Article Text

Statistics from Altmetric.com
Introduction
Everolimus-eluting bioresorbable vascular scaffold (BVS) was recently approved by the US Food and Drug Administration for the treatment of coronary artery disease (CAD). It provides initial support for the vessel then disintegrates overtime until it is completely resorbed, potentially overcoming the late adverse events with permanent metallic stents. BVS was associated with improved vascular response by helping restore vasomotion and adaptive remodelling,1–3 plaque regression, late lumen enlargement and restoration of endothelium-dependent vasodilation up to 5 years.4–6
Several randomised controlled trials (RCTs) compared BVS with second-generation drug-eluting stents (DES) and reported similar outcomes at 1 year.7–10 Multiple meta-analyses compared both devices and showed increased myocardial infarction (MI) and stent thrombosis (ST) with BVS compared with DES at 1 year.11–15 The BVS design aimed at more favourable long-term profile; however, long-term clinical outcomes of this device compared with DES are scarce. Given this limitation, we aim to perform the first meta-analysis to examine the 2-year clinical outcomes of BVS compared with second-generation DES across the spectrum of patients with CAD.
Methods
Data sources and study selection
The published strengthening Meta-analysis of Observational Studies in Epidemiology checklist was implemented to select the studies for this review.16 We also used the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) guidelines for reporting systematic reviews and meta-analyses.17 A comprehensive search of the online databases including PubMed, Cochrane CENTRAL, EMBASE, EBSCO, Web of Science and CINAHL databases was performed up until October 2016 for English language peer-reviewed studies comparing BVS with second generation DES. We used the following keywords in separate and in combination: ‘bioresorbable’, ‘scaffold’, ‘PCI’, ‘“drug eluting stents’, ‘BVS’, ‘ABSORB’ and ‘long term’. We screened studies' abstracts for established inclusion/exclusion criteria and studies that were relevant to our search were downloaded and full manuscripts were reviewed. We also scanned through references from relevant articles for additional studies not identified from the initial database search. Given the scarcity of data, both randomised trials and observational studies were eligible for inclusion. Major conferences were examined for abstract presentations from RCTs. Studies using only second-generation DES and reporting outcomes at follow-up of 2 years were included. Figure 1 illustrates the search strategy.

Search strategy and study selection as per Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow diagram.
Outcomes and definitions
Our primary outcome of interest was device-oriented composite events (DOCE), also known as target lesion failure, which was defined in the included studies as the composite of cardiac death, target vessel myocardial infarction (TV-MI) and ischaemia-driven target lesion revascularisation (TLR). Secondary outcomes included all-cause mortality, cardiac mortality, definite ST, definite/probable ST, very late ST (>1 year) and TLR. Outcomes were reported at 2 years of follow-up.
Data extraction and quality assessment
Data were independently extracted from the relevant articles by two physician reviewers (RN and MS) after determining their eligibility for inclusion. Discrepancies and disagreements regarding data incorporation were resolved through consensus among all authors. The baseline demographic characteristics of study participants (ie, sample size, age, gender, intervention in the study/control group) were collected from each eligible study as available. The number of events for clinical outcomes in each arm was tabulated. We assessed the quality and risk of bias in reporting data for individual studies objectively by using the methods specified in the Cochrane Handbook of Systematic Reviews and the New Castle-Ottawa scale for case–control studies and summarised in online supplementary table S1.18 ,19 Publication bias was assessed using funnel plots and egger test.
supplementary tables
Data synthesis and analysis
We reported clinical outcomes and their respective effect size in all of the included studies by using ORs, with the corresponding 95% CIs. Heterogeneity testing was performed by using the Cochran Q test and Higgins I2 test. To calculate a summary estimate across all included studies, we used random effects models (DerSimonian and Laird) to mitigate any heterogeneity. Fixed effects model performed as well for all outcomes of interest and reported as supplementary figure 1. A Cochran's Q p<0.10 and I2>50% were considered to be indicative of significant heterogeneity. All the p values were two-tailed with statistical significance level at 0.05. We calculated absolute risk reduction (ARI) as BVS event rate minus DES event rate. Relative risk reduction (RRI) was calculated as ARI divided by DES event rate. Number needed to harm (NNH) was calculated as 1 divided by ARI. All analyses were conducted by using RevMan V.5.2.4 software (Nordic Cochrane Centre, Cochrane Collaboration, 2013) (The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan) [Computer program]. Version 5.2; Copenhagen, 2012).
supplementary figure
Results
Our initial search yielded 473 studies for possible inclusion in this analysis. After rigorous examination, only five studies reported outcomes with 2 years of follow-up were identified,20–24 three were RCTs and two were observational multicentre multinational propensity score-matched analyses (figure 1). All studies included were of high quality and low risk of bias (see online supplementary tables S2 and S3). A total of 2360 patients who underwent PCI with BVS (n=1322) versus second-generation DES (n=1038) were available for analysis. PCI was done for stable angina or silent ischaemia in 36% of total patients, more in the BVS group compared with the DES group (42%, 558/1322 vs 28%, 291/1038, p<0.001). Patients with ST-segment elevation myocardial infarction (STEMI) represented almost 33% of total patients, significantly less in the BVS arm compared with DES (30%, 395/1322 vs 37%, 387/1038, p<0.001). Balloon predilatation was performed in 97% of the BVS group compared with 80% of the DES group (p<0.0001), while balloon postdilatation was performed in 60% of the BVS group compared with 46% of the DES group (p<0.001). Characteristics of the included studies as well as patients and procedural characteristics were summarised in tables 1 and 2.
Patient and procedural characteristics of the included studies
Characteristics of included studies
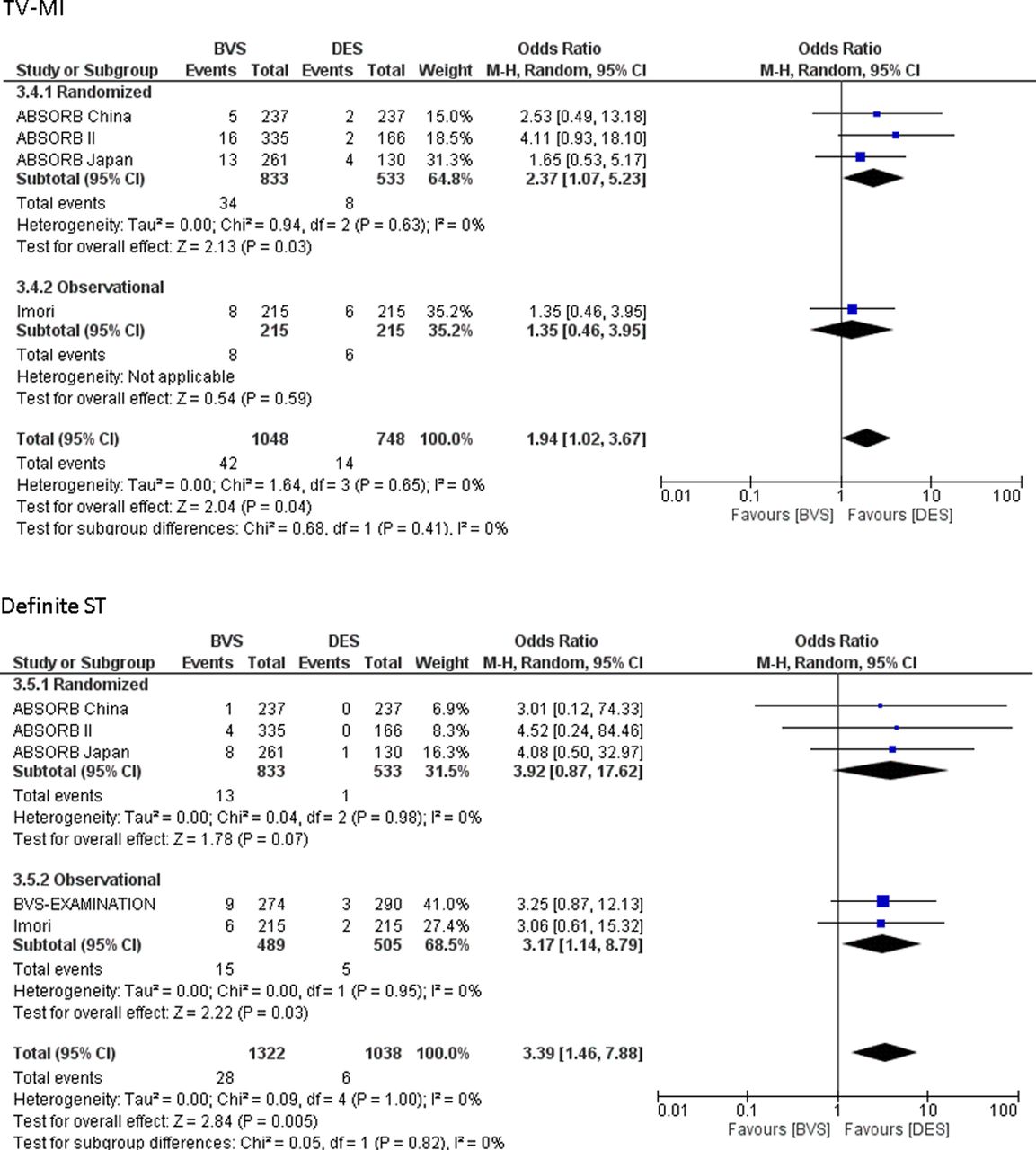
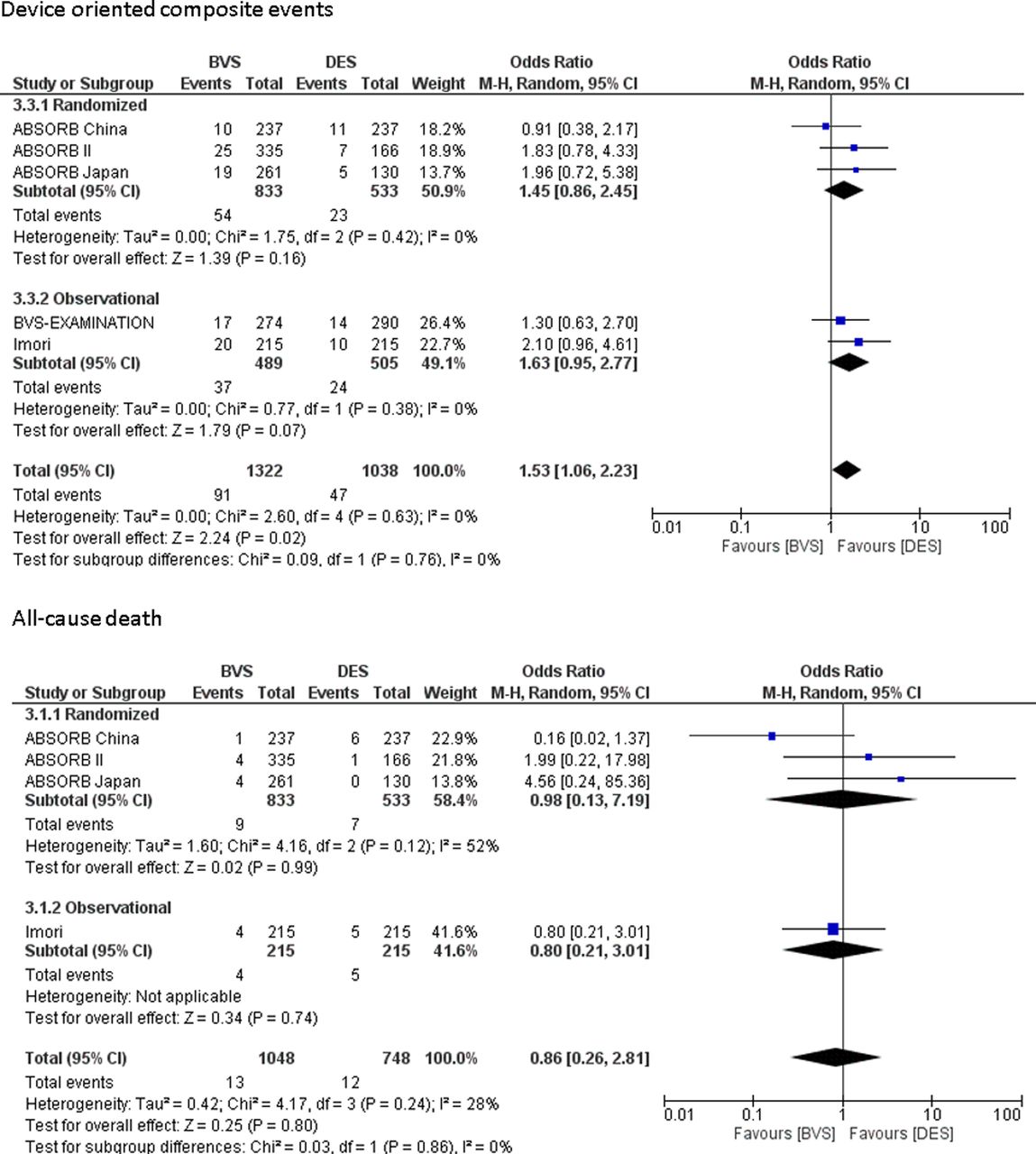
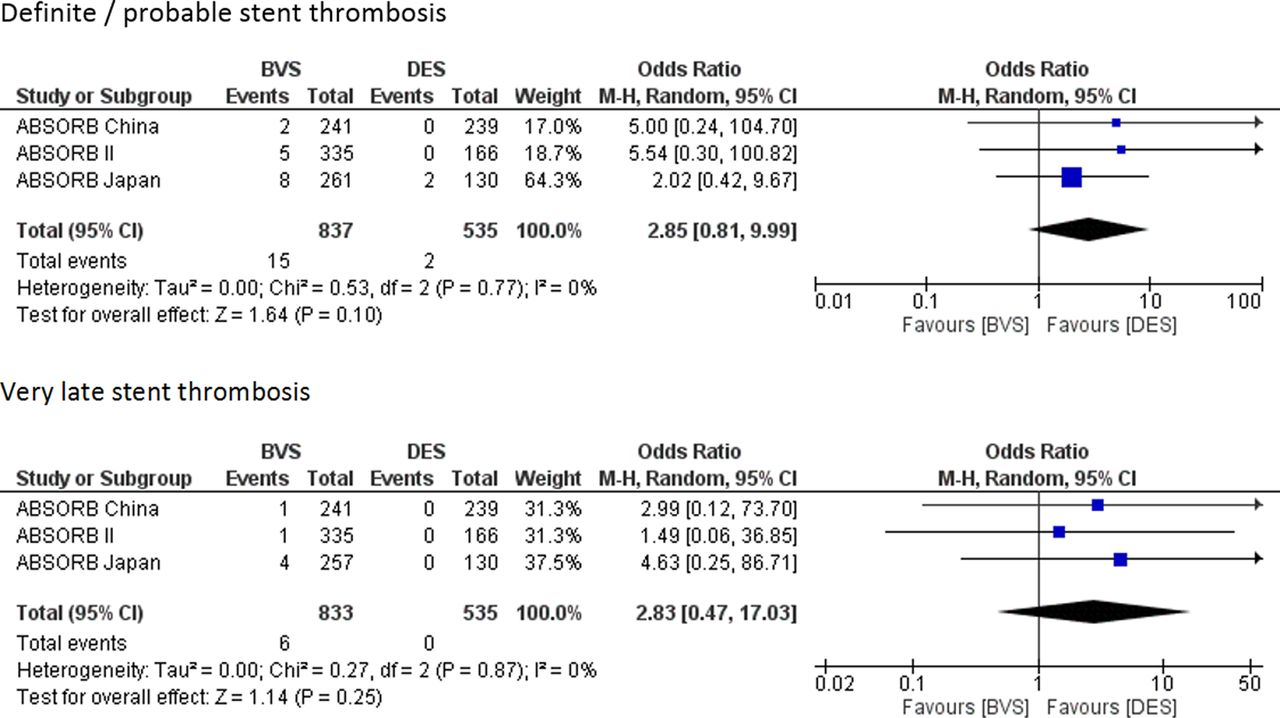
At 2 years, BVS was associated with higher rates of DOCE compared with DES (6.9% vs 4.5%; OR=1.53; 95% CI 1.06 to 2.23; p=0.02, I2=0%), ARI of 1.4%, RRI of 53% and NNH of 42. TV-MI was also higher with BVS compared with DES (4% vs 1.8%; OR=1.94; 95% CI 1.02 to 3.67; p=0.04, I2=0%), ARI of 2.2%, RRI of 122%, so was definite ST (2.1% vs 0.6%; OR=3.39; 95% CI 1.46 to 7.88; p=0.005, I2=0), ARI of 1.5%, RRI of 250%. No differences in all-cause mortality (1.2% vs 1.6%; OR=0.86; 95% CI 0.26 to 2.81; p=0.80, I2=28%) and TLR (3.9% vs 2.7%; OR=1.44; 95% CI 0.81 to 2.54; p=0.21, I2=6%) were observed between both groups (figures 2 and 3). Very late definite ST (>1 year) was numerically higher with BVS compared with DES, however, not statistically significant (0.7% vs 0%, OR 2.83, 95% CI 0.47 to 17.03; p=0.25), so was definite/probable ST (1.8% vs 0.37%, OR 2.85%, 95% CI 0.81 to 9.99; p=0.10) (figure 4). Only the three RCTs reported definite/probable ST rates and very late ST. These results were unchanged when fixed effects model was used. There was no evidence of publication bias by visual inspection of Funnel plots and by Egger's test. These findings may be undermined due to the few number of studies included in this analysis. Summary of clinical outcomes with BVS versus DES detailed in table 3.
Outcomes of interest at 2 years

Long-term outcomes in coronary artery disease (CAD) with bioresorbable vascular scaffold (BVS) versus drug-eluting stent (DES).
Long-term outcomes in coronary artery disease (CAD) with bioresorbable vascular scaffold (BVS) versus drug-eluting stent (DES).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Long-term outcomes in coronary artery disease (CAD) with bioresorbable vascular scaffold (BVS) versus drug-eluting stent (DES).
Discussion
To our knowledge, this is the first meta-analysis to date to report long-term clinical outcomes of BVS versus second-generation DES across the entire spectrum of CAD. Our study showed that at 2 years, BVS was associated with higher rates of DOCE, TV-MI and definite ST compared with DES. No difference in all-cause mortality and TLR between BVS and DES were observed. Interestingly, very late ST (beyond 1 year) continued to be numerically higher six events (0.7%) with BVS compared to none with DES. These results were consistent among randomised and observational studies.
One-year clinical outcomes of BVS compared with DES were reported in multiple RCTs and meta-analyses with conflicting results. In the largest RCT published to date, the ABSORB III trial, (everolimus-eluting BVS for CAD), BVS was non-inferior to DES in respect to the primary outcome; target lesion failure however subacute device thrombosis was higher.7 Other RCTs published showed equivalent clinical outcomes of BVS compared with DES at 1 year of follow-up.8–10 In a patient-level pooled analysis of four randomised trials,11 BVS was associated with similar rates of patient-oriented composite endpoint (all-cause mortality, all myocardial infarction or all revascularisation) and DOCE (target lesion failure) (cardiac mortality, TV-MI or ischaemia-driven TLR) compared with second-generation DES at 1 year of follow-up. However, in our analysis, extending follow-up of 2 years showed that BVS was associated with significantly higher DOCE rates compared with DES. This was driven mainly by significantly increased TV-MI and definite ST. In the patient-level pooled analysis by Stone et al, the higher rates of TV-MI observed was attributed to in part a non-significant increase in periprocedural MI and device thrombosis with BVS. Both in-device acute gain and minimal luminal diameter were significantly lower with BVS compared with DES, despite significantly higher rates of intravascular ultrasound/optical coherence tomography (OCT) use and balloon postdilation in that analysis.11
In a network meta-analysis including 126 526 patients, BVS was associated with higher risk of device thrombosis compared with cobalt–chromium DES, platinum–chromium DES and hybrid sirolimus-eluting stents at 1 year of follow-up (OR 2.28, 3.28 and 2.83, respectively).13 While a second meta-analysis showed that the pooled incidence of definite or probable ST after BVS implantation was 1.5 events per 100 patient-years.14 In our analysis, definite ST at 2 years with BVS was observed at a rate of 2.1% versus 0.6% with DES, while very late ST (>1 year) was 0.7% with BVS versus 0% with DES. The significantly increased definite ST was associated with higher rates of TV-MI and numerically higher rates of TLR. The finding of increased very late ST beyond 1 year is surprisingly alarming. This increased risk of ST believed by many to possibly be the initiating event of all the adverse outcomes with BVS.
Only three RCTs have published 2-year outcomes with BVS compared with DES while the largest trial, ABSORB III yet to release long-term results. The ABSORB II trial, enrolled mostly stable CAD with only ∼20% of patients being unstable angina, moderate to severe calcification were ∼15% and ACC/AHA Class B lesions were ∼97%. No difference was observed in DOCE (target lesion failure) between both stents (7% vs 3%, p=0.07). The ABSORB JAPAN enrolled around 12% unstable angina, 8% moderate to severe calcification and ∼22% ACC/AHA Class C lesions. The very late scaffold thrombosis rate (>1 year) was 1.6% with BVS compared with none in the DES arm and higher than the 0.6% observed in ABSORB II. DOCE rates were also similar between both stents (7.3% vs 3.8%, p=0.28). These DOCE rates are similar to our analysis, where DOCE with BVS was 6.9%, driven by TV-MI 4% and definite ST 2.1%. ABSORB CHINA trial enrolled around 20% stable angina and 64% unstable angina. Moderate or severe calcification was observed in ∼ 16%, while ACC/AHA class C lesions were ∼24%. At 2 years, DOCE rates were 4.7% versus 4.2%, while very late scaffold thrombosis was at 0.4% versus 0%. Moderate or severe calcification was a strong predictor of target lesion failure.9 ,23 In a large, single-centre registry (BVS EXPAND) which reported outcomes with BVS beyond 1 year (median follow-up 622 days), major adverse cardiovascular events (MACE) at 18 months were 6.8% driven by MI 5.2%. Definite scaffold thrombosis was 1.9% with very late scaffold thrombosis rate of 1.3%.25 Under-expansion of BVS was a frequent finding (26%) with a trend towards increased MACE (HR 2.25, p=0.16). Whether extending dual antiplatelets therapy beyond 1 year in BVS would mitigate the increased incidence of very late ST is unknown.
Lesion preparation and optimisation is critical for successful BVS deployment and improved clinical outcomes. High pressure postdilation seems to be safe in BVS as examined by intravascular imaging. One study used OCT after high-pressure postdilation and showed optimal BVS expansion, lower rate of strut mal-apposition and edge dissections, whether this translates into better clinical outcomes is debateable.26 The rate of postdilatation of BVS was overall low in our study 60%; this, however, was significantly higher compared with DES (46%). Whether the overall low average rate of postdilation or the inclusion of patients with STEMI in this analysis has contributed to the increased risk of ST and TV-MI with BVS compared with DES is unclear. The ABSORB JAPAN trial had a much higher rate of balloon postdilation (82%) and the 2-year target lesion failure rate was numerically higher, not statistically significant with BVS compared with second-generation DES (7.3% vs 3.8%).24 The ongoing ABSORB IV (ClinicalTrials.gov Identifier:NCT02173379), AIDA (ClinicalTrials.gov Identifier: NCT01858077) and COMPARE ABSORB (ClinicalTrials.gov Identifier: NCT02486068) RCTs will provide further data regarding clinical outcomes with BVS versus DES.
Limitations
The main limitation of this analysis is including observational studies. These were included due to the scarcity of long-term data from randomised trials. These studies were propensity score matched analyses from high PCI volume centres across several countries in Europe. All clinical events were adjudicated in one of the two observational studies (BVS EXAMINATION) by clinical review committee. Both RCTs and observational studies included in this analysis were of high quality and low risk of bias (see online supplementary table S2). It is also important to highlight that the analysis showed almost no heterogeneity and there is large concordance in the CIs between randomised and observational studies, confirmed by p value for interaction. Another limitation is that the definitions of clinical outcomes used among the included studies may have been different, which could have affected our results. Finally, lack of patient-level data hindered a more robust analysis and prevented identification of predictors of adverse events.
Conclusions
BVS may be associated with worse long-term clinical outcomes compared with DES in CAD. Long-term clinical outcomes from RCTs and patient-level analyses identifying predictors of adverse events are urgently required to shed more light on the long-term safety and efficacy of BVS.
Key messages
What is already known on this subject?
In randomised controlled trials, everolimus-eluting bioresorbable vascular scaffolds (BVS) were shown to have equal clinical outcomes compared with second generation drug-eluting stents (DES) at 1 year of follow-up.
What might this study add?
At 2 years, BVS was associated with higher device-oriented composite events compared with DES, 6.9% vs 4.5%, absolute risk increase of 1.4% and relative risk increase of 53%. This was driven by increased risk of target vessel myocardial infarction and definite stent thrombosis.
How might this impact on clinical practice?
This meta-analysis shows higher rates of device-oriented composite events, target vessel myocardial infarction and definite stent thrombosis with BVS compared with DES at 2 years. Randomised clinical trials should expeditiously report both long-term outcomes and predictors of adverse events with BVS versus DES.
References
Footnotes
Contributors All authors have contributed substantially to the manuscript and meet criteria for authorship.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.