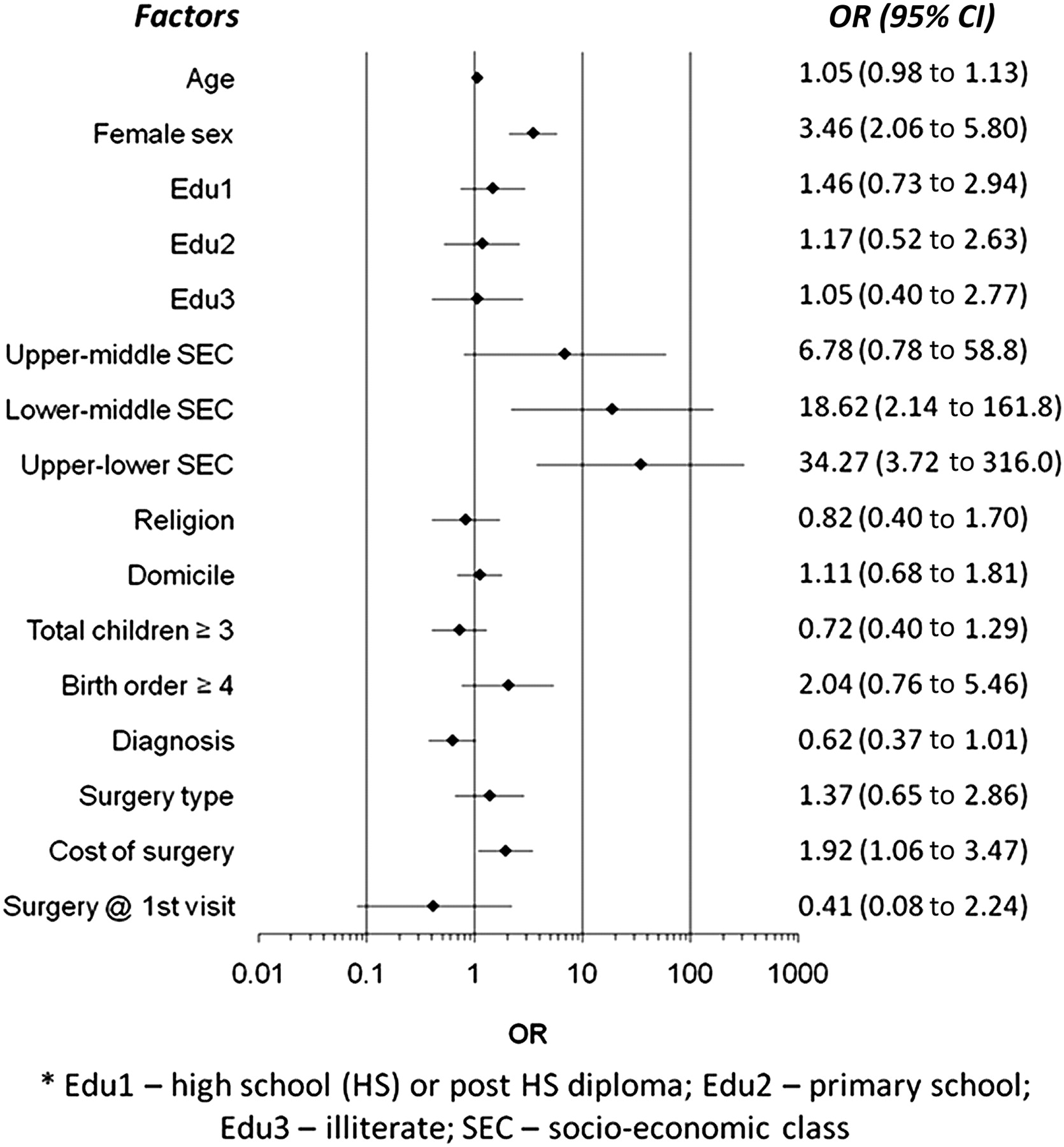{kind=link}
Factors independently affecting surgery status (logistic regression analysis).
Factors influencing compliance with surgery among girls
In the subgroup of girls (table 3), socioeconomic status was an important determinant of surgery status (p<0.002) with the percentage of patients undergoing surgery progressively decreasing from the ‘upper’ class (90%) to the ‘upper-lower’ class (21.3%). Similarly, a lower educational level of the head of household was associated with poorer compliance with surgery (p=0.001). Being a younger child in the family was associated with lower rates of undergoing surgery (p=0.004).
Factors affecting status of surgery among female patients
Social issues related to cardiac surgery
The families of 31/134 girls (23.1%) felt the need to conceal the illness of their child from relatives and friends compared with 4/271 (1.5%) boys' families (p<0.0001). A postoperative scar on the chest of the child was perceived as a problem for the parents of 62% of girls (83/134) compared with only 6% of boys (16/271, p<0.0001). Parents of girls were more fearful that surgery might dampen the matrimonial prospects of their child than parents of boys (65% (87/134) vs 2% (5/271); p<0.0001).
Qualitative interviews: reasons for the delay
The qualitative interviews were conducted among the parents of 20 children (12 boys and 8 girls). The concern that a surgical intervention might adversely affect the future matrimonial prospects of the child was a recurring theme and was expressed by parents of six girls but not by any parents of boys. The parents of girls were concerned that a ‘dubious’ past medical history as well as the scar of surgery would be detrimental to the future of their daughters. For all the boys, financial incapability was quoted as the major factor responsible for a delay in surgery. On the other hand, for girls the lack of support from relatives was the major factor responsible for this delay. Parents of boys often deferred having children for some time to give their ‘full-time attention and resources’ to the child with CHD, while only half of the parents of girls expressed such an opinion. Other issues that emerged were parents' ‘karma’ being responsible for the child's disease; village myths that delay the decision to opt for surgery (eg, the curative powers of faith healers and the disease-curing potential of dietary or lifestyle modifications in the treatment of CHD); the fear of undergoing surgery; and the apprehensions arising out of the need to visit big cities for surgical treatment.
Discussion
Our study shows that girls are significantly less likely to undergo recommended cardiac surgery than boys. Other major factors affecting compliance with paediatric cardiac surgery in India are socioeconomic class and cost of surgery. In a developing country like India the healthcare resources are limited and the vulnerable sections of the society are marginalised. Not only was the acceptance of surgical paediatric cardiac care lower among girls, but the access to such care was also lower. The number of boys and girls who sought paediatric cardiac care at our centre in 2009 was 3187 and 1400, respectively, similar to the ratio observed in our study population. Considering an equal incidence of serious CHD among boys and girls and based on the access and acceptance rate seen in the study, out of 100 boys and girls with congenital heart defects it can be estimated that, for 70 boys who have an operation, only 22 girls will undergo surgery.
Gender disparity in access to healthcare is widely prevalent across the world. Women are less likely than men to receive thrombolysis,6 to undergo angiography8 and to receive cardioprotective medications for primary and secondary prevention of cardiovascular diseases, even in the developed world.9 10 Surprisingly, gender equality in the utilisation of healthcare systems has not been evaluated in prospective studies, resulting in varied estimations of gender disparity among similar populations depending on the method used.8 15 Recent reviews of CHD from other developing countries make no mention of gender disparities in healthcare.16 In a retrospective study of paediatric admissions in Hong Kong, a significant gender disparity was found but was suggested to be due to male vulnerability to diseases.17 However, there was no gender disparity for acyanotic heart disease-related admissions. In our study, cyanotic heart disease almost emerged as a significant factor predicting the likelihood of surgery in both sexes. Delaying paediatric cardiac surgery leads to worse outcomes. The outcome in adults with CHD is shown to be inferior in women even in the developed world,18 and poor acceptability or delay in opting for surgery may further worsen the outcomes.
Very few studies have addressed the issue of gender disparity in the utilisation of healthcare in India. An analysis of the Indian national sample survey published in 200419 suggested that households facing financial constraints are more likely to spend their meagre resources on hospitalisation of boys than girls. The results of a small study among parents of newborn infants also suggested that the perception of illness and spending on health was lower for newborn girls than boys.20 A recently published retrospective study suggested a significant gender disparity among children undergoing paediatric cardiac surgery.21
The strength of our study is that it is prospective and enrolled a large and representative sample of children. Both quantitative and qualitative methods are needed to assess non-compliance with surgery in a comprehensive manner. The qualitative arm added value and helped in identifying social and cultural reasons for non-compliance with surgery. Qualitative research methods are ideally suited for such detailed exploration of cultural attitudes and norms. The qualitative findings were also validated using triangulation.
The sample size calculations were done on the basis of available data which suggest that a vast majority of CHD does not show gender preponderance.3 4 We wanted the sample size calculations to be unbiased and not to be affected by popular belief that healthcare-seeking behaviour is gender-driven. Surprisingly, there were no subjects from the lowermost socioeconomic class (the ‘lower class’). The ‘lower’ socioeconomic class represents a group with very poor healthcare-seeking behaviour associated with extremely low standards of literacy and income.
The reasons for this unacceptable level of gender disparity were multifactorial. Lower socioeconomic class clearly puts girls at a distinct disadvantage in accessing and accepting tertiary healthcare facilities compared with boys. On moving down the socioeconomic scale, a progressively lower percentage of patients had undergone surgery, although per capita income alone was not independently predictive of the decision to undergo surgery. A higher educational status of the head of the household was significantly associated with higher rates of opting for surgery. Our quantitative and qualitative studies showed that concerns regarding a postoperative scar and future matrimonial prospects were significantly greater for girls than for boys. Social issues peculiar to India may be important reasons for this disparity, which include arranged marriages with the custom of ‘dowry’ and the lack of empowerment of women even in day-to-day running of the family. In a society where a large number of female feticides happen for such social occurrences, they are also the likely reasons for a delay in cardiac surgery in children. Delaying/denying paediatric cardiac surgery to girls may represent a practice akin to female feticide.
Fortunately, there is evidence that sex-related inequalities in health and healthcare can be overcome.22 Persistent gender disparity across the world necessitated the inclusion of gender equality and empowering of woman among the Millennium development goals of the United Nations,23 and women-centred focus is a core principle of US President's global health initiative.24 Even though the ultimate solution lies in the social empowerment of women, an immediate solution is desirable. Subsidising the cost of surgery for girls or offering monetary incentives, plastic surgery for the scar, a programme to empower, employ and educate girls who undergo surgery and more widespread use of device closures for atrial septal defects and ductus arteriosus may reduce the social concerns and thus may reduce this gender disparity.
In conclusion, significant gender bias exists in the acceptance of paediatric cardiac surgical care. Deep-seated social factors underlie this gender bias and corrective measures are urgently needed to correct this disparity.
References
Footnotes
See Editorial, p 1897
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the All India Institute of Medical Sciences, New Delhi.
Provenance and peer review Not commissioned; externally peer reviewed.