Article Text

Abstract
Executive summary: This report addresses the needs and problems of grown-up congenital heart (GUCH) patients and makes recommendations on organisation of national medical care, training of specialists, and education of the profession.
The size of the national population of patients with grown-up congenital heart disease (GUCH) is uncertain, but since 80–85% of patients born with congenital heart disease now survive to adulthood (age 16 years), an annual increase of 2500 can be anticipated according to birth rate. Organisation of medical care is haphazard with only three of 18 cardiac surgical centres operating on over 30 cases per annum and only two established specialised units fully equipped and staffed.
Not all grown-ups with congenital heart disease require the same level of expertise; 20–25% are complex, rare, etc, and require life long expert supervision and/or intervention; a further 35–40% require access to expert consultation. The rest, about 40%, have simple or cured diseases and need little or no specialist expertise. The size of the population needing expertise is small in comparison to coronary and hypertensive disease, aging, and increasing in complexity. It requires expert cardiac surgery and specialised medical cardiology, intensive care, electrophysiology, imaging and interventions, “at risk” pregnancy services, connection to transplant services familiar with their basic problem, clinical nurse specialist advisors, and trained nurses.
An integrated national service is described with 4–6 specialist units established within adult cardiology, ideally in relation or proximity to university hospital/departments in appropriate geographic location, based in association with established paediatric cardiac surgical centres with designated inpatient and outpatient facilities for grown-up patients with congenital heart disease. Specialist units should accept responsibility for educating the profession, training the specialists, cooperative research, receiving patients “out of region”, sharing particular skills between each other, and they must liaise with other services and trusts in the health service, particularly specified outpatient clinics in district and regional centres. Not every regional cardiac centre requires a full GUCH specialised service since there are too few patients. Complex patients need to be concentrated for expertise, experience, and optimal management. Transition of care from paediatric to adult supervision should be routine, around age 16 years, flexibly managed, smooth, and explained to patient and family. Each patient should be entered into a local database and a national registry needs to be established. The Department of Health should accept responsibility of dissemination of information on special needs of such patients. The GUCH Patients’ Association is active in helping with lifestyle and social problems.
Easy access to specialised care for those with complex heart disease is crucial if the nation accepts, as it should, continued medical responsibility to provide optimal medical care for GUCH patients.
- grown-up congenital heart disease
- congenital heart disease
- GUCH
Statistics from Altmetric.com
Before the advent of cardiac surgery for congenital cardiac malformations, less than one fifth of children born with such lesions reached adulthood.1 Most survivors had mild lesions. Exceptionally, some with more severe or complex defects survived. The dramatic successes of surgical management, and more recently interventional catheterisation, in childhood has reversed this poor prognosis so that, by the 1980s 85% could be expected to reach adulthood. Most deaths from congenital heart disease now occur in adults (fig 1).2 Knowledge and training in congenital heart disease, adult cardiology, and general medicine are required for practitioners in this area.3 The lack of trained medical staff, and of specialised units to deal with the increasing population of adolescents and adults with congenital cardiac malformations, presents a major problem which requires urgent attention.

Data compiled from the statistics of the Office of Population Consensus and Surveys for England and Wales showing reported deaths from congenital heart disease in the various age groups. In 1958 death was most common in infancy and by 1986 deaths were more common over age 20 years.
The purpose of this document is to provide guidelines on the facilities required for the care of these patients. Suggestions are made about how to institute programmes to train specialists. We have chosen to use terms such as “grown-ups with congenital heart disease” (GUCH) as they are inclusive, simple, and best describe the important transition of the child through adolescence to adulthood, the latter being defined as aged 16 years or over by the Department of Health. Various other terms are used around the world (table 1). GUCH is familiar to the Department of Health and there is a Working Group GUCH (number 22) in the European Society of Cardiology. Congenital heart disease includes a large number and wide spectrum of malformations in the heart and great vessels. This document does not provide specific guidelines for management of individual conditions, as these can be found in the published Canadian Consensus Report,4 and will be available in the forthcoming report of the Task Force of the European Society of Cardiology for Grown-up Congenital Heart Disease. It is intended to promote collaboration between various professional groups involved in the care of adolescent and adult patients with congenital heart disease, as well as to inform administrators, purchasers, and those who distribute resources for healthcare, in the UK.
Acronyms used for grown-ups with congenital heart disease and organisations that register data on such patients
POPULATION OF GROWN-UPS WITH CONGENITAL HEART DISEASE
All patients aged 16 years and over with congenital malformations of the heart and great vessels are included in this population. Common lesions, such as mitral valve prolapse, and non-stenotic aortic valves with two leaflets (bicuspid aortic valve), even though congenital in origin, do not require management by experts in congenital heart disease. These patients, therefore, are not included in the projections for provision of services for grown-up congenital heart and vascular disease.
Additional patient groups may use, or come into the care of, the specialist unit established for grown-ups with congenital heart disease. This will depend on local facilities, the preference of the patients, and established practices for referral. Such patients include mature adolescents, patients with congenital syndromes which present with cardiovascular problems in adolescence or in young adult life such as Marfan’s syndrome, muscular dystrophy or other hereditary conditions, as well as adolescents and young adults with acquired diseases such as Kawasaki disease, vasculitis, rheumatic valvar disease, or diseases of the heart muscle and pericardium.
Classification
The existence of a large number of individual lesions and a variety of surgical treatments makes it important to have a broad system for classification. For this report, the major function of which is to provide guidelines for optimal care of patients, a system based on the need for specialist care has been used. An attempt has been made, therefore, to classify lesions based on their complexity, recognising in this way mild, moderate and severe categories and to use this to provide recommendations for level of care. It is recognised that this is no more than a broad guideline, since lesions often occur in combination. Furthermore, individual lesions vary in clinical severity. Those with ventricular septal defect or Ebstein’s malformation, for example, may exhibit mild to severe manifestations. With these caveats in mind, the lesions that are classified as complex, requiring specialist expertise, are presented in table 2.
List of conditions considered to be complex with special risks and complications
Current population
The prevalence of congenital cardiac malformations in the grown-up population is not known, and the absence of exact numbers has made planning difficult.5 Estimates can be made from the known birth rate, the incidence of congenital cardiac malformations, and the survival rate of the common lesions to be found in the majority of patients. These were published by the recent Bethesda conference in the USA.6 Using the same methods (table 3), it is estimated that there could be 20 000 patients with complex lesions currently requiring specialist care in the UK. The fact that these patients exist, and attend non-specialist clinics, was demonstrated by a study in the north of England.7 This confirmed that there were some patients with complex diseases receiving treatment in district hospitals, some never having been referred to a regional or specialist centre. A telephone survey of all units providing cardiac activity, identified by the presence of a coronary care unit, was conducted for the purposes of this document in 1994. This aimed to identify the facilities, and/or the staff, which were available for the grown-up population. It revealed little organisation, and almost no data concerning the number of patients. Questionnaires, 286 in all, were then sent to a designated consultant in each hospital listed in the records of the British Cardiac Society for the UK as delivering coronary and/or cardiac intensive care. A request was included to pass it to the consultant interested in congenital heart disease, if one was available; 208 (72%) were returned and 33 (16%) reported having some form of service for adults with congenital heart disease. Outpatient clinics using visiting specialist consultants existed in 30 of the centres. Only 12 centres reported seeing more than 100 grown-ups with congenital malformations each year, while 14 served between 50 and 100 patients.
Estimated prevalence of congenital heart disease for the population of the UK
Future growth
A recent study has attempted to predict the number and complexity of patients with congenital heart disease who will survive to adulthood, and hence present to future clinics dealing with congenital cardiac disease in the grown-up population. The study used a combination of 10 years of data from the north east regional database, and the predicted survival of individual lesions culled from the world literature.8 The authors divided the predicted survivors into those who would, and would not, require specialist care. When extrapolated to the UK as a whole, the predicted annual increase in patients requiring specialist care would be approximately 2000 new patients per year. Adding patients unknown before age 16 years, immigrants and asylum seekers will increase this to at least 2500.
Composition
The make up of a specialist clinic for congenital cardiac disease will be significantly different for children compared to grown-ups.9 Some simple lesions will have been treated definitively, or require no further assessment. Such patients may be discharged from cardiological services before reaching adulthood. The clinic for grown-ups, therefore, will have a disproportionate representation of lesions at the severe end of the spectrum. This must be taken into account when planning the provision of service and its funding. The pattern of diseases seen in clinics for grown-ups differs depending on whether they are located in a district general or regional setting or outside regional setting.7
Some patients reach adulthood without having had or needed surgery. These “natural survivors” include patients with relatively minor abnormalities, as well as those with complex conditions and “balanced physiology”. They also include patients with established pulmonary vascular disease. Although, in the UK, the diagnosis of congenital heart disease is usually made in childhood, some patients will also present for the first time as adults.
The majority of patients in a specialised service will have had one or more palliative or “corrective” operations in childhood. Few are “curative”, and most require long term follow up, and often further surgery. These operations include the inevitable need for replacement of biological and prosthetic valves or conduits, as well as procedures designed to deal with residual haemodynamic lesions such as pulmonary regurgitation after repair of tetralogy of Fallot. The survivors of “definitive surgery” for complex defects often have notably abnormal circulations. The late electrophysiological and haemodynamic problems after procedures such as the Fontan operation or the intra-atrial repair of transposition (Mustard or Senning operations) have become apparent and are progressive. These patients are challenging, both for the cardiologist and the surgeon specialising in the care of the GUCH population. Severe heart failure is likely to occur in an increasing number of patients, with requirements for both specialised medical care and surgical intervention, including heart and lung transplantation.
OUTPATIENT SERVICES
Transition from the paediatric clinic
There is no natural division between adolescence and adulthood.10 The speed of physical and emotional maturity is related to factors such as sex, family background, and coexisting disease. Some adolescents are best served by remaining in the familiar paediatric setting, particularly those with immature mental development. Others may mature early, such as the pregnant 14 year old! They will need earlier transfer to the service for grown-ups. A specialist transition clinic is helpful but not mandatory, and is the first step to the creation of a successful clinic for the grown-up population. Optimal management requires the collection of key information about treatment in childhood, particularly previous operation reports. This must be available at the time of first attendance.
The initial assessment should include consideration of prognosis and risk factors, and advice should be given concerning lifestyle. Many children reach adolescence with little understanding of the implications of their cardiac condition. This can result from parental overprotection, or lack of any instruction. Education of the patients themselves is needed at this stage. The patient must be able to have a private discussion with the specialist, as many adolescents resent parental presence. This entire process of transition of responsibility and knowledge from the parents to the adolescent and young adult is time consuming. It may also be stressful for both patient and parents. The nurse specialist or counsellor should be available to help.
Specialist outpatient clinic
Transition to the specialised GUCH clinic should occur around age 16–18 years. Timing needs to be flexible and depends on the circumstances of the individual patient. The majority of patients are seen only in the outpatient clinic. As in the transitional clinic, time must be allocated to discuss a broad range of issues, such as exercise, future employment, contraception, pregnancy, risks of recurrence of defects, and special risks and dangerous activities. Opportunity must be provided for private discussion between the patient and specialist (one to one as is routine in adult medicine). The nurse specialist or counsellor in the outpatient department should see all new patients, as well as being available for old patients. The first consultation is often the time to introduce patients to the GUCH Patients’ Association, whose representative may be at the clinic or whose literature should be available. Routine investigations needed in the outpatient clinic are a chest radiograph, an ECG, and an echocardiogram performed by an experienced technician or a doctor. Ambulatory monitoring, exercise testing, and blood testing should also be available. Unit protocols are particularly useful when there is a large, changing junior staff. Access to more sophisticated investigations is vital for a specialised centre. These include magnetic resonance imaging, stress echocardiography, and radionuclear scanning (see below). After assessment of medical status and prognosis, the level of care and follow up needs should be defined. Some patients need follow up exclusively in the specialist clinic, while others can have “shared care”’ with physicians and cardiologists interested in the spectrum of congenital heart diseases. These plans should take geography, travel and education into consideration and need to be explained to the patient, their family, and to the general practitioner (see below). University health services and course doctors may need information. Accurate information about care in childhood must be available at referral to the grown-up clinical service. Many hospitals have the policy of destroying records after 8–10 years. This should be stopped by law for patients who have attended a hospital with congenital cardiac malformations.
Non-specialist or district general hospital clinics
Some patients live a long distance from the specialist unit. They can have follow up shared locally by physicians or cardiologists interested and trained in congenital heart disease. For less complex lesions, care can be based at the local unit, provided liaison is established with the specialist team. This is important particularly in special circumstances such as pregnancy, or when non-cardiac surgery is required. For even the more severe lesions, it is useful if the local unit has some involvement in care as these patients may be admitted initially to their local unit in an emergency. The need for close liaison, with mutual trust and good communication between the specialist and non-specialist units, cannot be overemphasised.
INPATIENT SERVICES
Clearly a minority of grown-up patients require hospital admission (< 10% of the population in a specialist unit). It is advantageous for the patients to be within, or contiguous to, a multidisciplinary teaching/university hospital. A high proportion of patients have important non-cardiac medical and surgical problems requiring specialist advice. The presence of other specialities on the same site, therefore, is highly desirable. A dedicated ward area for the grown-ups with congenital heart disease needs to be established, with its own specified facilities. The unit is ideally located, and administered, within the directorate of adult cardiology. This enables patients to share all facilities for adults, along with the technology, educational facilities, staff, and budget available for their treatment. As many patients are younger than the usual adult, the unit must provide appropriate space for study and examination, and be organised with the young in mind. A quiet room for study and examination is useful as well as a room with television, computers, and games. A small kitchen in the unit is ideal and much used by hungry teenagers. Despite the fact that the unit will inevitably include young patients, the average age of patients admitted to the unit has and will increase with time (fig 2). This should be incorporated into planning.

Number and ages of grown-up patients with congenital heart disease admitted to the National Heart Hospital and Royal Brompton Hospital 1975 to 1997. In the last decade there has been an increase in adults over age 30 years. From JS, GUCH Unit database.
The major reasons for cardiac medical admissions are for control of arrhythmias, and interventional or diagnostic cardiac catheterisation. These services need to be available in the specialist centre. Admissions for management of heart failure are often linked with assessment for transplantation. “Other” reasons are increasing. They include investigation and assessment of non-cardiac problems, both surgical and medical, as well as infections, endocarditis, and pregnancy. Medical and surgical patients should be managed together before and after any necessary surgery so as to concentrate expertise and training. This has been successfully achieved in at least two units in the UK. It is predicted, from data currently available, that admissions to the specialised unit will increase in number and complexity and 300–500 admissions each year can be anticipated. To achieve this the number of specialised units will need to be limited to about six for England and Wales.
Complex patients require care from a dedicated team of consultant cardiologists, surgeons, anaesthetists, intensivists, and nurses as well as support from other medical services. This enables the training of those specialist cardiology registrars who need exposure to the care of GUCH patients during their training. The specialist registrar would generally come from a rotation in adult cardiology and spend from 3–6 months attached to the unit. According to the current guidelines, this would be the minimum amount of time needed for accreditation in adult cardiology. There should be experienced technical staff familiar with congenital heart disease available in the echocardiographic unit, catheterisation laboratory, and the facility for magnetic resonance imaging.
MEDICAL ISSUES
Contraception and pregnancy
It is the duty of the specialist in the clinic for grown-ups with congenital heart disease to provide informed advice on contraception, including discussion of risks.11 There are few data on the safety of the various contraceptive techniques in such grown-up patients and informed evidence based advice remains difficult because of low absolute numbers of patients and the many different types of anomalies and therapies. The low oestrogen pill may be contraindicated in patients at risk of thromboembolism, such as those with cyanosis or pulmonary hypertension, or because it may aggravate heart failure or upset anticoagulant control. The dangers of the “morning after pill” should be explained to those at particular risk of acute fluid retention and/or thromboembolism. Sterilisation, by tubal ligation for example, although the most secure method, can be a high risk procedure in patients with complex malformations, and/or those with pulmonary hypertension. Sterilisation of the male partner of a female with congenital heart disease should only be recommended as a last resort, and only after full explanation of the prognosis of the patient. The specialist in GUCH needs to interact both with the general practitioner and gynaecologist to provide optimal advice.
With the decline in the incidence of rheumatic heart disease, congenital malformations now represent the most common cause of morbidity and mortality from heart disease in pregnancy.12,13 This usually arises from poor assessment and advice before pregnancy, along with substandard management of the delivery and the puerperium. There may also be lack of communication between obstetrician, cardiologist, and anaesthetist. Counselling by an expert before pregnancy is important, and should include genetic advice, assessment of fetal risk from maternal complications, appropriate management of anticoagulation, and discussion of the likely risk of maternal complications14 (table 4). Periconceptual use of multivitamins may reduce the occurrence of certain lesions, and this should be mentioned.15 Expert fetal cardiac echocardiography must be available, and its consequences discussed early.
The outcome of pregnancy is favourable in most women with congenital heart disease, provided functional class and systemic ventricular function are good. A recent survey highlighted endocarditis and pulmonary hypertension as the major risk factors for maternal death.13 Pulmonary hypertension presents a serious risk during pregnancy. Even patients considered only to have “moderate” pulmonary hypertension after repair of their congenital heart malformations are at increased risk. Events often occur after delivery. Antibiotics should be given as the membranes rupture because of the risk of endocarditis. Intravenous amoxycillin is currently recommended. Pregnancy does not appear to produce deterioration or reduce the survival of homografts in the right ventricular outflow tract, or autografts on the systemic side of the circulation.16 In patients with mechanical valves, however, thromboembolic problems are more common, and there may be accelerated degeneration of bioprosthetic left sided valves.17,18 Few data are available on the impact of pregnancy on long term ventricular function in patients with complex circulations, particularly in those in whom the right ventricle serves the systemic circulation. There is a small group of patients with complex congenital cardiac malformations, pulmonary hypertension, and aortic disease in whom pregnancy is dangerous.19,20 Such patients at high risk should be managed and delivered in specialised centres, with appropriate experience and multidisciplinary expertise in congenital heart disease, obstetrics, anaesthesia, and neonatology. A coordinated care pathway for supervision of delivery and the puerperium needs to be in place, and recorded in the notes of the patient, by the beginning of the third trimester. These patients may need to come from “out of region” to specialist units, and referrals should be facilitated. Every specialised centre dealing with GUCH patients should develop a close and formal liaison with a department of obstetrics.
Infective endocarditis
Most, but not all, patients have a life long risk of endocarditis21 (table 5). It is vital that the specialist centre is informed as soon as the diagnosis is suspected. Prompt referral is usually indicated. General practitioners and physicians need to know that early diagnosis, and microbiological isolation of the responsible organism, are vital. Delay in the diagnosis and referral of endocarditis, however, remains a common problem and adversely influences outcome. Physical signs may be difficult to interpret. Antibiotics are frequently prescribed before the diagnosis is considered, or before obtaining appropriate blood tests which should include blood cultures which general practitioners are reluctant to do. It is easy for the non-expert to miss vegetations when performing echocardiography in patients with complex congenital cardiac malformations. Delay in diagnosis is longer in “right-sided” endocarditis, or if the causative organism is non-pyogenic. Fungal endocarditis is particularly difficult to treat. It may occur in patients with newly implanted biological valves, or after excessive use of antibiotics. Surgery has an important role in the management of endocarditis, but the optimal timing may be difficult.
Congenital cardiac lesions which do not require protection from infective endocarditis
Maintenance of good dental health is important, and this should be re-enforced regularly. Antibiotic prophylaxis for at risk procedures does not always prevent the disease. Patients at high risk need to be made aware of this. Other portals of entry for infection include skin sepsis, trauma, tattoos, and body piercing, and unusual occupations may lead to infection with rare organisms. Education of patients, general practitioners, and physicians about the risks of endocarditis, its identification, and the importance of early diagnosis needs constant re-enforcement. Antibiotic prophylaxis is recommended after surgical repair of most conditions. There are conditions which do not need prophylaxis (table 5).
Arrhythmia and electrophysiology
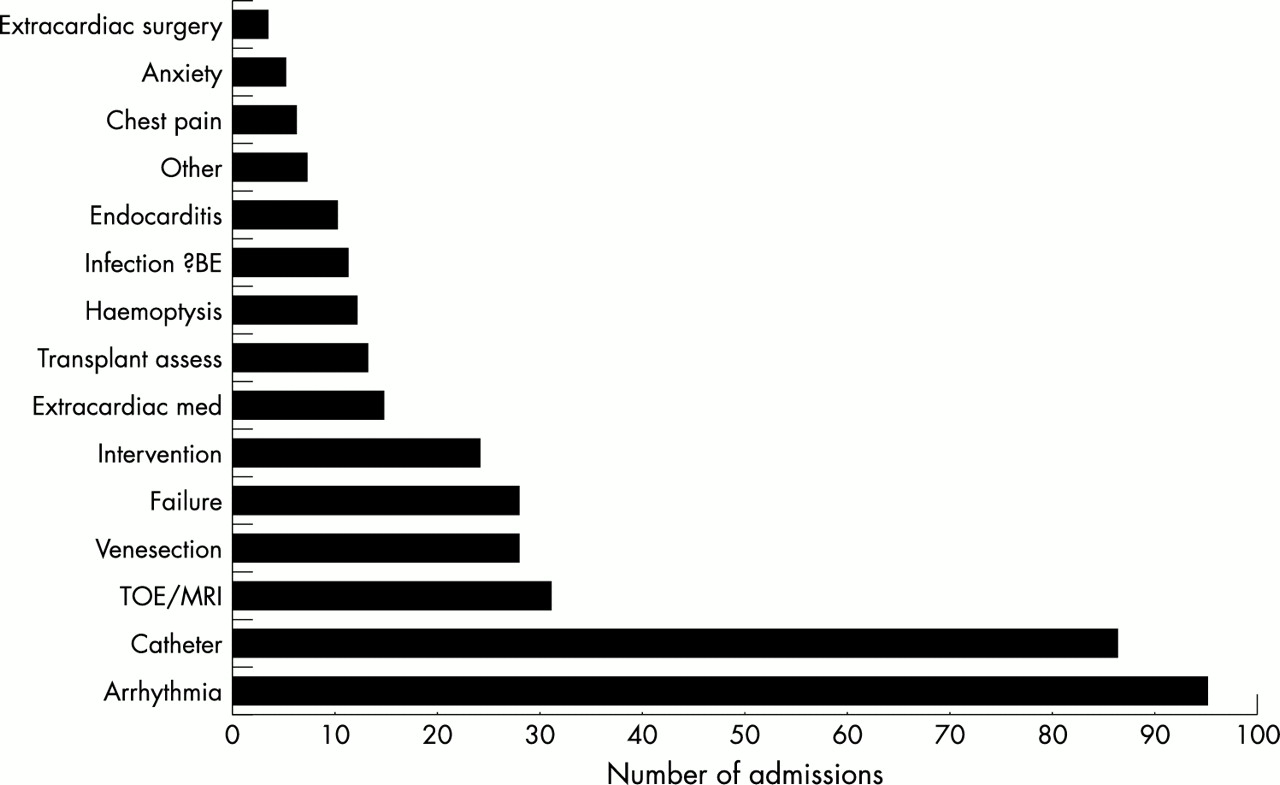
Arrhythmia, most commonly atrial flutter, is an increasingly important cause of morbidity and mortality, and is a need for hospitalisation in GUCH patients (fig 3). Patients with arrhythmia may present with palpitation, dizziness or syncope, effort chest pain or hepatic discomfort, or as part of an overall haemodynamic deterioration. Several factors contribute to the increased occurrence of arrhythmia. They may be part of the natural history of certain malformations, may result from scarring from cardiac surgery, both in the atria and ventricles, or be the consequence of the postoperative unnatural history and disturbed haemodynamics. Electrical and mechanical factors interact, and an arrhythmia is often the consequence of dilation and/or hypertrophy and fibrosis. As a result, optimal management of complex patients should involve the specialist cardiologist in grown-ups with congenital heart disease, as well as an electrophysiologist with a particular interest and experience in the area. Management may require transoesophageal echocardiography and cardiac catheterisation, electrophysiological mapping with ablation, cardiac surgery, or a combination of these approaches.22–24 Implantable defibrillators are increasingly being considered if the patient is felt to be at increased risk of sudden death. Whenever cardiac surgery in the GUCH patient is undertaken, the electrophysiological consequences of the defect and the operation should be considered, and concomitant surgery may be appropriate. This is an important area that requires specialist recognition and funding.

The principal reasons for 373 medical admissions to the Royal Brompton Hospital GUCH unit in 1997. Abbreviations: assess, assessment; BE, bacterial endocarditis; med, medical; MRI, magnetic resonance imaging; TOE, transoesophageal echocardiography. From JS, GUCH Unit database.
Implantation of pacemakers can present particular difficulties in this special population and experience is needed to prevent complications. Complete heart block occurs as part of the natural history of some conditions, and can be an immediate or late complication of intracardiac surgery. The problems encountered are venous access to the heart, difficulty in siting leads in non-standard chambers, high thresholds, low sensitivity, and displacement of leads. Anticoagulation is mandatory in patients with a right-to-left shunt because of the risk of systemic thromboembolism. Innovative approaches are often needed, particularly in patients with complex circulations such as after the Fontan procedure.
An electrophysiologist with experience in grown-ups with congenital heart disease is thus an important member of the specialist service. Experts with these particular skills will be rare and cannot be expected to be available in every regional centre. Interventions are time consuming, challenging, and expensive. Early results and risks of recurrence are currently less good than in adults with structurally normal hearts. This is, however, a rapidly developing field, and is likely to make a major impact on management.
Cardiac catheterisation and intervention
Despite new diagnostic imaging techniques, cardiac catheterisation with angiography remains important in the management of grown-ups with congenital heart disease. Diagnostic investigations should routinely include coronary angiography, which often demonstrates unexpected abnormalities of clinical relevance. There is an increasing need for therapeutic interventions. Both diagnostic and interventional procedures should be performed in the specialist centre by a trained investigator experienced in congenital heart disease, and guidelines are available. The scope and success of innovations in this field are increasing and interventional catheterisation can simplify surgical management, or obviate the need for surgery altogether.
Non-cardiac surgery
As the population with congenital heart disease ages, comorbidity becomes more common with an increasing need for non-cardiac operations. Issues to be addressed are summarised in table 6. Certain procedures are required more often than in the normal population, such as intervention for gallstones, cerebral abscess, or scoliosis, and abdominal hernias in Fontan patients can present repair problems. Basic preoperative assessment should include an ECG, chest radiograph, echocardiogram, and blood tests for full blood count and coagulation screen. The specialist team should always be involved in the care of complex patients, as this minimises avoidable errors which can cause important morbidity or even death.25
There is a case for non-cardiac surgery in patients with special risk (table 2) being undertaken within centres possessing both specialists for grown-ups with congenital heart disease and multidisciplinary experts. Advice should always be sought from the specialist centre, even for apparently simple operations. Some common surgical problems—for example, varicose veins or hernias in a patient with the Fontan circulation—reflect the underlying haemodynamic status, and need specialist assessment and supervision. Fluid balance is critical in cyanotic patients and in those with incipient heart failure. Patients with pulmonary hypertension are susceptible to catastrophic haemodynamic changes as a result of vomiting, induction of anaesthesia, and haemorrhage. As careful choice of anaesthetic agents and manipulation of intravascular volumes are so important, a cardiac anaesthetist is required for the at-risk patient having non-cardiac surgery. Recovery is often necessary in an intensive care unit. Nursing staff should be informed about specific issues related to the congenital cardiac malformation. The advantages of siting the specialist unit in a multidisciplinary environment are obvious.
Non-cardiac medical problems
In common with extracardiac surgery, there are increasing needs for specialist advice in other disciplines (table 6). The particular needs are for endocrine support (as in the case of thyroid dysfunction in patients on amiodarone), rheumatology advice (for example, in those with gout, and arthropathy in cyanotic patients), neurology advice, orthopaedic counsel for trauma and spinal disorders, as well as renal expertise. The specialist in grown-ups with congenital heart disease should be involved in the management of all extracardiac diseases in complex patients, as certain medications can upset anticoagulant control, cause renal dysfunction, and precipitate heart failure, thrombosis, or haemorrhage. Endoscopy can be dangerous in this group of patients and has led to deaths.
Advice concerning lifestyle
Patients have many of the constraints and difficulties associated with chronic medical conditions. Solutions may relate to, influence, or be influenced by the underlying cardiac conditions, and so specialist medical input is often required (table 7). Health and life insurance and mortgages can be difficult or impossible to obtain.26 The actuarial risks quoted by insurance companies usually bear little relation to long term outcome. The GUCH Patients’ Association has addressed this and can give useful advice. Support from specialists knowledgeable about prognosis, and complications, is important as attitudes of insurance companies vary considerably. Close liaison between the general practitioner, workplace or agency health team, and the specialist in congenital heart disease is always essential, but general practitioners should be discouraged from giving advice on prognosis and complications. Other issues should be discussed specifically with the patients, including the importance of avoiding cigarette smoking, recreational drugs, obesity, and excessive intake of alcohol. For some, the disco is a risky hobby! Anxiety concerning genetic issues, sudden death, abnormal body image, and fertility must be recognised and sensitive counselling and support are necessary. The particular needs and problems of the woman with congenital heart disease need to be recognised.27
Acquired heart disease
Acquired heart disease will occur with increasing frequency as the population ages. Development of coronary arterial disease, and/or systemic hypertension, can cause new or worsening symptoms requiring treatment of both the congenital and acquired disorders. Combined congenital and acquired problems may require input from adult cardiologists and cardiac surgeons. This again emphasises the importance for the specialised unit to be established within the fully equipped adult cardiology department.
Pulmonary hypertension
The specialised clinics for grown-ups with congenital heart disease will inevitably contain a number of patients with pulmonary hypertension and pulmonary vascular disease as these are the most common forms of cyanotic congenital heart disease to reach adulthood. The demonstration of haemodynamic improvement, and in some studies increased life expectancy, in primary pulmonary hypertension with a variety of treatments including oxygen, calcium antagonists, prostacyclin, and sildenafil is encouraging. Further studies are needed in the population with pulmonary vascular disease secondary to congenital heart malformations. Supplemental oxygen and anticoagulation should be considered for these patients. A coordinated plan for management should be established before the clinical situation becomes too severe. This will include both medical treatment and consideration of transplantation.
Death and necropsy
Death often occurs in patients unexpectedly. Knowledge of the pathological consequences of congenital heart disease and its treatment are vital. Necropsy and examination of relevant organs by an experienced cardiac pathologist are highly desirable. General practitioners need to be made aware that death, particularly “sudden”, requires a full enquiry. The referral centre should be informed and a necropsy should be obtained. A necropsy should be sought for all deaths occurring in hospital and the consultant or senior staff member may have to accept responsibility for obtaining permission and explaining the need for organ retention. A conference in specialist units to discuss each death is recommended. This contributes to knowledge of all concerned, the improvement of medical care, and is a useful exercise for audit and teaching.
CARDIAC SURGERY
Cardiac surgery in the GUCH patient presents major difficulties in management and technique. As in paediatric cardiac surgery, there are strong arguments for concentrating care and surgical practice into a small number of specialist centres where a critical mass of patients will allow expertise to be gained and taught28 and thus lead to better outcomes.
Specific surgical problems
There are a wide range of conditions which require specialist surgical intervention (fig 4A,B). A distinction needs to be made between relatively simple conditions, such as isolated replacement of the aortic or mitral valves, and more specialist surgery to be performed in the specialist unit. Incidence of the various types of operation differ in established GUCH units depending on the length of time established, specific expertise, population served (regional, national) and relation to paediatric cardiac centre(s). Surgeons who carry out operations on complex congenital heart diseases (table 2) need to be trained, and to be practising in both adult and paediatric congenital heart disease. They need to be an integral part of the specialised unit and to share responsibility for reviewing the diagnostic information and indication for surgery, as well as anticipating and planning for particular complications.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Operations performed in 1997 in the Royal Brompton GUCH specialist unit. (A) First operation. *Atrial septal defects (ovale type) now mostly closed by non-surgical intervention, profoundly reducing surgical treatment for this lesion. (B) Reoperation. Abbreviations: AoV, aortic valve; ASD, atrial septal defect; AVR, aortic valve replacement; clos, closure; Co Ao, coarctation of the aorta; Lig, ligation; LV, left ventricle; MV, mitral valve; OP, ostium primum; PA, pulmonary artery; PDA, patent ductus arteriosus; prev, previous; Reop, reoperation; Rep, repair; repl, replacement; Res, resection; RVOTR, right ventricular outflow tract reconstruction; Sec, secundum; sub AS, subaortic stenosis; TC, total correction; TP, transplant; valvot, valvotomy; VSD, ventricular septal defect. From JS, GUCH Unit database.
Unique surgical problems exist in this group of patients. For example, replacement of conduits may appear to be simple, but may require modification of both surgical and bypass techniques depending on the position of the conduit and on the presence or absence of associated defects. Sternotomy itself can be dangerous when the heart is adherent to the sternum so that femoral bypass may be required. The healing of femoral incisions, or their infection, often prolongs the stay in hospital. Haemostasis may be difficult during and after surgery, particularly in reoperations and in cyanotic patients with abnormal clotting factors. Blood losses are increased by dense pericardial adhesions from previous surgery and by long bypass times. Requirements for large transfusions of blood and clotting factors have cost implications, and specialist haematological support is essential. Myocardial dysfunction and pulmonary vascular disease are often present and underestimated in patients who may have undergone primary repair at an older age than is currently recommended, or already have had several operations. Patients with cyanotic heart disease present the most problems and their stay in intensive care and hospital is considerably longer than for adults undergoing valvar or coronary arterial surgery.
Postoperative intensive care and anaesthesia
Postoperative intensive care presents difficult and unique problems. Intensivists, anaesthetists, and intensive care nursing staff must understand basic surgical anatomy and pathophysiology of repaired and unrepaired congenital heart disease, along with the more common postoperative problems. The early recognition of impending difficulties is essential, but difficult to teach in units dealing with small numbers or even occasional patients. Expert management of arrhythmias, which are common after surgery, is important and access to expert electrophysiological help may be needed. Coordinated care between cardiologists, surgeons, and the staff of the intensive care unit is important. Many decisions concerning management need to be made at senior levels rather than delegated.
Transplantation
Transplantation of the heart, the heart and lung, or an isolated lung has to be considered in some patients when the risks of proposed conventional surgery are high, or if conventional surgery is not possible in the presence of a deteriorating clinical state. Morbidity and mortality are increased by the complexity of previous surgical procedures, underlying anatomy, inadequacy of the pulmonary vascular bed, collateral vessels, and the frequently associated renal dysfunction. Innovative surgical techniques are often required for harvesting the donor organ and transplantation. Transplantation in this population is a specialist problem within a supra-regional service. Only a very small number of units is likely to be required in the UK.
THE SPECIALIST UNIT
Role
This is the centre within which patients with complex disorders (table 2) are managed, and to which problems in any grown-up patient with congenital heart disease can be referred. The unit serves as a focus for excellence for clinical care. Equally important, it enables education and training of the profession and facilitates innovative research. The data from the unit with regard to outcomes will “feedback” to paediatric cardiologists, thus refining the care provided in childhood and permitting the introduction of new superior forms of treatment.
Site/referrals
-
The specialised unit should be located in an adult medical environment ideally with multidisciplinary specialist provision.
-
Referrals should be from general practitioners and regional centres, and nationally from other regions. Fewer grown-up units are likely to be required than those dealing with paediatric cardiology and cardiac surgery. Every region should have some service for these patients, but may not require a full specialist unit as currently there are both insufficient patients and experts.
Staffing requirements
-
A minimum of two cardiologists with specialist training in the management of grown-ups with congenital heart disease. One cardiologist should have experience in interventional techniques other than coronary angioplasty unless a paediatric cardiologist is available. Both cardiologists should be familiar with the echocardiography of congenital heart disease, including transoesophageal echocardiography, and both should perform these investigations, not relying solely on technicians, however experienced. Large centres may require more than two consultant cardiologists, particularly as the cardiologists start to subspecialise in different aspects of congenital heart disease. At the present time, this is impractical unless there is an established academic/research input. It is advisable to share duties where possible with the adult cardiology department and its staff. Paediatric cardiologists may also be involved providing their training is appropriate and the location is convenient.
-
A minimum of two cardiac surgeons trained and practising in adult and paediatric cardiac surgery.
-
An association/connection to a transplant centre, not necessarily restricted to one, with surgeon(s) familiar with congenital cardiac malformations. It is not necessary for the cardiac surgeons on site to have experience in this field.
-
An electrophysiologist with training and experience of arrhythmias in congenital as well as acquired heart disease, pacemaker technology, ablation technology, and defibrillator implantation.
-
Two or more cardiac anaesthetists with specific interest and experience in handling congenital cardiac malformations at all ages, particularly in adults.
-
Dental advice and a clinical service for dental surgery should be available, but not necessarily on site. The specialist unit may need to provide inpatient beds for extractions in “at risk” patients, particularly for wisdom teeth.
-
Close links with other specialist departments, including genetics, endocrinology, respiratory medicine, neurology, and surgery, ideally on site.
-
A formal link with a named obstetrician/obstetric team to allow the centralisation of expertise in management of pregnancy in “at risk” patients.
-
A clinical nurse specialist.
-
Liaison with the GUCH Patients’ Association (or appropriate similar organisation).
-
Appropriate numbers of medical secretaries.
-
Research coordinator/administrator for database and liaison with national databases.
-
A cardiac pathologist with an interest in congenital cardiac malformations.
-
A training programme for specialist training, as well as for cardiologists with an interest in grown-ups with congenital heart disease.
TRAINING
Medical training
The current curriculum for specialist training prepared by the Specialist Advisory Committee (SAC) in Cardiology recognises the importance of a basic knowledge of congenital heart disease in the adult for all trainees, as well as a requirement for more rigorous training for those wishing to subspecialise in the subject. Both are difficult to acquire.29 It was recommended that cardiology trainees wishing to subspecialise in adult congenital heart disease should be seconded, part time, for 3–6 months to a specialist unit dealing with paediatric cardiology. In addition, during basic training, all cardiology registrars should attend an outpatient clinic specifically for adults with congenital heart disease for at least six months. In the final, sixth, year of training, the subject of adults with congenital heart disease was designated as one of four such areas for subspecialist training. Despite these recommendations, very few cardiology trainees have received even basic minimal exposure to congenital cardiac malformations. Thus consultant cardiologists with little experience of the issues in the management of these patients should be expected to refer patients appropriately.
Training for specialist cardiologists
Specialists for the management of grown-ups with congenital heart disease require the following skills and knowledge:
Knowledge of congenital cardiac malformations and their treatment in infancy and childhood.
Knowledge of general medicine.
Knowledge of adult cardiology, including coronary arterial disease and expertise in echocardiography, cardiac catheterisation, pacing, electrophysiology, and post operative care.
Special knowledge and ability to perform and/or interpret transthoracic and transoesophageal echocardiography, magnetic resonance imaging, and cardiac catheterisation in the grown-up with congenital heart disease.
Postoperative care.
It is likely that trainees will come from a background of either adult or paediatric cardiology. In a specialist centre for grown-ups with congenital heart disease, there may be an advantage to appointing consultants from both backgrounds, ensuring seamless care for the younger teenagers in the transition clinic and the older patients with congenital and acquired cardiac disease. We wish to avoid the argument as to whether a paediatric or an adult cardiologist should be the preferred person to look after patients with congenital heart disease in adulthood. Either can undertake the task with appropriate training. The quality and training of the individual is more important than the starting point from which he or she came.
The current structure for obtaining the certificate of specialist training is inappropriate. It may be necessary to consider dual accreditation in both cardiology and paediatric cardiology, or a specialist accreditation in “cardiology with an interest in grown-ups with congenital heart disease”. It is clear, however, that the maximum training acceptable for specialist registrars in the current system is six years, with most speciality training requiring only five years.
The chairman and secretaries of the SACs in cardiology and paediatric cardiology met on 15 May 2001 and concluded that: “Two training structures for ‘specialists in grown-up congenital heart disease’ are proposed” for the specialised units:
Trainees from an adult cardiac SpR programme
-
After the first three years in general cardiology training, which will include one year with additional training in general internal medicine, trainees wishing to specialise in adult congenital heart disease will rotate to a cardiac centre that accepts tertiary referrals of patients with congenital heart disease, including adults. The training will cover all aspects of congenital heart disease and must include a period of at least six months in the care of infants and children.
-
As in the current training programme, a sixth year will normally be derived from a period of training in research, ideally in a subject related to congenital heart disease in adults. Alternatively the year could be credited for advanced training in a related subspeciality, such as intervention or electrophysiology.
Trainees from a paediatric cardiac background
-
The first three years will be spent in general paediatric cardiology. This will be followed by two years in adult congenital heart disease, but must include six months general (internal) medicine in a district general hospital. An additional year, out of programme, to obtain experience in research or additional training, is considered to be desirable.
It will be important for postgraduate deans and regional speciality advisors to encourage the training of physicians in adult congenital heart disease and to identify and place trainees wishing to subspecialise in the subject. This will require flexibility.
The specialist in management of GUCH patients will be responsible for the care and investigation of such patients in their region. It is recognised that cardiologists in the district general hospitals may wish to participate in the shared care of some adult patients with congenital heart disease. For this reason, training should be organised for the “adult cardiologist with an interest in grown-ups with congenital heart disease”.
Training for adult cardiologists with an “interest” in GUCH
This training would permit an adult cardiologist to share management of some grown-up patients with congenital heart disease. The cardiologists interested in providing such a service are likely to have already developed expertise in echocardiography and non-invasive imaging. The clinics in district general hospitals could be run by the “cardiologist with an interest”, or as a joint clinic with a regional specialist as part of an outreach clinic service. The “cardiologist with an interest” would not carry out cardiac catheterisation in this group of patients. This type of joint care would improve the quality of service in a number of situations such as in relatively low risk pregnancies where local delivery is planned and communication with the obstetrician would be better.
The training for the “cardiologist with an interest” should have a degree of flexibility, as the specialists in the unit for grown-ups with congenital heart disease would ultimately decide the level of care in an individual district general hospital setting. In addition to the six months as part of their adult training, further training in the care of grown-ups with congenital heart disease is recommended. This could take the form of attending the regional specialist clinic or participating in the outreach clinic. A minimum of 24 such clinics over a limited period, such as two years, would be needed. A formal attachment to the grown-up congenital regional unit would significantly shorten the training process. Each regional unit would need to make arrangements and lines of communication appropriate to the local needs and interests. The underlying principle is that the regional centre must be aware of the patients in the district general clinics, and clear lines of communication and a good working relationship are needed to ensure the combination of adequate specialist input into decisions with convenience to patients.
Surgical training
The surgeons who operate on grown-ups with congenital heart disease need expertise and training in both adult and paediatric cardiac surgery. Ideally, they should continue to obtain exposure to both types of surgery, thus preserving continuity and expertise. Appropriate decision making requires knowledge and collation of information from different investigations, including cardiac catheterisation, transthoracic and transoesophageal echocardiography, and magnetic resonance imaging. The surgical trainee should become familiar with these tests. Close interrelation and joint meetings with specialist physicians and between consultants and junior staff is vital.
Current specialist training in paediatric cardiac surgery requires two years intensive training, starting in the fifth and sixth years of the six year common training scheme. At present, all surgeons specialising in paediatric cardiac surgery will have completed their training in surgery for acquired heart disease. In the future, it is likely that cardiac surgeons will not continue to practice in both areas. This is likely to produce problems for training of surgeons able to care for grown-ups with congenital heart disease. It is envisaged that specialised centres will have two surgeons or more. In certain circumstances, two surgeons would operate together, particularly for patients with the most complex conditions.
Training programmes for the cardiac surgeon wishing to operate on grown-ups with congenital heart disease will need to be individualised. He/she must be prepared to leave the region for special training. Postgraduate deans need to be aware of the problems and be flexible.
Nursing training
In addition to nursing experience in adult or paediatric cardiology, additional on-going education is required. Training must include instruction in:
-
Basic physiology and anatomy of congenital cardiac malformations.
-
Understanding of effect of cyanosis and pulmonary hypertension.
-
Nursing adults.
-
Problems of adolescents and general advice required.
-
General issues affecting acquired cardiovascular disease.
-
Particular postoperative problems.
-
Special problems affecting nursing and outcomes in adult congenital heart disease.
Rotation of nursing staff in adult and paediatric areas ensures acquisition of useful, if not vital, experience and is recommended. Experience has shown this is difficult to arrange. The nursing hierarchy needs to be flexible and make arrangements for the individual.
Training for the allied specialities
There are support specialities, such as radiology, intensive care, anaesthesia, and magnetic resonance imaging, which require training and experience in congenital cardiac disease. This depends on centralisation of patients and resources to ensure that such specialists acquire the necessary experience. They can only receive this in a specialist unit, which must accept responsibility and initiate training opportunities.
DATABASE/RECORD KEEPING
It is currently difficult to identify and track grown-ups with congenital heart disease in the UK. This has hampered the development of a clinical service and continues to be a major issue. The development of regional and specialist databases using agreed terminology is essential. Physicians and surgeons should collaborate rather than using the current approaches, which separate the profession inappropriately.
Recent developments, such as the UK Central Cardiac Audit Database (www.ccad:compuserve.com) have demonstrated the feasibility of a national database. The current scope will need to be extended for congenital heart disease, and this has considerable implications for funding. Nevertheless, the authors of this report feel strongly that the availability of a national registry and a unit database as a mechanism for recording of accurate valid information is mandatory for the specialised unit. It should be regarded as a major priority. All patients transferred to adult care should be in a national registry as well as the unit’s database. Trusts accepting responsibility for such specialised units should accept the need for funding, as should additional funding sources such as supraregional service development. Availability of the resulting data at national level would help optimise patient care, develop evidence based protocols for treatment, improve audit, introduce and assess research and innovative approaches to treatment, and facilitate the development of planned services.
RECOMMENDATIONS FOR PROVISION OF SERVICES
General recommendations
The level of care for grown-ups with congenital heart disease in the UK is unsatisfactory at the present time. Patients are often managed as “special cases” in children’s units, or by adult cardiologists with varying degrees of expertise and input from local paediatric cardiologists. The establishment of a national service with a few dedicated specialist units is required for this population which is steadily increasing but small in numbers. The aim of this report is to propose and promulgate such a framework for a national service and to encourage clinicians, administrators and the Department of Health to recognise the needs of patients and ensure that those who have special needs are managed in an appropriately funded specialist unit with adequate resources. The following structure is suggested:
Patients should be transferred to appropriate adult care at around the age of 16 years.
All previous data should be available at transfer, particularly operation/intervention reports.
Paediatric cardiologists should be discouraged from retaining patients in the paediatric environment after the age of 16 years. Consideration must be given to the mental age and maturity of the individual patient. Provision should be made for excellence and care to match that delivered in childhood.
The level of care needs to be defined at the visits to the transitional clinic or initial outpatient clinic, and this will depend on the condition of the patient and diagnosis as well as local geography, outreach clinics, and the availability of cardiologists with an interest and appropriate training in the district general hospital. The general practitioner needs to be clear on the recommended route of referral and the plan for management. The patient also needs to be informed about his/her planned care. There is a case for most patients being seen at least once in the specialised unit within or outside region.
Each unit for paediatric cardiology should have available a regional service for grown-ups with congenital heart disease, staffed by specialists, with the outpatient and inpatient facilities already described. It should not be obligatory to refer all patients within region and particular conditions may require special expertise which may only be available elsewhere. The specialist unit of choice may be outside region (six recommended).
Complex congenital cardiac surgery for grown-ups with congenital heart disease (table 2) must be further centralised in specialised units with a minimum of 50 cases per annum, thus creating some “supra or outside regional units”. The 50 cases should be those in table 2 and not include primary aortic valve replacement or closure of atrial septal defects. Regional units with surgeons, trained and maintaining a practice in paediatric congenital cardiac malformations, which could not attain such numbers of adult cases, may continue to operate on less complex lesions.
Intervention and electrophysiology should be centralised, ideally dealing with a minimum of 40 cases per annum. The skilled practitioners may be required to share their expertise between specialist units until more specialists are available.
Complex conditions should be managed in the specialised unit. Less complex patients should receive shared care, with good communication between the local or regional medical team and the specialised unit. It is logical that the framework for referral centres for grown-ups with congenital heart disease should be related to the established active units for paediatric cardiology and surgery.
The number of fully staffed specialised units providing all expertise required and fully funded requires discussion with the Department of Health. The site and size of these units should be in line with the recommendations from the Department of Health Paediatric and Congenital Cardiac Services Review Group, co-chaired by James Monro and David Hewlett.
COMPOSITION OF THE WORKING GROUP
Chairman
Professor Jane Somerville, Emeritus Professor of Cardiology, Imperial College School of Medicine and Consultant Cardiologist, Grown-Up Congenital Heart Unit, Middlesex Hospital/UCL, London
Members
Mr Michael Cumper, Trustee, GUCH Patients’ Association. GUCH Patient Representative
Professor John Deanfield, Professor of Cardiology, Institute of Child Health, University College London and Director of Grown-Up Congenital Heart Unit, Middlesex Hospital/UCL, London
Professor Stewart Hillis, Professor of Cardiology, Department of Cardiology, Western Infirmary, Glasgow
Dr Stewart Hunter, Emeritus Consultant in Paediatric Cardiology, The Freeman Hospital, Newcastle
Mr Darryl Shore, Consultant Paediatric & Adult Cardiac Surgeon, The Royal Brompton & Harefield NHS Trust, London
Dr Graham Stuart, Consultant Paediatric Cardiologist and Director of Grown-Up Congenital Heart Disease Service, Bristol Royal Hospital for Sick Children/Bristol Royal Infirmary
Mr Victor Tsang, Consultant Cardiothoracic Surgeon, Grown-Up Congenital Heart Unit, Middlesex Hospital/UCL, London and Great Ormond Street Hospital for Sick Children, London
Nurse advisors
Ms Gillian Jackson, Children’s Rheumatology Nurse Specialist, Leeds General Hospital (Formerly Sister, Children’s Cardiac Intensive Care Unit, The Yorkshire Heart Centre, Leeds General Infirmary, Leeds)
Ms Adelaide Tunstill, GUCH Nurse Specialist, Grown-Up Congenital Heart Unit, Middlesex Hospital, London
Co-opted external advisors
Professor R H Anderson, Professor of Paediatric Cardiac Morphology, Cardiac Unit, Institute of Child Health, University College London and President of the British Paediatric Cardiac Association
Dr John O’Sullivan, Consultant Paediatric Cardiologist, The Freeman Hospital, Newcastle
Dr Carole Warnes, Adult Congenital Heart Disease Unit, Mayo Clinic, Rochester, Minnesota, USA
Dr Gary Webb, Adult Congenital Heart Specialist Unit, Toronto Hospital, Canada
Report production
Ms Sue Stone, Grown-Up Congenital Heart Research Co-ordinator, Oxford
Lay summary
Progress in medical proficiency over 50 years has resulted in patients with complex and severe congenital heart disease surviving to adulthood. Children with congenital heart disease have been well provided for within the National Health Service when compared to the level of service available to them once they become adults. They then become a new medical group of Grown-Up Congenital Heart (GUCH) patients.
Cardiologists who have cared for them as babies and children are now faced with a patient who no longer fits into a child’s environment. Their issues are of an adult nature and are without enough cardiologists experienced in their needs. This transition of care to an adult environment is important and requires skill and experience.
These patients are growing in number although many can be considered cured despite the scars on their chests. The special group of complex patients are in need of cardiac services that are familiar with their congenital problems as well as those of the adult.
Specialised services are limited and these patients, especially those with complex conditions, are in danger of not receiving the specialist attention that they need to survive or avoid disability. Patients do not know where to go and doctors are unaware of special needs, often reluctant to refer out of local region.
The GUCH Patients’ Association is concerned and knows their medical population is small, needing only a few well staffed and funded units. Such units should work with regional units and district outpatient services for the convenience of patients. There are many problems other than with the heart itself; both medical and lifestyle issues require informed advice and management which are difficult to find.
The service is currently growing by force of demand and is not being managed effectively as a service for the country as a whole. It is patchy and varies greatly and there are continued difficulties in accessing expertise.
This report outlines the problems that must be faced in recognising that the country needs a structured service with varying levels of expertise and an ease of referral between those levels. All relevant health care workers need to be informed as to the dangers that might be present in complex cases as well as how to identify those who are not “at risk”.
The problem must be solved by meeting the needs of the patients. This will be achieved by providing the right number of recognised, organised cardiac units staffed by properly trained specialists and informing the whole medical profession of the importance of correct referral and treatment for adults with congenital heart disease.
Acknowledgments
We wish to thank Tom Quinn at the Department of Health for advice on nursing issues, Dr Andy Webb, intensivist at the Middlesex Hospital/University College London, who read and advised on the section on intensive care, and Dr Patrizia Presbitero who provided advice on pregnancy and contraception.
REFERENCES
Footnotes
-
↵* For composition of Working Party see end of article