Article Text

Abstract
Objective To assess allograft function over time after the Ross procedure.
Design Prospective multicentre registry.
Setting 10 cardiac surgery departments in Germany and the Netherlands.
Patients Among 1775 consecutive adult patients (mean age 43.7±12.0) who underwent the Ross procedure, 1645 (93%) received an allograft (pulmonary=1612, aortic=12, unknown=21), 120 (6%) a bioprosthesis, and 5 (0.3%) a bovine jugular vein for right ventricular outflow tract reconstruction.
Intervention Ross procedure.
Main outcome measures Using non-linear longitudinal models, serial echocardiographic records (N=6950) were studied to assess pulmonary conduit function over time in patients who had undergone the Ross procedure, with a maximum echocardiographic follow-up of 22.4 years (5.5±4.3 years).
Results A slight increase in pulmonary conduit regurgitation grade was observed during follow-up. Freedom from regurgitation grade ≥2+ was 95% after 14 years. Female patient gender, allograft use (compared to bioprosthesis), male donor gender, antibiotic treatment of the allograft, and specific surgical adjustments were associated with a significantly higher regurgitation grade. Mean conduit gradient increased from 4.7 mm Hg at 1 month to 10 mm Hg by 14 years, while peak gradient increased from 8.4 to 18.5 mm Hg. Smaller conduit diameter, male patient gender, younger patient age, younger donor age, and use of a bioprosthesis were associated with a significantly higher mean and peak gradient. During follow-up, 76 reinterventions were required on the pulmonary conduit in 67 patients. Freedom from pulmonary conduit reintervention or dysfunction was 90.6% (95% CI 87.7% to 93.6%) and 79.5% (95% CI 75.2% to 84.0%) at 15 years, respectively.
Conclusions Echocardiographic follow-up of pulmonary conduits shows good conduit durability. Clinically important conduit regurgitation and stenosis are rare in adult patients after the Ross operation.
- Cardiac Surgery
Statistics from Altmetric.com
Introduction
Although initially there was concern about the outcome of the Ross procedure, several short and mid term studies have proven that the procedure can be performed with low operative risk and with survival rates comparable to the general population.1–4 The need for specific surgical expertise to perform this complex operation and concerns about early and late failure led to its limited usage.3 With growing experience, however, the advantages of the Ross procedure have become more fully appreciated.
The long term fate of the pulmonary conduit is largely unknown but it is crucial for a more comprehensive judgment of this operation to be made. This is because this procedure results in the treatment of a single aortic valve disease with a two-valve procedure, subsequently placing two valves at risk of failure. In this regard, it is essential to understand how the pulmonary conduits in Ross patients function over time and to determine the factors associated with poor conduit performance. This knowledge can potentially lead to better patient management and improved outcomes in these young adult patients.
The durability of the pulmonary autograft depends on an appropriate surgical technique applied systematically and tailored to the individual patient.5–8 The long term durability of the reconstructed right ventricular outflow tract (RVOT) is predominantly related to non-surgical factors including degenerative processes.
The prevalence and predictors of late pulmonary conduit failure after the Ross procedure in adults have been addressed in only a few reports with small patient numbers.3 ,9–11 The natural dynamics of conduit stenosis and/or regurgitation are poorly understood. In the present multicentre study the availability of large numbers of patients and systematically collected echocardiographic records, and the use of sophisticated statistical methods, offer the unique opportunity to study extensively pulmonary conduit function over time in Ross patients and to explore potential risk factors associated with poor performance of the pulmonary conduits. Therefore, the objective of this study was to assess allograft function over time after the Ross procedure.
Methods
Study population
Data from 2038 patients who underwent a Ross procedure between November 1988 and September 2011 were collected and analysed from the German-Dutch Ross Registry database. All patients aged ≥16 years (n=1775) were entered into the study. Baseline characteristics are shown in table 1. The prospective registry was started in January 2002 and includes patient data from 10 cardiac surgery departments in Germany and the Netherlands. Institutional review board approval was obtained to conduct this prospective follow-up study in each participating centre (clinical trial ID NCT 00708409).
Baseline patient characteristics
Surgical technique
The surgical technique was determined by the surgeon responsible at each centre. Details of the operative technique have been described elsewhere.6 ,7 Perioperative and pulmonary conduit characteristics are shown in table 2. The presence of allograft sclerosis or fibrosis were determined by the tissue bank (pathology finding) during the harvesting and treatment of the homograft (the large majority) or as noted by the surgeon intraoperatively (minority). Of the implanted allografts, approximately 1.5% of fresh pulmonary allografts and approximately 15% of cryopreserved allografts received antibiotic treatment.
Perioperative characteristics
Although five percutaneous pulmonary valve implantations were performed during the follow-up of our patient population, the long term results of the Melody valve in adults are unknown at this moment and there is some reservation regarding the use of Melody valves in adults. Currently, we reserve the percutaneous pulmonary valve implantations for older and sick patients. For young adults, homograft is still the procedure of choice.
Clinical follow-up and echocardiographic data acquisition and measurements
Follow-up investigations were scheduled at discharge and on a yearly basis thereafter.
Conduit regurgitation was graded by mapping the dimensions of the regurgitation jet with pulsed and colour flow Doppler echocardiography, analogous to the semiquantitative method described by Perry and colleagues.12 The width of the proximal pulmonary regurgitation jet and the density and deceleration rate of the spectral Doppler flow signal were included in the assessment of regurgitation severity. This was graded from 0 to 4 (0 none, 1 mild, 2 moderate, 3 moderate-to-severe, 4 severe). Additionally, trace (trivial) insufficiency—defined as a very small regurgitation jet in early diastole near the detection limit—was included in the analyses as grade 0.5. Because of the low frequency of patients in grade 4 (n=7), this grade was combined with grade 3 and treated as one category. Because this is a multicentre study, the final decision regarding regurgitation grading was left to the attending echocardiographer. Maximum velocities across the pulmonary conduit were obtained by continuous Doppler in the basal short axis. Pressure gradients across the RVOT were calculated by the modified Bernoulli equation.
The prospective echocardiographic database was frozen on 1 November 2011, and echocardiographic data on all patients aged ≥16 years at the time of the Ross procedure were extracted (n=1775, mean age 43.7±12.0, range 16.1–70.5 years). Based on the distribution of the echocardiographic measurements, we could reliably assess overall temporal trend up to 14 years postoperatively.
For the analysis of ‘hard’ clinical end points (eg, death and reoperation), all consecutive patients were included in the study. However, there were also patients in whom no echocardiographic follow-up was available due to several reasons (eg, did not reach 12 months postoperative follow-up at the time the database was frozen). These patients were, therefore, not included in the echocardiographic analyses. For the echo analyses, only patients with at least one echocardiographic follow-up were included. A total of 6950 standardised echocardiographic measurements were analysed. The mean echocardiographic follow-up duration was 5.5 years (median 4.8 years, SD 4.25, range 0–22.4 years). At least one echocardiographic follow-up was obtained in 93.5% of patients (166 patients did not have any follow-up due to various reasons, eg, did not reach 12 months postoperative follow-up at the time the database was frozen, lost to follow-up).
The mean clinical follow-up duration was 7.2 years (median 6.7 years, SD 4.6, range 0–22.4 years).
Valve related events were defined according to the guidelines for reporting morbidity and mortality after cardiac valvular operations.13 Any degeneration of function not attributable to the valve leaflets (eg, the valve leaflets being intact) was considered as non-structural dysfunction (eg, regurgitation due to dilatation), whereas dysfunction due to leaflet degeneration was considered as structural valve failure (eg, retraction, calcification). Reconstruction was defined as the restoration of valve function without the exchange of the valve (or implantation of a new one)—that is, valve repair.
Statistical analyses
Simple descriptive statistics were used to summarise the data. Continuous variables are presented as mean±SD. Categorical data are described using frequencies and percentages. Parametric estimates of the postoperative echo derivatives are accompanied by an asymmetric 95% confidence interval (CI), comparable to ±2 SE. The CI is obtained by the bootstrap percentile method.14
Analyses of clinical data
Actuarial estimates of freedom from conduit reintervention and conduit failure were accomplished using Kaplan-Meier methods (SPSS V.11.0 for Windows, SPSS Inc, Chicago, Illinois, USA). The indications for reintervention were clinically overt right heart failure, medically intractable infective endocarditis, or maximal pressure gradients across the RVOT of one half of the systemic systolic pressure even in asymptomatic patients but with right ventricular hypertrophy and dilatation. Conduit dysfunction was defined as conduit reintervention, mean pressure gradient ≥25 mm Hg or regurgitation grade III or IV. This composite end point takes into consideration patients who have developed significant allograft dysfunction but for various reasons have not yet undergone reoperation by the database closure date. This end point better reflects the true incidence of significant and clinically relevant allograft dysfunction.
Analyses of echocardiographic data
Categorical echocardiographic measurement
To assess the temporal trend of likelihood of conduit regurgitation grades over time after surgery, follow-up transthoracic echocardiograms were analysed longitudinally for change in percentages of patients in each aortic regurgitation grade across time.
Continuous echocardiographic measurement
To assess the temporal trend of mean conduit gradient and peak conduit gradient over time after surgery, follow-up transthoracic echocardiographic measurements were analysed longitudinally for change in mean response across time.15 A non-linear longitudinal mixed model regression16 ,17 (SAS PROC NLMIXED) was used to analyse these continuous repeated measurements.
A focused unadjusted analysis (two separate analyses) was performed to assess the association between the postoperative mean and peak gradients, and pulmonary valve regurgitation. In the cumulative logistic mixed effects model for pulmonary valve regurgitation, we treated postoperative mean and peak gradients as the time varying covariates and assessed the effect of these gradients on the likelihood of higher pulmonary valve regurgitation grades.
Variable selection and risk factor analyses
Patient characteristics, conduit properties, and procedure related variables that are shown in tables 1 and 2 (and various transformations of these variables) were screened for association with postoperative conduit regurgitation, mean conduit gradient, and peak conduit gradient. In addition, year of surgery and recipient–donor blood group mismatch were also included in the model as a potential risk factor.
Variable selection utilised bootstrap bagging (bootstrap aggregation).16 ,18 The purpose behind the use of bootstrapping is simply to test the reliability of p values that are generated via statistical models. If bootstrap reliability of a variable is, for example, calculated as 30%, then—even though the p value is significant—it is judged to be significant in only ∼30% of datasets pertaining to the Ross operation. Our over-arching aim is to be as conservative as possible when reporting significant variables.
A detailed description of the statistical analyses can be found in the online supplementary appendix. All statistical tests with a p value of 0.05 or lower were considered significant. The longitudinal analyses of echocardiographic data were performed using SAS V.9.1 (SAS, Cary, North Carolina, USA).
Results
Reinterventions on the pulmonary conduit
During follow-up, 76 reinterventions (56 explants, 20 reconstructions) were required on the pulmonary conduit in 67 patients. Mean time to reintervention was 5.6±4.5 years (range 0.1–16.7 years). Structural valve failure was present in 53 reinterventions and non-structural failure in seven reinterventions. Pulmonary conduit endocarditis was present in 16 reinterventions.
Freedom from pulmonary conduit reintervention was 99.4% at 1 year (95% CI 99.1% to 99.8%), 94.7% at 10 years (95% CI 93.3% to 96.2%), and 90.6% at 15 years (95% CI 87.7% to 93.6%). Freedom from pulmonary conduit dysfunction (defined as conduit intervention or regurgitation >2 or mean gradient >25) was 98.5% at 1 year (95% CI 97.9% to 99.1%), 88.5% at 10 years (95% CI 86.4% to 90.6%), and 79.5% at 15 years (95% CI 75.2% to 84.0%).
With regard to allografts, during follow-up 63 reinterventions (48 explants, 15 reconstructions) were required on the pulmonary conduit in 54 patients. Mean time to reintervention was 6.9±4.5 years (range 0.04–16.3 years). Structural valve failure was present in 43 reinterventions and non-structural failure in six reinterventions. Pulmonary conduit endocarditis was present in 14 reinterventions. The mean time for endocarditis incidence was 6.3 years (SD 4.5, range 0.06–16.25). Freedom from pulmonary conduit reintervention was 99.5% at 1 year (95% CI 99.2% to 99.9%), 95.5% at 10 years (95% CI 94.1% to 97.0%), and 91.4% at 15 years (95% CI 88.5% to 94.3%). Freedom from pulmonary conduit failure was 98.4% at 1 year (95% CI 97.8% to 99.0%), 88.4% at 10 years (95% CI 86.4% to 90.5%), and 78.1% at 15 years (95% CI 74.6% to 83.1%).
With regard to bioprostheses, during follow-up 13 reinterventions (eight explants, five reconstructions/dilatation) were required on the pulmonary conduit in 13 patients. Mean time to reintervention was 1.8±0.9 years (range 0.17–3.4 years). Structural valve failure was present in 10 reinterventions and non-structural failure in one reintervention. Pulmonary conduit endocarditis was present in two reinterventions. In patients with bioprostheses freedom from reintervention was 98.2% at 1 year (95% CI 95.8% to 100.0%) and 85.4% at 10 years (95% CI 78.0% to 93.6%). Freedom from dysfunction was 91.4% at 1 year (95% CI 86.8% to 96.2%) and 66.8% at 5 years (95% CI 55.3 to 80.6).
The clinical outcomes of these patients and reinterventions have been extensively presented in previous publications of the Registry.19–24
Pulmonary conduit regurgitation over time
The percentage of patients in each grade of pulmonary conduit regurgitation changed significantly over time (p=0.003). During follow-up, the percentage of patients with pulmonary conduit regurgitation grade 0 or trace decreased from about 88% at 1 month to about 66% by 14 years after the procedure. The percentage of patients with grade 1+ increased from about 11% to about 29% during the same time period. The percentage of patients with grade 2+ or higher increased from about 1.1% to about 4.7% during the same time period.
The temporal trend of pulmonary regurgitation over time is non-linear. There is an early hazard phase evident within the initial 2 years; beyond that, the risk is relatively constant and low (figure 1A).
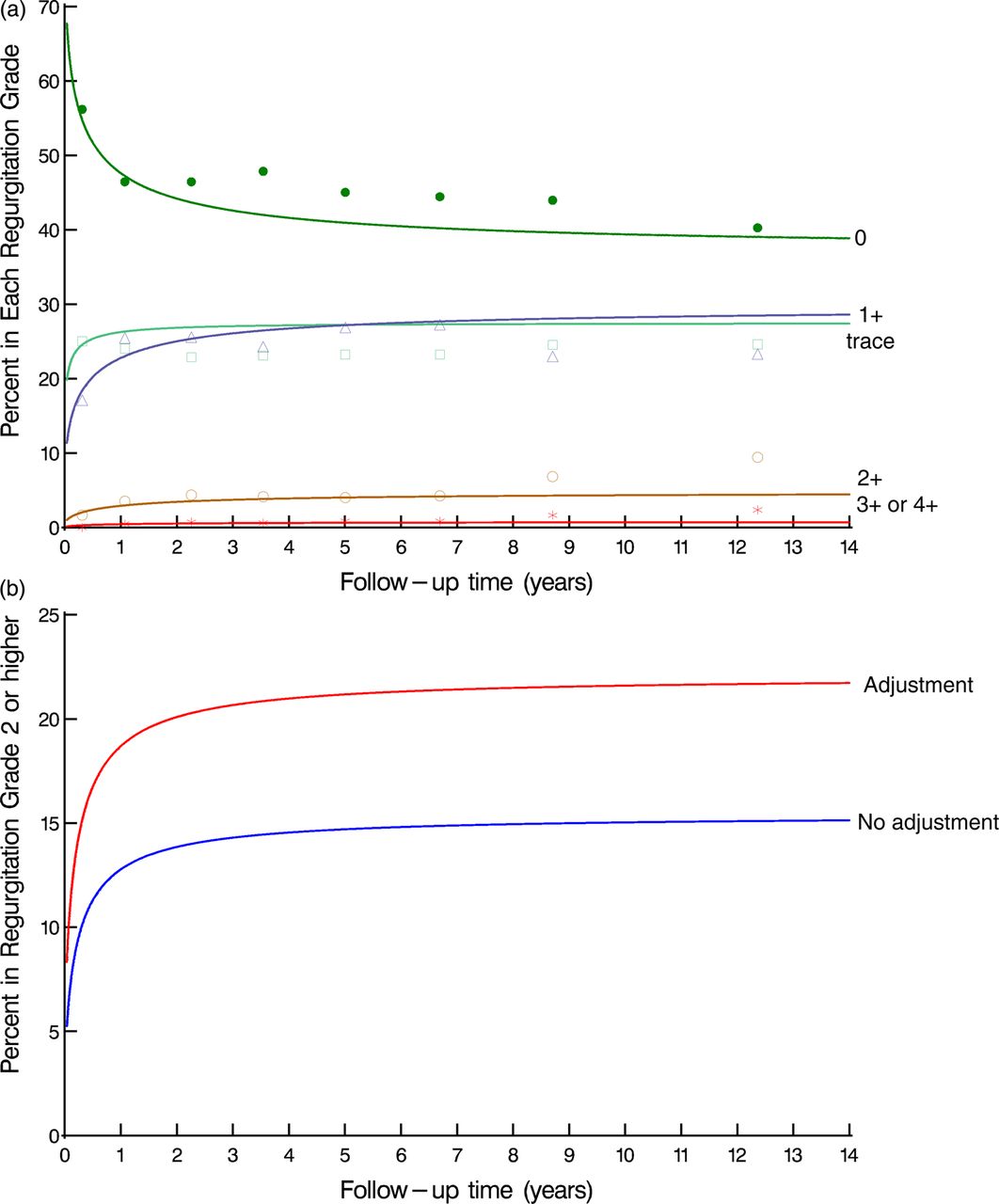
(A) Temporal trend of pulmonary regurgitation grade after the Ross procedure. Solid lines represent percentage of patients (mean effect) in each grade at various time points. Symbols represent crude estimates of grouped raw data without regard to repeated measures and are presented here just to verify the model fitting. (B) Predicted percentages of patients in regurgitation grade 2 or higher stratified by specific surgical adjustments of the allograft. The nomogram was solved for patients with a high risk profile with the following values for variables in the model: type of prosthesis=allograft; antibiotic treatment of the allograft=yes; female donor gender; female recipient gender; absence of sclerosis or fibrosis; absence of fenestrations. Access the article online to view this figure in colour.
The risk factors associated with a greater risk of higher pulmonary conduit regurgitation grade are shown in table 3. Overall, female patient gender was associated with a significantly greater risk of higher pulmonary conduit regurgitation grade compared to males (p<0.001). Furthermore, with respect to allograft properties, antibiotic treatment of the allograft (p<0.001) and male donor gender (p=0.032) were associated with a higher risk of higher pulmonary conduit regurgitation grade. In addition, the use of an allograft (as compared to a bioprosthesis) was correlated with a significantly higher grade of pulmonary conduit regurgitation grade during follow-up of Ross patients (p<0.001). Specific surgical adjustments of the allograft (resection of the allograft's subvalvular muscle with or without replacement with a stripe of pericardium, GoreTex membrane, or Dacron prosthesis) were associated with a significantly higher regurgitation grade (p<0.001) (figure 1B).
Risk factors associated with increased likelihood of higher conduit regurgitation grade and increased mean/peak conduit gradient
The presence of allograft sclerosis or fibrosis appeared to be associated with a lower pulmonary conduit regurgitation grade (p<0.001). However, this effect was only significant in the first 2 years after the Ross operation. The presence of allograft fenestration, on the other hand, was only significantly associated (p=0.012) with a lower regurgitation grade late in the follow-up (>2 years after surgery).
Pulmonary conduit obstruction over time
Mean pulmonary conduit gradient
Mean pulmonary conduit gradient increased from about 4.7 mm Hg at 1 month to about 10 mm Hg by 14 years after the procedure (figure 2A). The change in mean gradient was mainly observed in the first 2 years after surgery. The increase was statistically significant (p<0.001).
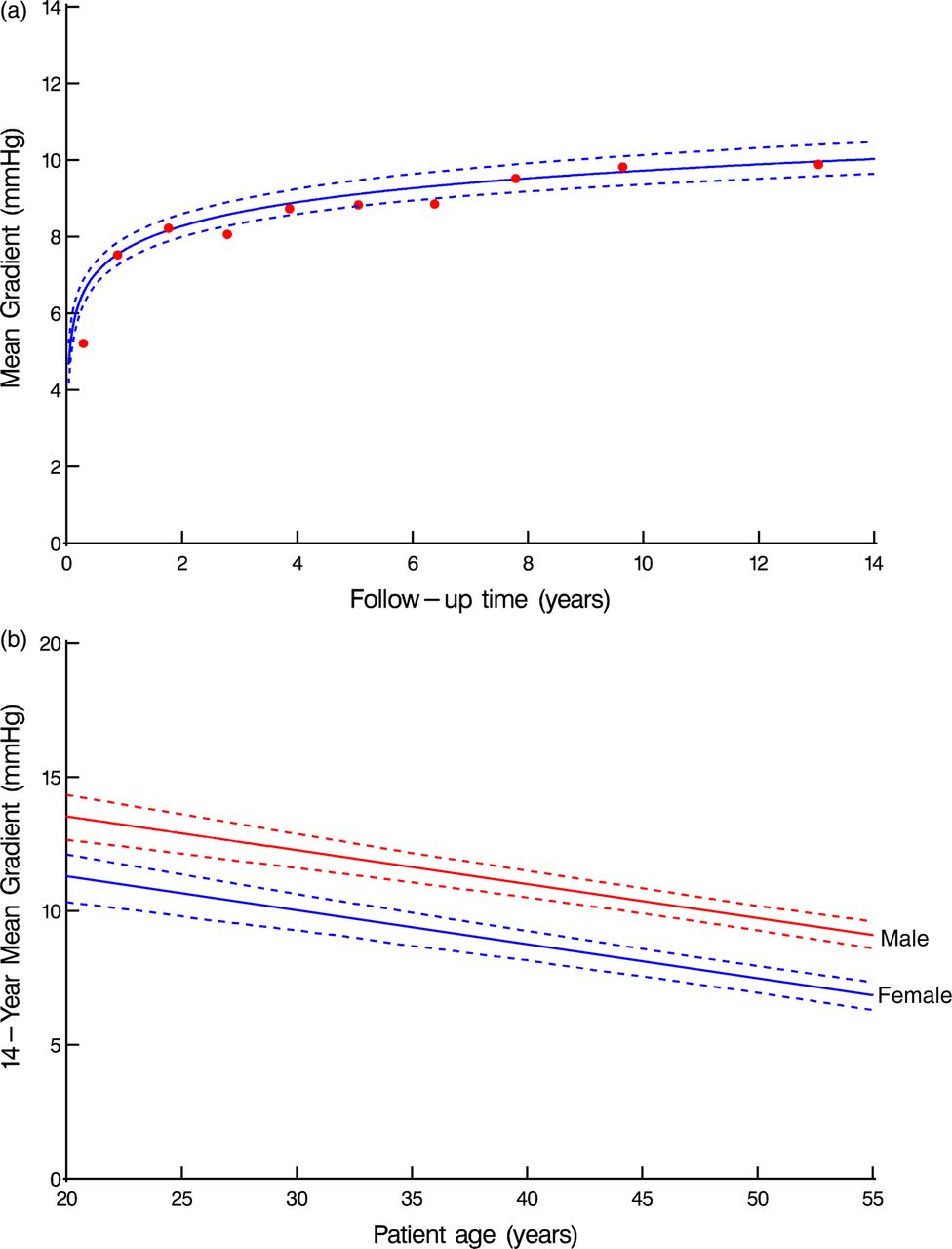
(A) Solid lines are parametric estimates of mean gradient from non-linear longitudinal mixed model and are enclosed within dashed 95% bootstrap percentile confidence bands, equivalent to 2 SD. Symbols represent crude estimates of grouped raw data without regard to repeated measures and are presented here just to verify the model fitting. (B) Fourteen year predicted mean gradient by age, stratified by gender. The nomogram was solved for the following values for variables in the model: type of prosthesis=allograft; mean conduit diameter (25 mm); mean donor age (47 years). Access the article online to view this figure in colour.
Both younger age of the recipient (p<0.001) and younger age of the allograft donor (p=0.012) were associated with a significantly higher mean pulmonary conduit gradient. Male patient gender (p<0.001) (figure 2B) and the use of smaller conduit diameters (p<0.001) were correlated with a higher mean pulmonary conduit gradient. Furthermore, the use of a bioprosthesis (as compared to an allograft) (p<0.001) appeared to be associated with higher pulmonary conduit gradient.
Donor gender, allograft quality (presence of fenestrations, sclerosis or fibrosis), allograft adjustments by surgical means (yes vs no, different surgical techniques), allograft length (distance between pulmonary artery bifurcation resection line and sinutubular junction of the pulmonary valve ≤20 mm (short) or >20 mm (long)), allograft diameter (absolute value), year of surgery, and recipient–donor blood group mismatch had no substantial effect on the annual progression of the mean pulmonary conduit gradient.
The focused unadjusted analysis to assess the association between mean gradient and PVR during follow-up showed that early postoperative mean gradient does not have any impact (p=0.1) on the early return of PVR. However, higher postoperative mean gradient is associated with an increased likelihood of higher grade of late PVR (p<0.0001).
Peak pulmonary conduit gradient
Peak pulmonary conduit gradient appears to be slightly increased from about 8.4 mm Hg at 1 month to about 18.5 mm Hg by 14 years after the procedure (figures 3A). The increase was statistically significant (p<0.001) and was mainly observed in the first 2 years after surgery.

{kind=link}
{kind=link}
{kind=link}
(A) Solid lines are parametric estimates of peak gradient from non-linear longitudinal mixed model and are enclosed within dashed 95% bootstrap percentile confidence bands, equivalent to 2 SD. Symbols represent crude estimates of grouped raw data without regard to repeated measures and are presented here just to verify the model fitting. (B) Fourteen year predicted peak gradient by age, stratified by type of prosthesis used. The nomogram was solved for the following values for variables in the model: mean conduit diameter (25 mm); continuous proximal suture line; allograft harvested from non-heart beating donor; male patient gender; mean donor age (47 years). Access the article online to view this figure in colour.
As with the mean pulmonary conduit gradient, younger age of the recipient (p<0.001) (figure 3B) and the use of bioprosthesis (as compared to allograft) (p<0.001) (figure 3B) were associated with a significantly higher peak pulmonary conduit gradient after 14 years of follow-up. Figure 3B shows on the x-axis that younger patient age (for both allograft and bioprosthesis recipients) is correlated with a higher peak conduit gradient after 14 years of follow-up (shown on the y-axis). The older the patient at the time of the procedure, the lower the peak gradient is after 14 years of follow-up. In addition, this figure also shows that although younger patient age is correlated with higher peak conduit gradient after 14 years of follow-up, the use of a bioprosthesis is correlated with a higher gradient compared to the use of allografts, independent of how old the patient is at the time of the procedure (shown by the two stratified lines in the figure).
Younger age of the allograft donor (p=0.012), male patient gender (p<0.001), and smaller conduit diameter were associated with a significantly higher peak pulmonary conduit gradient (p<0.001). In addition, it appears that the use of an interrupted suture line (as compared to continuous) (p=0.017), allografts harvested from non-heart beating donors (p=0.024), and a recent date of surgery (p=0.039) were also associated with a higher peak gradient after RVOT reconstruction with a conduit.
Donor gender, allograft quality, allograft adjustments by surgical means, allograft length, and recipient–donor blood group mismatch had no substantial effect on the annual progression of the peak pulmonary conduit gradient.
The focused unadjusted analysis to assess the association between peak gradient and PVR during follow-up showed that early postoperative peak gradient does not have any impact (p=0.1) on the early return of PVR. However, higher postoperative peak gradient is associated with an increased likelihood of a higher grade of late PVR (p<0.0001).
Discussion
The results of the present study show that both pulmonary conduit pressure gradient and pulmonary conduit regurgitation grade increases predominantly within the first two postoperative years. Clinically important pulmonary conduit regurgitation is rare in adult patients after the Ross procedure, with the number of patients with clinically significant pulmonary conduit regurgitation being <5% after 14 years of follow-up. In addition, conduit obstruction of potential clinical impact occurs in a minority of patients (3.2%). Furthermore, in the present study we were able to identify several patient, donor, and procedure related factors influencing the pulmonary conduit function during the follow-up of the Ross patients.
The use of allografts in the reconstruction of the RVOT is widely accepted and this conduit is considered as the ‘gold standard’ in patients undergoing the Ross operation. However, the limited availability and the high costs involved in the preparation and storage of these valves have led to the use of bioprostheses as a suitable alternatives. Some studies investigating hard clinical end points showed comparable intermediate results between allografts and bioprostheses,25 ,26 while others reported a significantly higher risk of reintervention with bioprosthetic valves as compared to allografts.27 The results of the present study show that the use of bioprosthetic valves is correlated with significantly higher mean and peak gradients as compared to allografts. Patients with an allograft, on the other hand, had a significantly greater risk of higher regurgitation grade as compared to patients with bioprosthetic valves. The difference in regurgitation grade and gradient between allografts and bioprosthetic valves occurred mainly in the first 2 years after surgery and remained constant after this period.
An allograft related factor that has been found to play a role in the chronic degeneration process of the allograft is younger donor age.9 ,10 ,28 We observed a clear age dependent association between donor age and mean/peak allograft gradient: the younger the donor allograft, the higher the allograft mean and peak gradient. This is in accordance with communications in the literature which report on the entire age range from infants to adults.29 In most studies, younger donor age is also related to a smaller allograft diameter. The present report includes only young adult and adult patients, thus the issue of age related small allografts in children and adolescents does not play any role. It may be speculated that this age dependency is related to the amount of viable cells with pronounced immunogenic properties.29
The effect of conduit diameter on valve failure has been extensively studied, but no generally accepted consensus has been reached.30 ,31 Previous reports have shown that smaller conduit diameter is associated with limited longevity, while others have not found any relation between absolute allograft diameter and its longevity.32–34 In the present study, smaller conduit diameter was correlated with a significantly increased risk of higher mean and peak conduit gradient over time. We can only speculate that with larger implanted allografts, the expected shrinkage process induced by immunologically active material is less obstructive since a diameter reserve works protective. The length of the allograft had no effect on the changes of the pressure gradient or allograft regurgitation grade. This is in contrast to other studies which stressed the occurrence of an extensive fibroproliferative process with consecutive compression and/or shrinkage of the tubular part of the allograft as a major mechanism of deteriorating graft haemodynamics.11
Shrinkage of the allograft was pronounced in the proximal annulus area,35 suggesting that implantation of a glutaraldehyde fixed pericardial strip after donor muscle resection might reduce allograft annulus shrinkage with a haemodynamic benefit. In the present study allograft adjustments resulted in a significantly greater risk of higher allograft regurgitation grade compared to the allografts without any surgical adjustment interventions. Allograft adjustments were not correlated at all with allograft stenosis. Since no large scale reports on allograft adjustments to prevent the occurrence of allograft shrinkage are available, long term echocardiographic follow-up studies are necessary to confirm the modelled results.
A more recent year of operation correlated with a significantly higher peak conduit gradient. This finding has also been previously reported.28 Although patient gender and antibiotic treatment of the allografts were also found to be significantly associated with allograft function over time, the clinical relevance of these factors is negligible since the difference in mean gradient between male and female patients was ±2 mm Hg.
There is uncertainty about the role of blood group compatibility in relation to accelerated allograft failure. While some investigators have suggested that blood group incompatible allografts have a significantly higher early reoperation rate compared to blood group compatible allografts,36 other investigators were not able to find any association at all.37–39 In the present study, we were not able to identify any correlation between recipient–donor blood group mismatch and allograft function over time.
Clinical implications
Thus far the number of reinterventions on the pulmonary conduits for haemodynamic deterioration is low, although a considerable number of conduit failures were due to infective endocarditis. Strict adherence to endocarditis prophylaxis guidelines and high clinical suspicion to detect and diagnose non-fulminant allograft endocarditis may decrease the incidence of endocarditis and further improve the postoperative outcomes. Our echocardiographic analyses showed that a small but not negligible subset of patients is at risk for progressive valve failure. Thus, not only overt failures (with the need for reoperation) have to be reported, but also the number of conduits at risk with an expected high failure rate in the longer term need reporting. An almost linear increase of the mean transvalvular gradient occurred within the first 2 years and flattened out in a steady state afterwards. In contrast, a small gradual increase in conduit regurgitation over time is detectable, but the progression rate is sustained and clinically insubstantial. Using non-linear longitudinal models, we were able to define several patient and conduit related factors that are associated with increased dysfunction and/or progression of conduit dysfunction over time. These insights may be helpful in applying the optimal surgical technique (conduit type, suturing, donor/patient characteristics mismatch, sizing, and surgical adjustments) and to monitor patients more adequately who present with an increased risk of allograft failure.
We find that the pulmonary allograft, together with consideration of allograft related risk factors, constitutes the most appropriate valve substitute in the setting of the Ross operation, although it is challenging to take into account risk related allograft factors given the limited availability of pulmonary allografts. Alternative valve substitutes depict no optimal RVOT substitute so far, due to the lack of scientific evaluation with respect to large patient cohorts and mid term or even long term observations.
Study strengths and limitations
Some reports on institutional experiences tried to define prognostic factors for pulmonary conduit dysfunction in the mid term. These reports have included relatively low numbers of patients, they mainly focused on the development of allograft stenosis, the follow-up time was limited, and serial longitudinal analysis of haemodynamic conduit function over time was not considered.
One of the major strengths of the present study is the systematic echocardiographic follow-up of a large group of Ross patients. In addition, the surgical procedure was performed in 10 cardiac surgery departments in Germany and the Netherlands which increases the generalisability of the results presented. Furthermore, using longitudinal methods in the present study, we were able to explicitly model the temporal trend of the echocardiographic measurements. Using this method we were able to visualise the temporal trend of each conduit regurgitation grade over time during follow-up, which enabled the clinicians to determine how conduit regurgitation on average developed over time after valve implantation. These methods are superior to dichotomising outcomes and analysing them with actuarial methods as if they were events, such as freedom from grade 1+ or 3+ conduit regurgitation after valve surgery, where only a snapshot image of valve function is expressed.40–42 Modelling of the temporal trend and identifying factors that influence this temporal trend can be of particular importance since it can help clinicians understand how a certain process changes over time and thus can contribute to better patient management (eg, by determining which patients should be monitored more closely by their physicians and at which time interval).
The current study presents several limitations. The echocardiographic examinations were not reviewed independently or blindly. However, the echocardiographic examination protocol was standardised, and forms designed specifically for this registry were completed at each examination. The echocardiographic examination data were, therefore, collected prospectively. The mean echocardiographic follow-up time is 5.5±4.2 years. Furthermore, a slow-going haemodynamic deterioration of the RVOT conduit is well compensated clinically for a long time. Therefore, long term studies are necessary. As with all multicentre echocardiographic follow-up studies, a bias cannot be excluded and may have influenced the results. The lack of an echo core laboratory is an additional potential weakness of the present study. Finally, the applied longitudinal statistical methods are relatively new and therefore there is no widespread general knowledge about their use.
Conclusion
Echocardiographic follow-up of pulmonary conduits shows good conduit durability. Clinically important pulmonary conduit regurgitation is rare in adult patients after the Ross procedure. Conduit obstruction with a potential clinical impact occurs in a minority of patients. While conduit pressure gradient development occurs predominantly during the first 2 years postoperatively, conduit regurgitation increases gradually over time yet is clinically insignificant on average. Consideration of risk associated predictors may improve both conduit and patient outcome.
Key messages
-
What is already known on this subject?
-
Although initially there was concern about the outcome of the Ross procedure, several short and mid term studies have proven that the procedure can be performed with low operative risk and survival rates comparable to the general population. The need for specific surgical expertise to perform this complex operation and concerns about early and late failure led to its limited usage. With growing experience, however, the advantages of the Ross procedure have become more fully appreciated.
-
How might this impact on clinical practice?
-
The long term fate of the pulmonary conduit is largely unknown, but it is crucial for a more comprehensive judgment of this operation since this procedure results in the treatment of a single aortic valve disease with a two-valve procedure, subsequently placing two valves at risk of failure. In this regard, it is crucial to understand how the pulmonary conduits in Ross patients function over time and to determine the factors associated with poor conduit performance.
-
What this study adds?
-
This knowledge can potentially lead to better patient management and improved outcomes in these young adult patients.
Acknowledgments
We thank Mrs Katrin Meyer for her excellent data management and secretarial support at the Registry Site in the Department of Cardiac and Thoracic Vascular Surgery, University of Lübeck, Germany.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix-Centers
- Data supplement 2 - Online appendix-statistical
Footnotes
-
Contributors MMM: conception, design, analysis, interpretation of data, and drafting the article. EIC: conception, design, interpretation of data, drafting the article, final approval of the version to be published. US, AdJJCB and H-HS: conception, design, final approval of the version to be published. JR and EHB: analysis and final approval of the version to be published. JJMT conception, design, interpretation of data, final approval of the version to be published.
-
Funding MMM is funded by a Mosaic grant of the Netherlands Organisation for Scientific Research (NWO 017.006.058).
-
Competing interests None.
-
Ethics approval Institutional review board approval was obtained to conduct this prospective follow-up study in each participating centre (clinical trial ID NCT 00708409).
-
Provenance and peer review Not commissioned; externally peer reviewed.