Article Text

Abstract
The European Paediatric Pulmonary Vascular Disease (PVD) Network is a registered, non-profit organisation that strives to define and develop effective, innovative diagnostic methods and treatment options in all forms of paediatric pulmonary hypertensive vascular disease, including specific forms such as pulmonary arterial hypertension (PAH)-congenital heart disease, pulmonary hypertension (PH) associated with bronchopulmonary dysplasia, persistent PH of the newborn, and related cardiac dysfunction.
Methods The writing group members conducted searches of the PubMed/MEDLINE bibliographic database (1990–2015) and held five face-to-face meetings with votings. Clinical trials, guidelines, and reviews limited to paediatric data were searched using the terms ‘pulmonary hypertensioń’ and 5–10 other keywords, as outlined in the other nine articles of this special issue. Class of recommendation (COR) and level of evidence (LOE) were assigned based on European Society of Cardiology/American Heart Association definitions and on paediatric data only, or on adult studies that included >10% children.
Results A total of 9 original consensus articles with graded recommendations (COR/LOE) were developed, and are summarised here. The topics included diagnosis/monitoring, genetics/biomarker, cardiac catheterisation, echocardiography, cardiac magnetic resonance/chest CT, associated forms of PH, intensive care unit/ventricular assist device/lung transplantation, and treatment of paediatric PAH.
Conclusions The multipaper expert consensus statement of the European Paediatric PVD Network provides a specific, comprehensive, detailed but practical framework for the optimal clinical care of children with PH.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Video abstract
Pulmonary hypertensive vascular disease (PHVD) is a fatal disease characterised by pulmonary vascular remodelling, leading to elevated pulmonary arterial pressure, right ventricular dysfunction, left ventricular compression and consequently heart failure.1–6 Despite significant advances in pulmonary arterial hypertension (PAH)-targeted therapies, survival of children and adults with idiopathic PAH and other forms of group 1 pulmonary hypertension (PH), such as persistent PAH after repair of congenital heart disease (CHD), remains poor.7–12 Morbidity and mortality of paediatric PH represent substantial and growing healthcare burden:12–15 From 1997 to 2012, shifts in case mix toward paediatric PH not associated with CHD, non-cardiac procedures and care in urban teaching hospitals have been noted in a recent retrospective study in the USA.15 Based on a separate analysis of the period 2000–2009, the number of PH-related hospitalizations of children is increasing, and the overall mortality for PH-related hospitalizations is greater than that for hospitalizations not associated with PH (5.7% vs 0.4%; odds ratio: 16.22 (95% CI 14.8% to 17.8%), p<0.001).16 Nevertheless, PH-associated mortality has been decreasing over the recent years in children16 ,17 and adults9 ,10 (box 1).
Rationale for an expert consensus statement on paediatric pulmonary hypertension
Diagnostic and therapeutic strategies in children with pulmonary hypertension (PH) are markedly influenced by unique features of the pulmonary circulation in childhood (developmental biology) and certain paediatric diseases that are commonly associated with PH.
A new World Symposium on Pulmonary Hypertension (WSPH) classification18 was published in December 2013 and slightly modified in the new 2015 European Society of Cardiology European Respiratory Society guidelines on the diagnosis and treatment of PH—a document that mainly focuses on clinical care in adults.
Yet, we felt that comprehensive, detailed but practical recommendations addressing the specifics of PH and pulmonary vascular disease in children are lacking.
Recent randomized controlled trials on mono or combination PH therapy have enrolled a substantial number of children, or—more recently—have been exclusively designed to study PH in children (eg, STARTS-1, -2).
Analyses of several paediatric patient registries (TOPP, REVEAL, COMPERA KIDS) and basic science and clinical advances have led to multiple high-impact publications in the past 10 years.
The unique features of paediatric PH were—for the first time—recognized at the 2013 WSPH in Nice, resulting in a brief 10-page document on paediatric PH.19 In addition, the first specific paediatric pulmonary hypertensive vascular disease classification (Pulmonary Vascular Research Institute, Panama) published in 201120 is currently undergoing revisions and modifications, as practicing PH doctors aim to apply the detailed paediatric-specific classification. Hence, this multipaper expert consensus statement on the paediatric PH by our network is timely indeed.
Objectives of the expert consensus statement of the European Paediatric Pulmonary Vascular Disease (PVD) Network
We were seeking to develop a framework that better defines the course of paediatric PH, identifies current gaps in our knowledge and provides a consensus statement with practical recommendation on how to best manage paediatric PH in diverse settings, acknowledging that most recommendations will have level of evidence (LOE) B or C. The 10 documents, including this executive summary, do not comprehensively review the pathobiology and clinical findings of paediatric PH, but rather contain practical recommendations for healthcare providers treating children and adolescents with different forms of PH.
The objectives of this multipaper consensus statement were (1) to discuss the most recent classifications of PH: World Symposium, Nice, 2013; progressive post-haemorrhagic ventricular dilatation (PPHVD) pulmonary vascular resistance index Panama 2011; European Society of Cardiology (ESC)/European Respiratory Society (ERS), 2015; (2) to summarise clinical study results and their limitations, (3) to provide graded, evidence- and expert-based recommendations for the diagnosis and treatment of infants, children and adolescents with PH (including CHD/Eisenmenger syndrome), according to the grading system provided by American Heart Association (AHA) and ESC, (4) to address features specific to PH forms in childhood, (5) to define the multiple gaps in our knowledge on paediatric PH, (6) make suggestions on future trial design and (7) to discuss emerging PH therapies (safety and efficacy).
Methodology
The European Paediatric PVD Network
The European Paediatric PVD Network is a registered non-profit organisation that is independent of any medical–scientific society and industry. The network strives to define and develop effective, innovative diagnostic methods and treatment options in all forms of paediatric PHVD, including specific forms such as PAH–-CHD, PH associated with bronchopulmonary dysplasia (BPD), persistent PH of the newborn (PPHN) and related cardiac dysfunction. In order to achieve these objectives, an interdisciplinary writing group (WG) was assembled to develop a multipaper expert consensus statement that is being published in this special issue of Heart.
Composition of the PVD Network's WG ‘Expert Consensus Statement on the Diagnosis and Treatment of Paediatric Pulmonary Hypertension’
The WG members were recruited from Austria, Germany, Finland, France and the UK. The WG consists of 23 paediatricians (with subspecialty expertise and board certifications in paediatric cardiology, critical care and/or neonatology), a clinical physiologist and a thoracic transplant surgeon. The WG started within the German Paediatric PVD Network, a newly founded WG of the German Society of Paediatric Cardiology (DGPK) in 2013, and then quickly evolved into the multinational European Paediatric PVD Network that now publishes the expert consensus statement. The majority of the 24 authors of the PVD network's WG are also members of the WG of ‘PH and heart failure’ of the ‘Association for European Paediatric and Congenital Cardiology’ (AEPC). Georg Hansmann is chair and Christian Apitz is co-chair of the according WG of the European Paediatric PVD Network.
Special features of this expert consensus statement—the multipaper approach leading to recommendations for the practicing physician and specialised PH doctor
Conventional consensus statements or guidelines published by scientific societies tend to be >40-page documents attempting to cover all aspects of an often very heterogeneous disease, and thus may—at times—become too unwieldy to fully address the needs of the practicing healthcare providers and their patients, immediate relatives and insurance companies. WGs are usually large and—due to the time-consuming voting, writing and editing processes—very relevant original publications of the preceding 12–18 months often cannot be included in such a large document before it is published.
We followed a novel approach and created small taskforces within an interdisciplinary international multiexpert WG, to develop nine individual papers by clinical topic plus this executive summary and grouped the manuscripts in a special issue entitled ‘paediatric pulmonary hypertension’. All 10 papers include graded recommendations according to the grading system provided by the ESC and the AHA. All articles underwent a rigorous peer review process (see below).
Within the multipaper concept, we divided the topics as they relate to the ‘syndrome paediatric PH’ by the clinical scenario they usually occur in real life, that is, general recommendations on diagnosis/monitoring;21 specific diagnostics tools, that is, biomarker/genetics;22 cardiac catheterisation;23 echocardiography;24 and cardiac magnetic resonance/CT.25
Moreover, we addressed two disease-specific, complex and common patient groups separately: (1) PH/PHVD associated with CHD, including recommendations that are relevant for both children and adolescents/adults with PAH-CHD,26 and (2) PPHN and BPD/chronic lung disease in infancy.27
Finally, detailed recommendations on therapy are given in two documents: (1) treatment of acute PH in the intensive care unit, including ventricular assist device (VAD)/extracorporeal membrane oxygenation and lung transplantation (LuTx),28 and (2) comprehensive recommendations on mid- to long-term treatment of PH/PHVD in the inpatient and outpatient setting, including pharmacotherapy, catheter interventions and surgery.29
Literature search, grading system of recommendations, voting and review process
Literature search
Computerized searches of the PubMed/MEDLINE bibliographic database were conducted for the time period 1990–2015. Clinical trials, guidelines, and reviews limited to paediatric data were searched using the terms ‘pulmonary hypertensioń’ and 5–10 other keywords, as outlined in each of the 10 articles of this special issue ’Expert Consensus Statement on the Diagnosis and Treatment of Paediatric Pulmonary Hypertension’. The primary focus of this manuscript is on group 1 PH, according to the World Symposium on Pulmonary Hypertension (WSPH) classification (Nice, 2013)18 that was recently slightly modified in the ‘ESC/ERS Guidelines on the Diagnosis and Treatment of Pulmonary Hypertension’.30
Class of recommendation (COR), level of evidence (LOE)
The recommendations relate to the grading system for class of recommendation (COR) and LOE currently proposed by the ESC and the AHA (COR, table 1; LOE, table 2) and was based on paediatric data only (paediatric studies, or adult studies enrolling >10% children). The grading and voting process is described further below. Within this executive summary, only the recommendations listed in each table #1 of the 9 subtopic consensus statements are listed. A full list of references can be found in the individual 9 subtopic articles. Importantly, healthcare providers must adhere to the medication labelling and follow future drug recommendations/warnings potentially published by the European Medicines Agency (EMA) and the US Food and Drug Administration (FDA) when transforming these recommendations into clinical practice.
Classes of recommendations
Levels of evidence
Voting process
The WG held five face-to-face meetings to discuss the individual topics and conduct the voting on the wording of the recommendations and the grading (COR, LOE) thereof (tables 1 and 2). The according meetings were conducted on 28 January 2014 in Bad Nauheim, Germany; on 28 July 2014 in Hannover, Germany; on 4 October 2014 in Weimar, Germany; on 21 May 2015 in Prague, Czech Republic; and on 6 June 2015 in Weimar, Germany. Of the 144 graded recommendations, 65 were class (COR) I, 72 were class II (39 COR IIa, 33 COR IIb); and 7 determined as class III (COR III, no benefit or harm). Three recommendations were LOE A, 41 were LOE B and the majority, that is, 100, were stratified as LOE C, due to the lack of randomized controlled studies.
Peer review process
Each manuscript of the multipaper expert consensus statement has been peer reviewed by at least two anonymous external experts according the journal's standardised review process for original articles and—in addition—by two anonymous experts selected by the International Society of Heart and Lung Transplantation (ISHLT) scientific board.
Endorsement process (ISHLT, DGPK)
The ISHLT was actively involved in the peer review process as outlined above and endorsed the first five manuscripts on 3 September 2015 and the final five manuscripts on February 9, 2016. The DGPK, that is, the society for paediatric and congenital cardiology in Austria, Germany and Switzerland, endorsed the multipaper expert consensus statement on January 7, 2015 (box 2).
Definitions
Pulmonary Hypertension (PH)
mPAP ≥25 mm Hg in children >3 months of age at sea level
PAH
mPAP ≥25 mm Hg
PCWP <15 mm Hg
PVR index >3 WU×m2
Idiopathic Pulmonary Arterial Hypertension (PAH)
PAH with no underlying disease known to be associated with PAH
Hereditary PAH
PAH with no underlying disease but with positive family history or positive genetic testing
Pulmonary hypertensive vascular disease
For biventricular circulations:
mPAP ≥25 mm Hg and PVR index >3 WU×m2
For circulations with cavopulmonary anastomosis (eg, Fontan physiology):
mean TPG >6 mm Hg (calculate mPAP minus mLAP or PCWP) or PVR index >3 WU×m2
Detailed haemodynamic definitions of PH (eg, precapillary vs postcapillary PH, value of the diastolic transpulmonary pressure gradient) by the European Paediatric Pulmonary Vascular Disease Network are presented in ref. 23.
mPAP, mean pulmonary artery pressure; mLAP, mean left atrial pressure; PAH, pulmonary artery hypertension; PCWP, pulmonary capillary wedge pressure (syn. PAWP, pulmonary artery wedge pressure); PVR, pulmonary vascular resistance; and TPG, transpulmonary pressure gradient; WU, Wood units.
Summary of graded recommendations (COR, LOE) by clinical topic
See tables 3⇓⇓⇓⇓⇓⇓⇓⇓–11 and figures 1⇓⇓⇓–5 for summary of graded recommendations.
Recommendations on diagnosis, monitoring and outpatient care in children with suspected or confirmed PH/PPHVD21
Recommendations on the use of genetic testing and biomarkers in children with PH.22
Recommendations on haemodynamic assessment and acute pulmonary vasoreactivity testing in the evaluation of children with pulmonary vascular disease23
Recommendation on transthoracic echocardiography (TTE) in paediatric pulmonary hypertension24
Recommendations on the use of cardiac magnetic resonance and computed tomography in children with suspected or confirmed PH/ PPHVD25
Recommendations on the evaluation and management of PH in children and adolescents with CHD (CHD–PAH, CHD–PPHVD)26
Recommendations for supportive measures and pharmacotherapy in PPHN and PH associated with BPD/nCLD27
Recommendations on the therapy of acute PH in the paediatric intensive care unit28
Recommendations on treatment of children with paediatric pulmonary hypertension29
Writing group disclosures: conflicts of interests and relationships with industry

Diagnostic algorithm for a child or adolescent with suspected pulmonary hypertension. BPD, bronchopulmonary dysplasia; CLD, chronic lung disease; CHD, congenital heart disease; CTEPH, chronic thromboembolic pulmonary hypertension; CXR, chest X-ray; HPAH, hereditary pulmonary arterial hypertension; IPAH, idiopathic pulmonary arterial hypertension; PCH, pulmonary capillary haemangiomatosis; PH, pulmonary hypertension; PVOD, pulmonary veno-occlusive disease; VQ, ventricular-perfusion.

Determinants of risk in paediatric pulmonary hypertensive vascular disease. The variables listed distinguish between lower and higher risk. The intermediate risk group is broad and not specifically defined. Overall, these determinants have only level of evidence C due to sparse or lack of paediatric data. Healthcare providers may include here PVR/SVR ratio, the 6 min walk distance and the max. oxygen consumption (VO2 max.) obtained during cardiopulmonary exercise testing as risk variables; however, it is unclear where exactly the cut-off values should be set. One must also note that most of these variables have been validated mostly for IPAH and the cut-off levels used above may not necessarily apply to other forms of PAH. Furthermore, the use of approved therapies and their influence on the variables should be considered in the evaluation of the risk. BNP, brain natriuretic peptide; CI, cardiac index (syn. Qs); IPAH, idiopathic pulmonary arterial hypertension; mPAP, mean pulmonary artery pressure, mRAP, mean right atrial pressure; NT-proBNP, N terminal pro BNP; PVRi, pulmonary vascular resistance index; RA, right atrium; RV, right ventricle; SVRi, systemic vascular resistance index; WHO, World Health Organisation. Modified from McLaughlin and McGoon.31

Algorithm for management of patients with congenital heart disease associated with PAH/PPVD and congenital shunt lesions. The indication for invasive diagnostics and eligibility for surgery/operability by comprehensive right and left heart catheterisation includes basic evaluation and AVT, the latter especially in the grey zone of forecast uncertainty. Modified from: Lopes AA and Barst R and the PVRI PAH-CHD taskforce (PVRI website; published on 26 September 2013). ASD, atrial septal defect; AVT, acute vasodilative testing; CHD, congenital heart disease; PDA, patent ductus arteriosus; PAH, pulmonary arterial hypertension; PH, pulmonary hypertension; pre OP, preoperatively; PVR, pulmonary vascular resistance; PVRI, pulmonary vascular resistance index; Qp, pulmonary blood flow; Qs, systemic blood flow; SVR, systemic vascular resistance; WU, Wood units; VSD, ventricular septal defect PAH, pulmonary arterial hypertension.
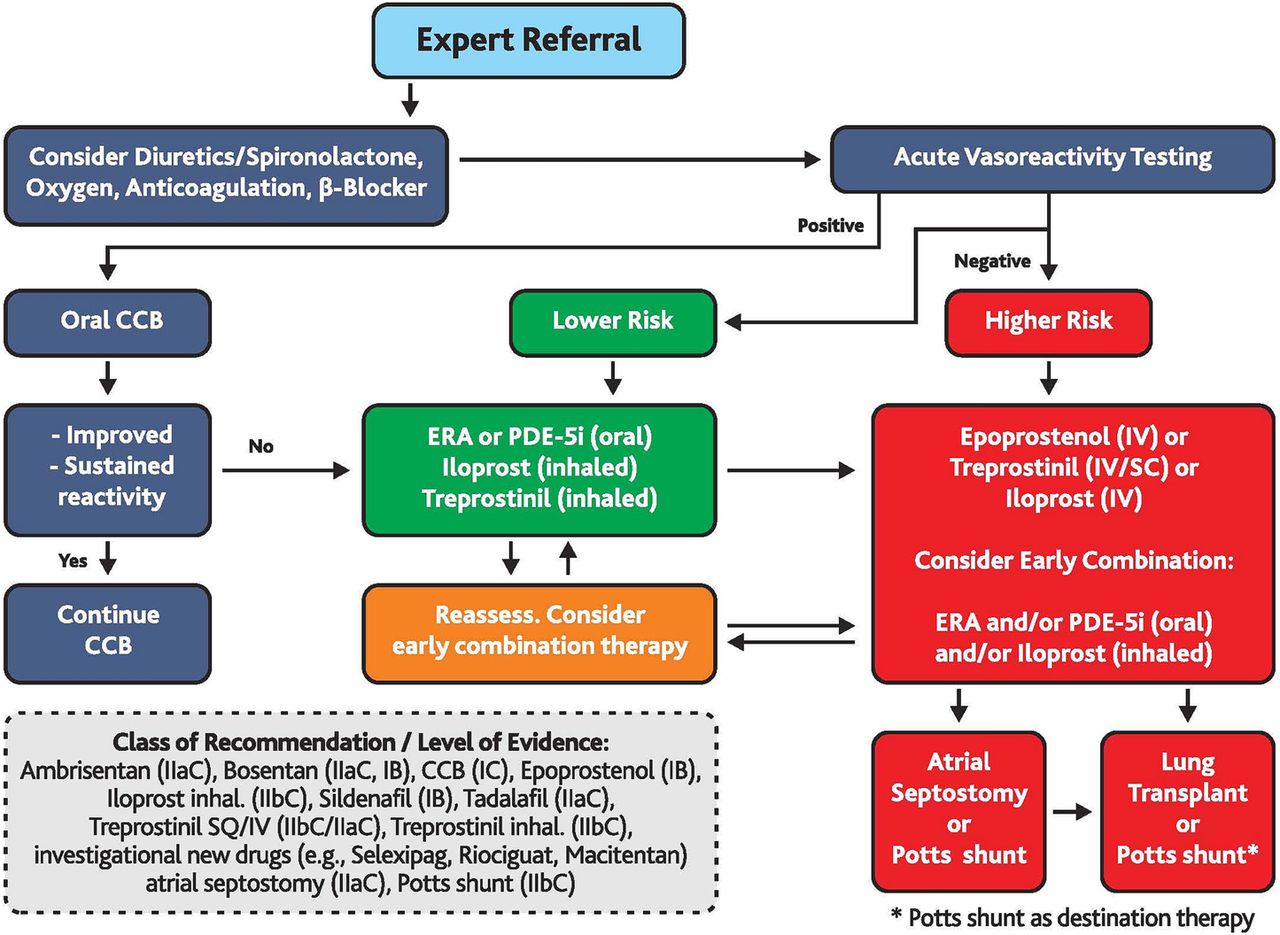
Treatment algorithm for paediatric pulmonary arterial hypertension. This algorithm applies to IPAH HPAH (FPAH). Solid clinical data on the therapy of other forms of PH is limited. The ‘intermediate’ risk group is broad and not specifically defined (see figure 1). Healthcare providers may consider upfront, early or rapid sequence-targeted PAH therapy in ‘intermediate’ risk group (between ‘lower risk’ and ‘higher risk’ in figure 1: ‘Determinants of risk’). Use of all agents is considered off-label in children aside from sildenafil and bosentan (>1-year-old) in Europe. Sildenafil dosing recommendations should follow EMA-approved dosing for children. Bosentan received the following dual grading: COR I, LOE B for children with PAH and Eisenmenger syndrome, and COR IIa, LOE C for children with PAH without Eisenmenger syndrome. CCB, calcium channel blocker; COR, class of recommendation; ERA, endothelin receptor antagonist; EMA, European Medicines Agency; HPAH, hereditary pulmonary arterial hypertension; inh., inhalation; IPAH, idiopathic pulmonary arterial hypertension; IV, intravenous; LOE, level of evidence; PDE-5i, phosphodiesterase 5 inhibitor; PH, pulmonary hypertension;; PAH, pulmonary arterial hypertension; SC, subcutaneous. Modified and expanded from Ivy et al.19

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Treatment algorithm for combination therapy in PAH (evidenced-based only for adults with PAH, ie, group 1 PH). Bosentan received the following dual grading: COR I, LOE B for children with PAH and Eisenmenger syndrome, and COR IIa, LOE C for children with PAH without Eisenmenger syndrome. The ‘intermediate’ risk group is broad and not specifically defined (see figure 1). (a) Some WHO-FC III patients may be considered high risk (see table 1). (b) In adult PAH, initial combination with ambrisentan plus tadalafil has been shown to be superior to initial monotherapy with ambrisentan or tadalafil in delaying clinical failure. (c) Intravenous epoprostenol should be prioritised as it has reduced the 3 months rate for mortality in high-risk adult PAH patients also as monotherapy. (d) Consider also balloon atrial septostomy. Modified from Galie et al.30 CCB, calcium channel blockers; COR, class of recommendation; DPAH, drug-induced PAH; HPAH, heritable PAH; IPAH, idiopathic PAH; i.v., intravenous; LOE, level of evidence (according to European Society of Cardiology and American Heart Association). PAH, pulmonary arterial hypertension; PCA, prostacyclin analogues; WHO-FC, WHO functional class.
Limitations of the multipaper expert consensus statement on paediatric PH
We acknowledge that most LOE of our recommendations on paediatric PH, are B or C, since only very few randomised controlled trials have been conducted so far due the heterogeneity of what is still considered a rare—but underdiagnosed—disease in the so-called developed world. Thus, we called this special issue ‘Expert Consensus Statement’ rather than ‘Guidelines’. We do strongly feel—however—that the previous PH documents provided by adult cardiology or respiratory societies or the WSPH, while improved, do not reflect to a satisfactory extent the specific complexity of paediatric PHVD and hence developed this consensus statement (box 3).
Challenges and future directions of the European Paediatric Pulmonary Vascular Disease Network
Identification of valid treatment goals in paediatric PAH.6 ,32–35
Regulatory requirements, patient recruitment and retention, clinical trial endpoints for paediatric PAH trials.33 ,34
Need to conduct multicentre studies and establish new registries for paediatric pulmonary hypertension.14 ,34
Initiation of a prospective multicentre study on early combination therapy in paediatric including a comparative group (early combined dual or triple combination, rapid sequence of two agents).
When and how to perform a Potts shunt procedure36 (surgery, intervention?) for advanced PAH and how to combine this pressure-unloading shunt with combination pharmacotherapy?
Initiation of investigator-initiated pilot and/or industry-sponsored phase 2/3 studies on the safety and efficacy of new compounds recently published/approved for adult PAH (macitentan, riociguat, selexipag, treprostinil).29
Conclusions
This multipaper expert consensus statement of the European Paediatric PVD Network provides a specific, comprehensive, detailed but practical framework for the optimal clinical care for children with PH/PHVD. Additional patient registries and prospective, controlled and randomised studies on the diagnosis and treatment of PH in children are urgently needed to move on from frequently experience-based towards mostly evidence-based recommendations.
Web link
European Paediatric Pulmonary Vascular Disease Network http://www.pvdnetwork.org
Key messages
What is already known on this subject?
Pulmonary hypertension (PH) in neonates, infants, children and adolescents is a complex condition that may be associated with diverse cardiac, pulmonary and systemic diseases, and contributes to significant morbidity and mortality. However, current approaches to caring for paediatric patients with PH have been limited by the lack of consensus recommendations from experts in the field of paediatric PH.
What might this study add?
The European Paediatric Pulmonary Vascular Disease (PVD) Network is a registered, non-profit organisation that strives to define and develop effective, innovative diagnostic tools and treatment options in all forms of paediatric pulmonary hypertensive vascular disease (PHVD), including specific forms such as pulmonary arterial hypertension–congenital heart disease, PH associated with bronchopulmonary dysplasia, persistent PH of the newborn, and related cardiac dysfunction. In order to achieve these objectives, a multipaper expert consensus statement was developed to provide comprehensive and practical recommendations.
How might this impact on clinical practice?
This multipaper expert consensus statement of the European Paediatric PVD Network provides—for the first time—a specific, comprehensive, detailed but practical framework for the optimal clinical care of children with PH/PHVD.
Acknowledgments
Chair and co-chair would like to thank all writing group members for their voluntary contributions and result-driven dedication to this project. We very much appreciate the support from ISHLT and DGPK leadership, the editors and editorial board of Heart, as well as Lindsey Fountain and Eleanor Naylor, and the editorial staff at BMJ Publishing.
References
Footnotes
This manuscript is a product of the writing group of the European Paediatric Pulmonary Vascular Disease Network (Writing Group Chair: G Hansmann, Writing Group Co-Chair: C Apitz). ISHLT, International Society of Heart and Lung Transplantation; DGPK, German Society of Paediatric Cardiology.
Contributors The contributor statement can be found in table 12.
Funding This Heart supplement was produced with support from an unrestricted educational grant from Actelion Pharmaceuticals Germany GmbH, Bayer Pharma AG, and Pfizer Inc. None of these organisations had any influence on the composition of the writing group or the content of the articles published in this supplement.
Competing interests The European Paediatric Pulmonary Vascular Disease Network is a registered, non-profit organisation that makes every effort to avoid any actual or potential conflicts of interest that may arise as a result of an outside relationship or a personal, professional or business interest of a member of the writing panel. Specifically, all members of the writing group are required to complete and submit a disclosure questionnaire showing all such relationships that might be perceived as real or potential conflicts of interest. All authors filled out and signed a form for disclosure of potential conflict of interests provided by the International Committee of Medical Journal Editors. Chair (GH) and co-chair (CA) of this writing group indicate no conflicts of interests or relationships with industry related to the content of this article. Comprehensive information on conflict of interests, relationships with industry, current grant support of all writing group members can be found in table 12 of this article.
Provenance and peer review Not commissioned; internally peer reviewed.