Article Text

Abstract
This review addresses recent advances in the epidemiology, pathogenesis and prognosis of acute heart failure and cardiomyopathy based on research conducted in Africa. We searched Medline/PubMed for publications on acute decompensated heart failure and cardiomyopathy in Africa for the past 5 years (ie, 1 January 2008 to 31 December 2012). This was supplemented with personal communications with colleagues from Africa working in the field. A large prospective registry has shown that acute decompensated heart failure is caused by hypertension, cardiomyopathy and rheumatic heart disease in 90% of cases, a pattern that is in contrast with the dominance of coronary artery disease in North America and Europe. Furthermore, acute heart failure is a disease of the young with a mean age of 52 years, occurs equally in men and women, and is associated with high mortality at 6 months (∼18%), which is, however, similar to that observed in non-African heart failure registries, suggesting that heart failure has a dire prognosis globally, regardless of aetiology. The molecular genetics of dilated cardiomyopathy, hypertrophic cardiomyopathy and arrhythmogenic right ventricular cardiomyopathy in Africans is consistent with observations elsewhere in the world; the unique founder effects in the Afrikaner provide an opportunity for the study of genotype–phenotype correlations in large numbers of individuals with cardiomyopathy due to the same mutation. Advances in the understanding of the molecular mechanisms of peripartum cardiomyopathy have led to promising clinical trials of bromocriptine in the treatment of peripartum heart failure. The key challenges of management of heart failure are the urgent need to increase the use of proven treatments by physicians, and the control of hypertension in primary care and at the population level.
- HEART FAILURE
Statistics from Altmetric.com
Introduction
Heart failure is a clinical syndrome that develops as a consequence of cardiac disease, and is recognised by a constellation of symptoms of effort intolerance and signs of fluid retention produced by neurohumoral responses to cardiac dysfunction.1 The syndrome may occur as the end result of damage caused by a number of disease processes affecting the structure and function of the heart. In Western developed countries, coronary artery disease, either alone or in combination with hypertension, is the most common cause of heart failure.2 In contrast, cardiomyopathy and rheumatic heart disease have historically been considered to be the major causes of heart failure in sub-Saharan Africa, accounting for nearly half of all cases of presentations to hospital in the period between 1957 and 2005.3
The cardiomyopathies pose a potential great challenge in Africa because of: their higher prevalence in societies still plagued by diseases of famine and pestilence; the difficulty of diagnosis, which often requires specialised cardiological investigations that are lacking in resource-poor environments; the limited access to effective interventions, such as heart transplantation; and the high mortality associated with these often irreversible disorders of heart muscle.4 There has been important new research on the epidemiology, pathogenesis and prognosis of heart failure and cardiomyopathy in Africans since the last major reviews on the subject were published between 2005 and 2009.3 ,5 ,6 The new research provides information that is relevant to the treatment and prevention of heart failure and cardiomyopathy in African patients. This review seeks to summarise the advances that have been made mainly over the past 5 years, and addresses their implications for the prevention, treatment and investigation of these disorders in Africa.
What is new on the epidemiology of acute heart failure and cardiomyopathy in Africans?
Heart failure
Acute decompensated heart failure is the most common primary diagnosis for patients admitted to hospital with heart disease in Africa.7 ,8 The sub-Saharan Africa Survey of Heart Failure (THESUS-HF) is the first and largest multicentre registry of acute heart failure in Africa to date, which has characterised the causes and short-term outcomes in 1006 Africans with heart failure from 12 tertiary cardiology centres in nine countries in sub-Saharan Africa.9 The diagnosis of heart failure in THESUS-HF was based on the presence of dyspnoea associated with physical findings of congestive heart failure (ie, pedal oedema, raised jugular venous pressure, pulmonary congestion and/or tender hepatomegaly) necessitating admission to hospital in patients who were ≥12 years of age. Echocardiography was used to demonstrate cardiac dysfunction in all patients who were entered into the study. It is apparent from THESUS-HF that there are major differences between the epidemiology of acute decompensated heart failure in sub-Saharan Africa and that in North America/Europe (table 1). One of the most striking features is the relative youth of the African patients affected with acute heart failure (mean age, 52 years). In Western countries, acute decompensated heart failure is a disease of the elderly, with a mean age of 70–72 years.10 ,11 Acute heart failure therefore strikes African patients in the prime of their lives, with major economic implications because it affects the generation of breadwinners and care givers. As may be expected, the younger African patients with acute heart failure have a lower frequency of hypertension, ischaemic heart disease, diabetes mellitus, atrial fibrillation and renal insufficiency than older heart failure sufferers in developed countries (table 1).
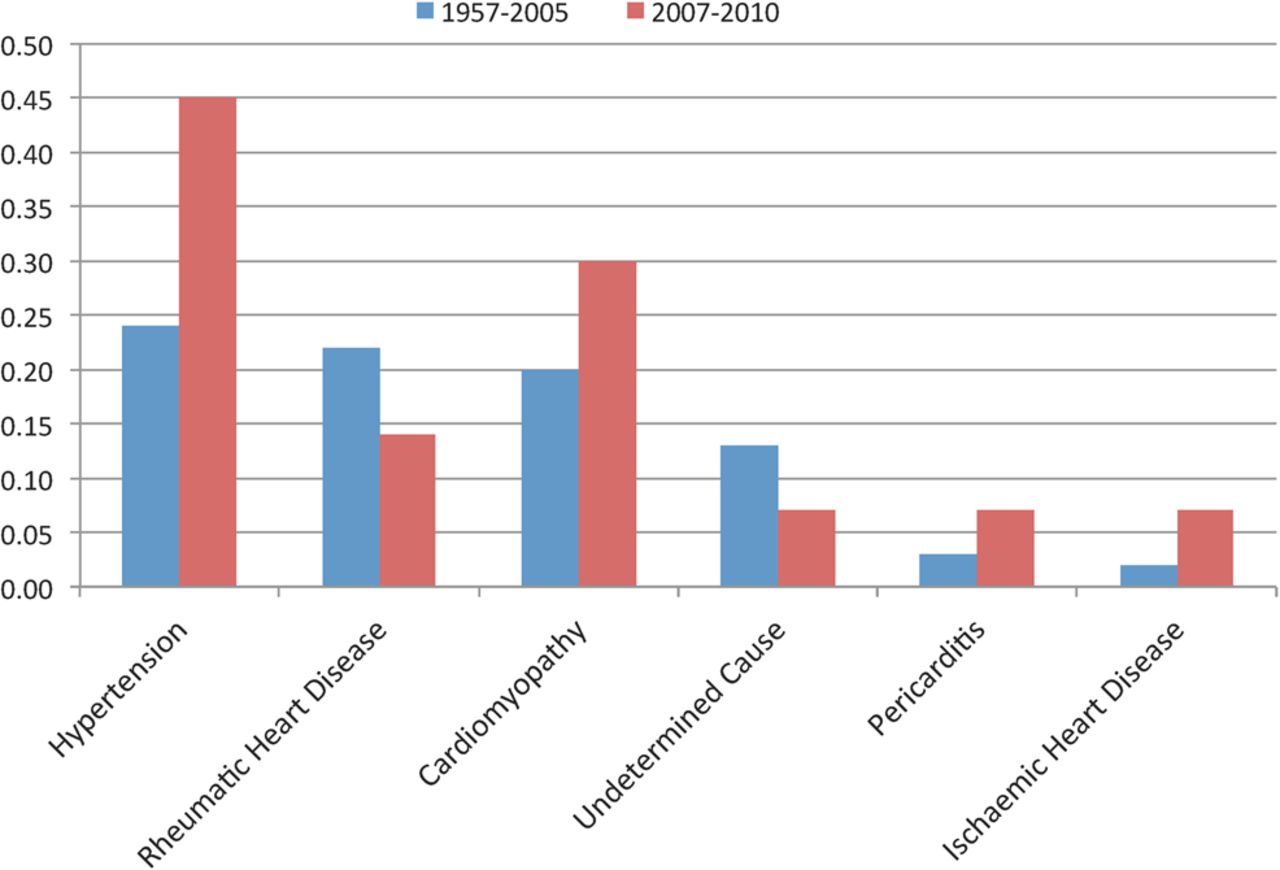
Compared with a summary of the causes of heart failure in sub-Saharan Africa based on the case series published between 1957 and 2005, THESUS-HF shows a changing trend in the epidemiology of acute heart failure in sub-Saharan Africa. This change is characterised by a rise in the contribution of hypertension as a cause of heart failure from 23% to 45%, a reduction in the role of rheumatic heart disease from 22% to 14%, and an apparently increasing recognition of ischaemic heart disease as a cause of heart failure from 2% to nearly 8% (figure 1). The high prevalence of hypertension and relatively low rate of coronary artery disease, which has also been observed in other single-centre studies,7 ,12 may be partly due to the largely non-invasive assessment of the aetiology of heart failure in THESUS-HF: many individuals with heart failure due to coronary artery disease (but without a clinical history of myocardial infarction or angina pectoris) may have been misclassified in terms of aetiology because of the known association of hypertension with coronary artery disease.1 The persistence of the low prevalence of coronary artery disease in African patients with heart failure has, however, been demonstrated in the Heart of Soweto Study, where <10% of cases of heart failure were attributed to coronary artery disease.13
{kind=link}
In Western series, men tend to be younger than women when admitted for the first time with heart failure, but because of greater female longevity, the number of male and female admissions is roughly equal.2 ,10 In contrast, men were significantly older than women on admission in THESUS-HF (54 vs 51 years, p=0.005). The African men also tended to have a significantly greater proportion of hypertension (60% vs 51%, p=0.004) and a greater propensity to smoke than women (17% vs 3%, p<0.001).9
Cardiomyopathy
Cardiomyopathy continues to be an important cause of heart failure contributing between 20% and 30% of cases of heart failure in adult Africans (figure 1).3 ,9 The major developments in the study of the epidemiology of cardiomyopathy in Africa have been the publication of a population-based survey of endomyocardial fibrosis (EMF) in Mozambique,14 the systematic ascertainment of the frequency of familial dilated cardiomyopathy (DCM) and peripartum cardiomyopathy (PPCM),15 and the identification of isolated left ventricular non-compaction (ILVNC) as a previously unrecognised cause of heart failure and stroke.16
Mocumbi et al14 have reported the first population-based study of the epidemiological features and early stages of EMF. They used transthoracic echocardiography to determine the prevalence of EMF in a random sample of 1063 subjects of all age groups from a rural area of Mozambique. Major and minor diagnostic criteria were defined, and a severity score was developed and applied. The estimated overall prevalence of EMF was 19.8%. The prevalence was highest among persons 10–19 years of age (28.1%) and was higher among male than among female subjects. The most common form was biventricular EMF (a prevalence of 55.5%), followed by right-sided EMF (a prevalence of 28.0%). Most affected subjects had mild-to-moderate structural and functional echocardiographic abnormalities. Only 48 people with EMF (22.7%) were symptomatic. The frequency of familial occurrence was high. These findings have laid the basis for the study of the pathogenesis of the disease and for the development of new management strategies.17
Studies from Europe and North America have long suggested that 20–50% of patients with DCM may have familial disease.18 There is little information on the frequency and clinical genetics of familial DCM in Africa. Ntusi et al15 were the first to determine the frequency and probable mode of inheritance of familial DCM in patients referred for investigation of the cause of DCM at a tertiary centre in Cape Town. They found that familial DCM affected at least a quarter of African patients with DCM, presented at a young age compared with idiopathic DCM (mean age of presentation 28 vs 39 years), was associated with PPCM in 7% of cases, and followed an autosomal dominant pattern of inheritance in the majority of families. These findings extend the recommendation for family screening for familial DCM in all cases of unexplained DCM, including patients with PPCM, to African patients with the disease.19
To the best of our knowledge, the first African case of ILVNC was reported in 2006.20 Over the ensuing 7 years, several cases were reported from Djibouti, South Africa and the Sudan.21–24 ILVNC is a cardiomyopathy caused by intrauterine failure of the myocardium to compact, and the common clinical complications are heart failure, arrhythmias and cardioembolism. Peters and colleagues have conducted a single-centre, prospective study in Johannesburg, in which subjects attending a dedicated cardiomyopathy clinic were screened for and diagnosed with ILVNC, provided they had no other associated structural heart disease and fulfilled all the accompanying echocardiographic criteria for diagnosis.25 Fifty-four subjects were identified (mean±SD age 45.4±13.1 years, 55.6% male and 63.0% in New York Health Association class II). The prevalence of ILVNC in their clinic was 6.9%. Heart failure associated with systolic dysfunction was the most common clinical presentation (53 subjects, 98.1%). Common sites of non-compaction were the apical (100%), mid-inferior (74.1%) and mid-lateral (64.8%) walls. Right ventricular non-compaction occurred in 12 subjects (22.2%). Pulmonary hypertension was documented in 45 cases (83.3%). Right ventricular dilation was present in 40 subjects (74.1%), while right ventricular function was depressed in 32 (59.3%). They concluded that the ILVNC in patients of African descent was characterised by biventricular abnormality and pulmonary hypertension, in addition to isolated left-sided abnormality.
What is new on the pathogenesis of heart failure and cardiomyopathy in Africans?
Heart failure
Recent research has highlighted the interaction between infectious diseases and heart failure in African patients.26 ,27 Infections play a primary aetiological role in many forms of heart failure that are endemic in sub-Saharan Africa, such as rheumatic heart disease, pericarditis and right heart failure. New research on the pathogenesis of rheumatic heart disease has shown that genetic risk factors contribute to 60% of the heritability of rheumatic fever.28 Pericarditis, which is due to tuberculosis in the majority of cases, is being increasingly recognised as an important cause of heart failure in sub-Saharan Africa (figure 1).9 ,29 There is intriguing evidence that, while HIV infection increases the burden of tuberculous pericarditis, the retrovirus reduces the risk of development of constrictive pericarditis in survivors of tuberculous pericarditis.30 Pulmonary tuberculosis and HIV infection are also recognised as important risk factors for right heart failure, which has been observed in 27% of Africans with heart failure.13 ,26 ,31 ,32
Cardiomyopathy
Research performed over the last decade has revealed novel molecular mechanisms of PPCM. Among these, elevated serum proinflammatory markers, such as sFas/Apo1, C-reactive protein, interferon γ and interleukin 6, point to proinflammatory processes involved in the induction and progression of PPCM and, possibly, impact on the prognosis.33 ,34 Work by Hilfiker-Kleiner et al35 points to a possible involvement of a pathophysiological circuit involving unbalanced oxidative stress and subsequent enhanced cleavage of the prolactin into an angiostatic and proapoptotic 16 kDa subfragment, which leads to endothelial damage and ventricular dysfunction. An important role of endothelial damage is further supported by the significantly elevated endothelial microparticles found in acute PPCM reflecting apoptosis with impaired microcirculation.36 Furthermore, angiogenic imbalance in PPCM which may not only depend on 16 kDa prolactin, but also on other factors such as soluble fms-like tyrosine kinase (sFlt-1).37 Finally, genetic factors may contribute to a higher susceptibility to PPCM in some of the patients with a positive familial history of cardiomyopathy who typically display a more severe course of disease.15 ,38 ,39
The studies of molecular genetics of DCM, hypertrophic cardiomyopathy (HCM) and arrhythmogenic right ventricular cardiomyopathy (ARVC) in Africans have continued apace over the past 5 years (table 2). The investigation of the genetic association of the β1- and α2c-adrenoreceptor variants and G308A polymorphism of the tumour necrosis factor α gene with idiopathic DCM and the mitochondrial DNA T16189C polymorphism with HIV-associated cardiomyopathy have proven to be negative in African patients.40–43 Previously, positive associations were noted with regard to the aldosterone synthase gene and improvement in left ventricular ejection fraction in DCM,44 and the mitochondrial DNA T16189C polymorphism and HLA variants in increasing the risk of DCM (table 2).45 ,46
Summary of molecular genetic studies in African patients with cardiomyopathy
There have been two key developments in the study of the molecular pathogenesis of HCM. The first development has been the identification of the polymorphisms in the ACE2 and angiotensin II type 2 receptor genes as modifiers of cardiac hypertrophy in patients with HCM (table 2).47 ,48 The second development has been new insights gained from studies of functional effects of genetic mutations that cause HCM in the South African founder families.49 ,50 Long-term follow-up of founder families with HCM (due to β myosin heavy chain (MYH7) R403W and troponin T (TNNT2) R92W mutations) showed that all carriers of the TNNT2 R92W mutation (who typically have no cardiac hypetrophy during their youth) developed hypertrophy after the age of 35 years, and the MYH7 R403W mutation is a strong predictor of the development of left ventricular dilation and systolic dysfunction in later life.51 In addition, TNNT2 and MYH7 mutations have distinct cardiac functional effects in HCM patients without hypertrophy.49 The distinct functional effect of the TNNT R92W mutation was a relative increase in systolic functional parameters, that of the MYH7 A797T mutation was reduced diastolic function, while the MYH7 R403W mutation reduced both systolic and diastolic function. Furthermore, an abnormal blood pressure response to exercise occurs more commonly in HCM patients with the TNNT2 R92W mutation than in those with MHY7 mutations.50 These observations may be relevant to the understanding of the high mortality associated with TNNT2 R92W mutation despite minimal evidence of cardiac hypetrophy.52
To the best of our knowledge, the first confirmed cases of ARVC from Africa were reported in 2000, and a kindred that is linked to the ARVC6 locus was subsequently reported in 2006.53 ,54 The ARVC Registry of South Africa has presented the first findings of the molecular genetics of ARVC on the African continent.55 Fifty unrelated cases of ARVC were enrolled between January 2004 and April 2009. The clinical presentation and proportion of mutations in the plakophylin-2 (PKP-2) gene (ie, 25%) were similar to those reported in other studies in Europe and North America. There was, however, the discovery of a founder effect involving a novel C1162T mutation in the PKP-2 gene in Afrikaner families.55
What is new on prognosis of heart failure and cardiomyopathy in Africans?
Heart failure
New information is emerging on the outcome of heart failure and cardiomyopathy in sub-Saharan Africa based mainly on the registries that have recently been established.9 ,55–57 The mortality in hospital (4%) and at 6 months (18%) after discharge for acute heart failure in THESUS-HF was similar to the outcome of participants in European and North American registries.10 ,11 ,58 This finding is remarkable because this almost identical outcome was observed despite major differences in patient characteristics (eg, a 20-year difference in age) and causes of heart failure (table 1), suggesting that once acute heart failure occurs, it may have a distinct course independent of patient characteristics and disease aetiology.9
Cardiomyopathy
Several studies of outcome in PPCM, DCM and ARVC have been carried out mainly in South Africa. Although patients with PPCM have a higher rate of spontaneous recovery of left ventricular function than patients with other forms of non-ischaemic cardiomyopathy,59 normalisation of left ventricular function at 6 months has been reported to occur in 23–54% of patients.57 ,60 Factors predicting poor outcome in African patients with PPCM are increased left ventricular systolic dimension, lower body mass index and low serum cholesterol at presentation, while older age and smaller left ventricular end systolic dimension appear to be independently associated with a higher chance of left ventricular recovery.61
A single-centre follow-up study of 80 patients with PPCM from Johannesburg reported a death rate of 28% at 2 years.57 The important finding of this study was the continued occurrence of deaths throughout the period of observation independently of HIV status, recovery of left ventricular systolic function, or subsequent pregnancy. Therefore, long-term monitoring is indicated in the management of women with PPCM. In addition, a proof-of-concept pilot study has provided preliminary evidence that bromocriptine may improve cardiac function and survival in patients with PPCM.62 There is a need for a full-scale trial that is adequately powered to study the effect on maternal mortality and childhood outcomes in the resource-poor environment of Africa.3
Ntusi et al56 have followed-up 120 patients with familial and idiopathic DCM over 14 years at a tertiary centre in Cape Town. A mortality of 10% per year occurred in both familial and idiopathic DCM. The presence of New York Heart Association functional class III and IV symptoms was an independent predictor of mortality, while heart transplantation was an independent predictor of survival. Digoxin use was a significant predictor of mortality in idiopathic DCM, which has reopened the controversy on the value of digoxin for heart failure.63
The national multicentre ARVC registry of South Africa reported an annual mortality of 2.8% and a 5-year cumulative mortality of 10%.55 Outcomes were worse than in other parts of the world; on average, patients died two decades earlier than patients in France.64 There are several explanations for this, the most likely of which was that implantable cardioverter defibrillators, which are life-saving for patients with ARVC, were underutilised in South Africa. Furthermore, there were significant delays in the referral of patients to centres with expertise to diagnose and manage this complex disease.65
What are the implications of the new information for the prevention and treatment of and research on heart failure and cardiomyopathy in Africa?
The remarkable progress that has been made over the past 5 years in the delineation of the epidemiology, pathogenesis and survival of patients with acute heart failure and cardiomyopathy in Africa provides a clear agenda for the prevention, treatment and research outlined in table 3. The adoption of the recommendations of the High-level United Nations Summit on cardiovascular disease and other non-communicable diseases by African countries is relevant to the control of heart failure.27 In addition, Mensah and Mayosi27 have argued that African governments need to address transmissible risk factors for non-communicable diseases (such as Mycobacterium tuberculosis, HIV and Group A β-haemolytic streptococcus) which are associated with endemic causes of heart failure such as pericarditis, cardiomyopathy and rheumatic heart disease in Africa. There is also a need to strengthen primary healthcare to facilitate the early detection and control of high blood pressure and other risk factors for heart failure and cardiomyopathy on the continent (table 3).
Priorities for prevention, treatment and research in the field of heart failure and cardiomyopathy in Africa
THESUS-HF has revealed suboptimal use of proven treatments for heart failure, such as β-blockers, which were only used in 50% of patients at 6 months of follow-up.9 The combination of a long-acting nitrate together with hydralazine, which is proven to be effective in African-Americans with heart failure, is hardly ever used in African patients.9 The quality of care for patients needs to be improved through systems that monitor adherence by physicians and patients to standard guidelines for management of patients with heart failure. Evaluation of patients with unexplained DCM and PPCM requires the examination of first-degree relatives for evidence of familial disease, based on the adaptation of guidelines and processes for clinical genetics to the resource-poor African environment.66
There are at least five areas that are ripe for further research on heart failure and cardiomyopathy. The first relates to clinical trials on the effectiveness of promising or controversial treatments for heart failure and cardiomyopathy such as the fixed-dose isosorbide dinitrate/hydralazine combination,67 digoxin,63 bromocriptine62 and pentoxifylline.68 A prospective, placebo-controlled, double-blind, randomised study to compare treatment with hydralazine/isosorbide dinitrate versus placebo on top of standard care in 500 African patients admitted with acute heart failure and left ventricular dysfunction (ie, Bi treatment with hydralazine/nitrates versus placebo in Africans admitted with acute HEart Failure (B-AHEF)) is underway. The second question relates to the emergence of coronary artery disease as a cause of heart failure in Africans. The studies performed to date have not used coronary angiography in a systematic fashion to assess the burden of ischaemic heart disease. Prospective studies that use a valid method for the detection of ischaemic heart disease are needed. Thirdly, the advent of high-throughput methods of genotyping provides the opportunity for detailed studies of the contribution of genetics to cardiomyopathy, and the determination of the cost-effectiveness of molecular genetic testing in the diagnosis and management of inherited cardiomyopathies in the African context.69
Finally, population-level studies of the incidence and prevalence of heart failure and cardiomyopathy need to be extended from EMF to other forms of cardiomyopathies and to the burden of heart failure in the community. These population-based surveillance studies will influence decisions on the allocation of resources for prevention and treatment, and the monitoring of progress after the deployment of control measures. This may be achieved by extending the studies of the epidemiology of blood pressure and vascular disease that have been initiated at several demographic surveillance systems, such as Agincourt and Hlabisa in South Africa.70 ,71
Conclusion
In summary, recent investigations performed in Africa or via collaborative efforts with investigators from around the world have provided several key insights into the epidemiology, pathogenesis and prognosis of acute heart failure and cardiomyopathy on the continent. First, the emergence of hypertension as the leading risk factor for heart failure highlights the need to place the treatment and control of hypertension in a central role for the global improvement of cardiovascular health.72 Second, the suboptimal use of effective treatments for heart failure, such as β-blockers, emphasises the need for physician education and introduction of measures to improve the quality of care. Third, the discovery of potential mechanistic pathways for cardiomyopathy is raising the promise of new interventions, such as the proposed role of bromocriptine in the treatment of PPCM.62 Finally, molecular and genetic studies of cardiomyopathy and population-based epidemiological surveys of heart failure represent the new frontier of cardiovascular research in Africa.
References
Footnotes
Bongani Mayosi is the Guest Editor of this Cardiology in Africa review series.
-
Contributors BMM conceived the idea of the manuscript. KS wrote the first draft. BMM revised the draft and prepared the final manuscript. Both KS and BMM approve the final manuscript that was submitted.
-
Competing interests KS receives support by unconditional research grants from the University of Cape Town, the University of the Witwatersrand, Servier, BHP Billiton, and the Medtronic Foundation. BMM is funded in part by the Lily and Ernst Hausmann Foundation, the South African Medical Research Council, and the National Research Foundation of South Africa.
-
Provenance and peer review Commissioned; externally peer reviewed.