Article Text

Abstract
Objective To examine the relation between the initial microvascular perfusion pattern, as assessed by intracoronary myocardial contrast echocardiography (MCE), immediately after restoration of TIMI (thrombolysis in myocardial infarction) (TIMI) grade 3 flow during acute myocardial infarction, and the extent and timing of functional recovery in the area at risk.
Setting Referral centre for interventional cardiology.
Methods Intracoronary MCE was performed 15 minutes after TIMI grade 3 recanalisation of the infarct artery in 25 patients. Segmental myocardial contrast patterns were graded semiquantitatively (0, none; 0.5, heterogeneous; 1, homogeneous). Functional recovery was assessed by echocardiography on days 9 and 42.
Results Among 174 myocardial segments in the area at risk, wall motion recovery on day 9 was observed in 40% of MCE grade 1 segments but there was no significant recovery in grade 0 or 0.5 segments. On day 42, recovery had occurred in 56% of MCE grade 1 segments (p < 0.0001v MCE grade 0 and 0.5; p = 0.0001v MCE grade 1 on day 9), and 22% of MCE grade 0.5 segments (p = 0.02 v MCE grade 0; p = 0.0005 v MCE grade 0.5 on day 9); MCE grade 0 segments did not recover. Negative predictive value in predicting recovery by contrast enhancement was 95% and 89% by days 9 and 42, respectively.
Conclusions Contractile recovery occurs earliest in well reperfused segments. Up to one quarter of segments with heterogeneous contrast enhancement show wall motion recovery within the first six weeks. Myocardial perfusion after recanalisation in acute myocardial infarction, even if heterogeneous, is a prerequisite for postischaemic functional recovery. Thus preservation of acute myocardial perfusion is associated with more complete and early functional recovery.
- acute myocardial infarction
- myocardial contrast echocardiography
- microcirculation
- functional recovery
Statistics from Altmetric.com
Complete patency of the infarct related artery (that is, thrombolysis in myocardial infarction (TIMI) flow grade 31) is an independent prognostic factor in survival after early reperfusion treatment,2 ,3 but does not necessarily result in restoration of adequate myocardial perfusion at the tissue level.4 Failure to achieve adequate microvascular reperfusion (the “no-reflow” phenomenon) has been documented in man during acute myocardial infarction by myocardial contrast echocardiography (MCE)5 ,6 and is consistently associated with impaired recovery of contractile function and a worse clinical outcome.5-11
Most previous studies have used a categorical definition of no-reflow, as opposed to a quantitative approach based upon segmental analysis of perfusion in the area at risk. However, the no-reflow phenomenon is not necessarily homogeneously distributed in the myocardium at risk,11 and functional recovery of the areas with heterogeneous microvascular perfusion has not yet been specifically studied. Furthermore, the time course of functional recovery of these no-reflow areas is not well documented.12
The purpose of this study was to examine the extent and timing of functional recovery of myocardial segments in the area at risk according to initial microvascular perfusion pattern, as assessed by intracoronary MCE immediately after re-establishment of complete patency of the culprit vessel during acute myocardial infarction.
Methods
STUDY POPULATION
Patients with their first acute myocardial infarction admitted less than six hours after the onset of symptoms were screened for inclusion in the study. Myocardial infarction was defined as typical chest pain of more than 30 minutes’ duration, resistant to nitrates, with ST segment elevation ⩾ 0.1 mV in limb leads or ⩾ 0.2 mV in two or more chest leads. The diagnosis was eventually confirmed by a rise in plasma creatine kinase to twice the normal value. Emergency angiography was performed in all patients, either with a view to primary angioplasty or to ascertain patency of the infarct vessel after intravenous thrombolysis. Patients were included only if TIMI grade 3 patency was angiographically demonstrated. Patients with angiographic TIMI grade flow ⩽ 2, haemodynamic instability or shock, ⩾ 50% stenosis of the left main coronary artery, and previous myocardial infarction or coronary artery bypass surgery were excluded, as well as those with significant valvar disease, primary myocardial disease, or aged less than 18 or more than 80 years.
STUDY DESIGN
Cross sectional echocardiography was performed immediately upon admission in the catheterisation laboratory to assess baseline segmental wall motion and delineate the area at risk, defined as the area with dyssynergic segments (that is, hypokinetic, akinetic, or dyskinetic segments). Coronary angiography was done immediately in patients in whom primary angioplasty was intended. In patients treated with thrombolysis, angiography was done at 60 to 90 minutes, to determine the patency of the infarct vessel and perform percutaneous transluminal coronary angioplasty (PTCA) as a rescue procedure if appropriate. MCE was performed 10 minutes after obtaining stable TIMI flow grade 3 in the infarct vessel. Coronary angiography was repeated on day 9 to verify the patency of the infarct related artery. Cross sectional echocardiography on days 9 and 42 allowed serial assessment of recovery of segmental and global contractile function. All patients gave their informed consent, and the protocol was approved by the institution’s ethics committee on human research.
ECHOCARDIOGRAPHIC STUDIES
Initial cross sectional and intracoronary MCE examinations were performed with the patient lying supine, a foam wedge under the right shoulder, using a commercially available echocardiographic system (Sonos 1500, Hewlett-Packard Inc, Camas, Washington, USA) with a 2.5 MHz transducer. MCE was performed by injecting 3 ml of sonicated ioxaglate (Hexabrix 320, Guerbet, France)11 followed by a 3 ml saline flush, separately into the left and right coronary arteries. One contrast injection in each artery was used for each of the four standard echocardiographic views (parasternal long and short axis and apical two and four chamber views). Image recording was initiated 10 seconds before microbubble injection and continued until the disappearance of myocardial contrast enhancement with a constant gain setting, with storage on S-VHS videotapes for off-line analysis. The ECG was monitored continuously.
ECHOCARDIOGRAPHIC DATA ANALYSIS
We used the American Society of Echocardiography left ventricular segmentation, with 16 segments.13 Contrast enhancement was analysed on end diastolic frames, and graded in each segment as 0 for absence, 0.5 for heterogeneous or subepicardial, and 1 for homogeneous and complete enhancement (figs 1 and 2). A mean perfusion score was calculated for each patient by averaging the contrast scores in the area at risk, as previously described.11 A patient was considered to have no-reflow if his mean perfusion score was 0.5. Wall motion was graded using the degree of myocardial thickening and the inward motion of the endocardial border. Each segment was assigned a wall motion grade (WMG): 1 for normal, 2 for hypokinesia, and 3 for akinesia or dyskinesia. Segmental contractile function recovery at day 9 or 42 was defined as a decrease of at least one grade in wall motion. A regional wall motion score index (WMSI) was obtained for each patient by averaging the scores from each segment within the area at risk.
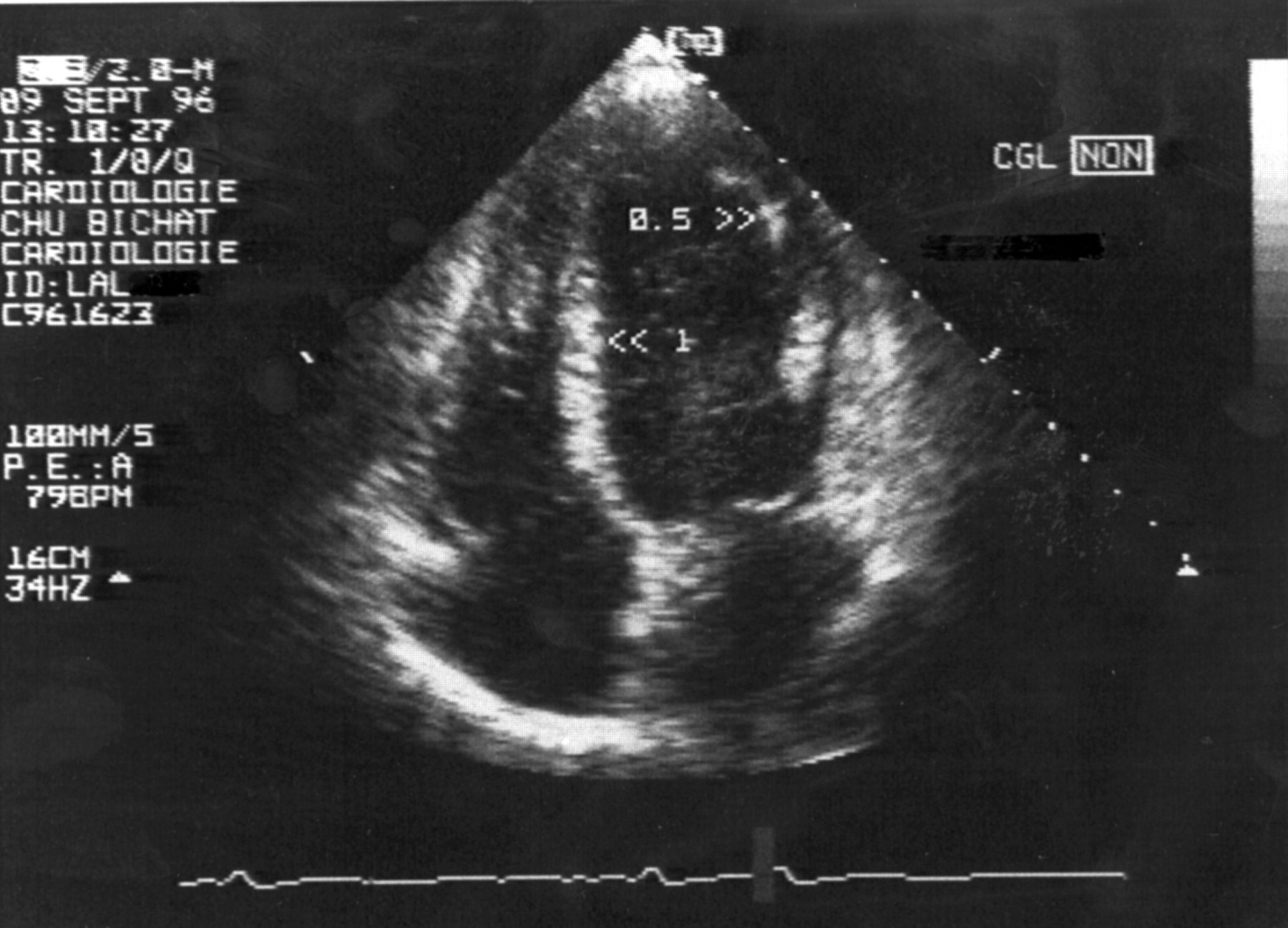
Apical four chamber view obtained by myocardial contrast echocardiography (MCE) in a patient immediately after successful primary angioplasty of an occluded left anterior descending coronary artery. The mid-septal segment is well perfused (MCE grade 1); the apicolateral segment shows only subendocardial perfusion (MCE grade 0.5).
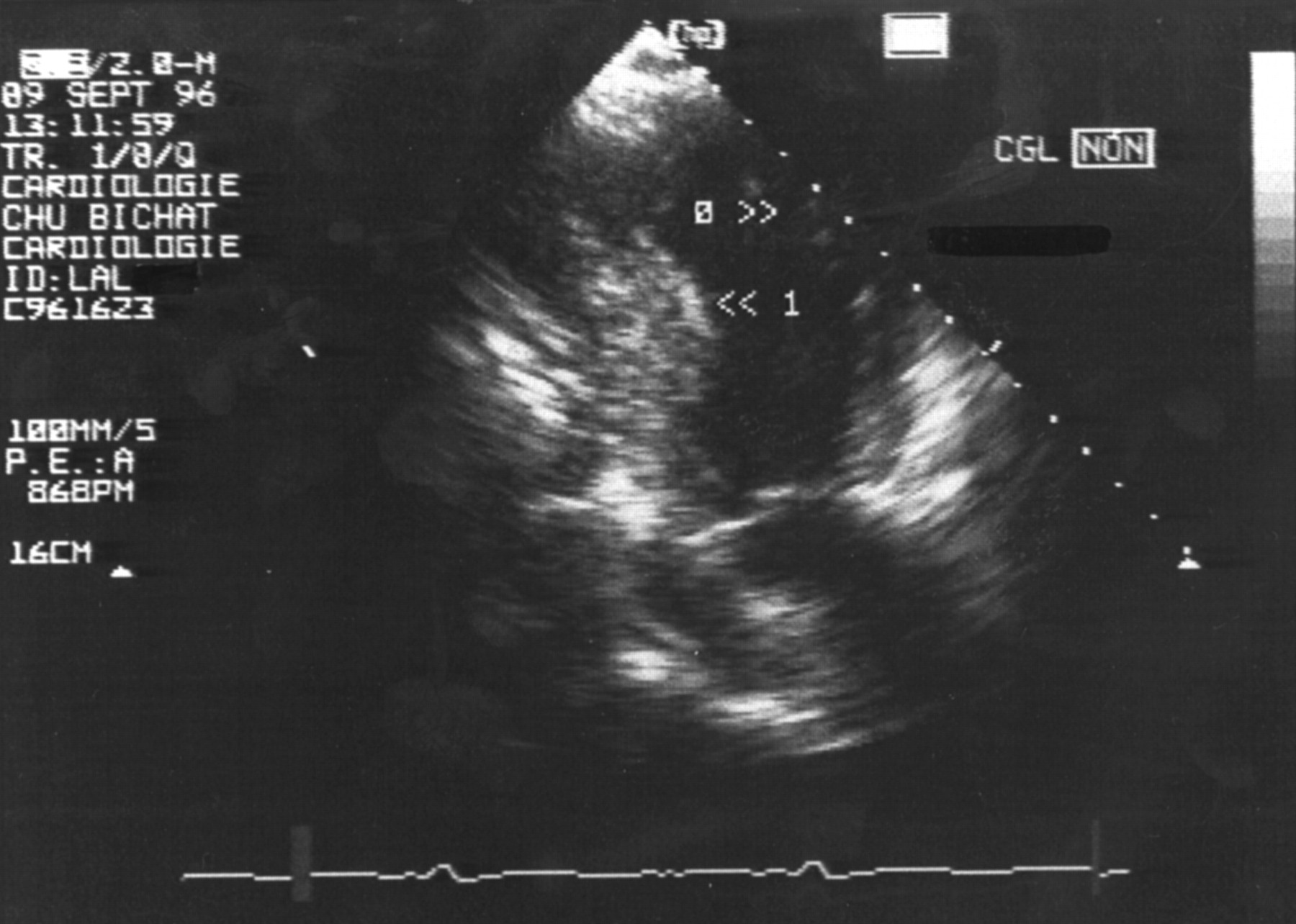
Apical two chamber view of the same patient. The apical segment of the anterior wall has no tissue perfusion (MCE grade 0), whereas the mid-segment of the inferior wall is well perfused (MCE grade 1).
REPRODUCIBILITY OF ECHOCARDIOGRAPHIC DATA
Videotapes were read simultaneously by two experienced observers blinded to clinical and angiographic data. Discrepancies were resolved by consensus reading. The reproducibility of location and intensity of the contrast enhancement grading, as well as of segmental wall motion scoring, was assessed by duplicate reading of 10 randomly selected patients. Reading reproducibility was 84% for contrast enhancement and 85% for segmental wall motion. Discrepancies in contrast intensity and wall motion scoring were never more than one grade.
STATISTICAL ANALYSIS
All values are expressed as mean (SD). Comparisons between groups were performed using factorial or repeated measures analysis of variance (anova) as appropriate. When significant, post-hoc comparisons between groups were performed using Scheffe’s method. A probability (p) value of < 0.05 was considered significant. The χ2 was used for comparisons involving qualitative variables. The correlation between contrast scores and the evolution of regional wall motion score index was assessed using linear regression analysis. As patient values were not normally distributed, comparisons between groups were performed using the Mann–Whitney U test.
Results
Thirty seven patients admitted less than six hours after the onset of acute myocardial infarction fulfilled the inclusion criteria. Ten patients were excluded from the analysis because of poor echogenicity (seven inferolateral and three anterior wall infarctions), and two because of absence of wall motion abnormality precluding delineation of the area at risk. Therefore, data from 25 patients were available for analysis. Twenty patients had undergone successful primary angioplasty, four thrombolysis, and one spontaneous recanalisation of the infarct vessel. Mean (SD) age was 51 (12) years, 22 patients were men and 15 women, and 11 (40%) had multivessel disease. The infarct related artery was the left anterior descending coronary artery in 17 patients, the left circumflex in one, and the right coronary artery in seven. The time from symptom onset to angiographic demonstration of TIMI grade 3 flow was 220 (65) minutes.
Repeat coronary angiography, performed 9 (2) days (range 6 to 14) after admission, showed persistent TIMI grade 3 patency of the infarct vessel in all patients. All patients treated by thrombolysis had > 70% residual stenosis and underwent coronary angioplasty of the culprit lesion. Follow up echocardiography on day 42 was available in 19 patients; the status of six patients was assessed by telephone. All patients had an uneventful recovery at the time of follow up.
MCE PATTERNS IN THE ACUTE STAGE
There were 174 hypokinetic, akinetic, or dyskinetic segments on the baseline cross sectional echocardiogram, an average of 7.4 (2.6) segments in the area at risk per patient (range 3 to 12). Segmental MCE analysis showed the absence of contrast enhancement after ioxaglate injection (grade 0) in 41 segments (23%), patchy or incomplete enhancement (grade 0.5) in 43 segments (25%), and homogeneous enhancement (grade 1) in 90 segments (52%) (p = 0.0001). Among MCE grade 0 segments, 39 (95%) were akinetic or dyskinetic and two (5%) were hypokinetic at baseline; among MCE grade 0.5 segments, the proportions were respectively 98% and 2%; and among MCE grade 1 segments, they were respectively 72% and 28% (p = 0.0001) (fig3).
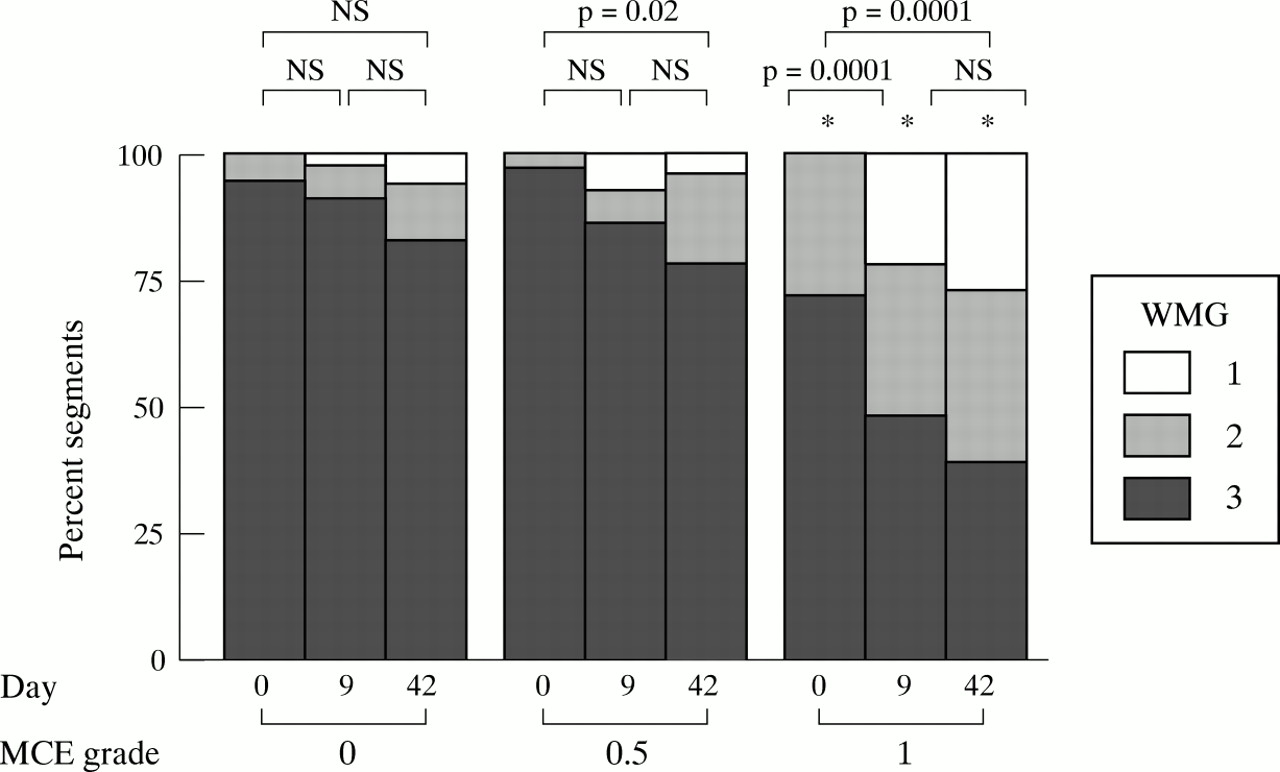
Bar graph showing serial echocardiographic segmental wall motion assessment (at day 0, day 9, and day 42) as a function of acute (day 0) myocardial contrast pattern. MCE, myocardial contrast echocardiography; WMG, wall motion grade. *p = 0.0001 v perfusion grade 0 and 0.5 on the same day
RELATION BETWEEN MCE PATTERNS AND RECOVERY OF SEGMENTAL CONTRACTILE FUNCTION
The initial, day 9, and day 42 segmental wall motion according to the initial myocardial perfusion pattern is shown in fig3. The vast majority (90%) of MCE grade 0 segments remained akinetic or dyskinetic on day 9, as well as 86% of MCE grade 0.5 segments. Conversely, among MCE grade 1 segments, only 48% remained akinetic or dyskinetic, while 22% were normokinetic, and 30% hypokinetic. Similar results were observed on day 42. The echocardiographic wall motion of MCE grade 0.5 and grade 1 segments was significantly improved at six weeks compared with day 0 (fig 3).
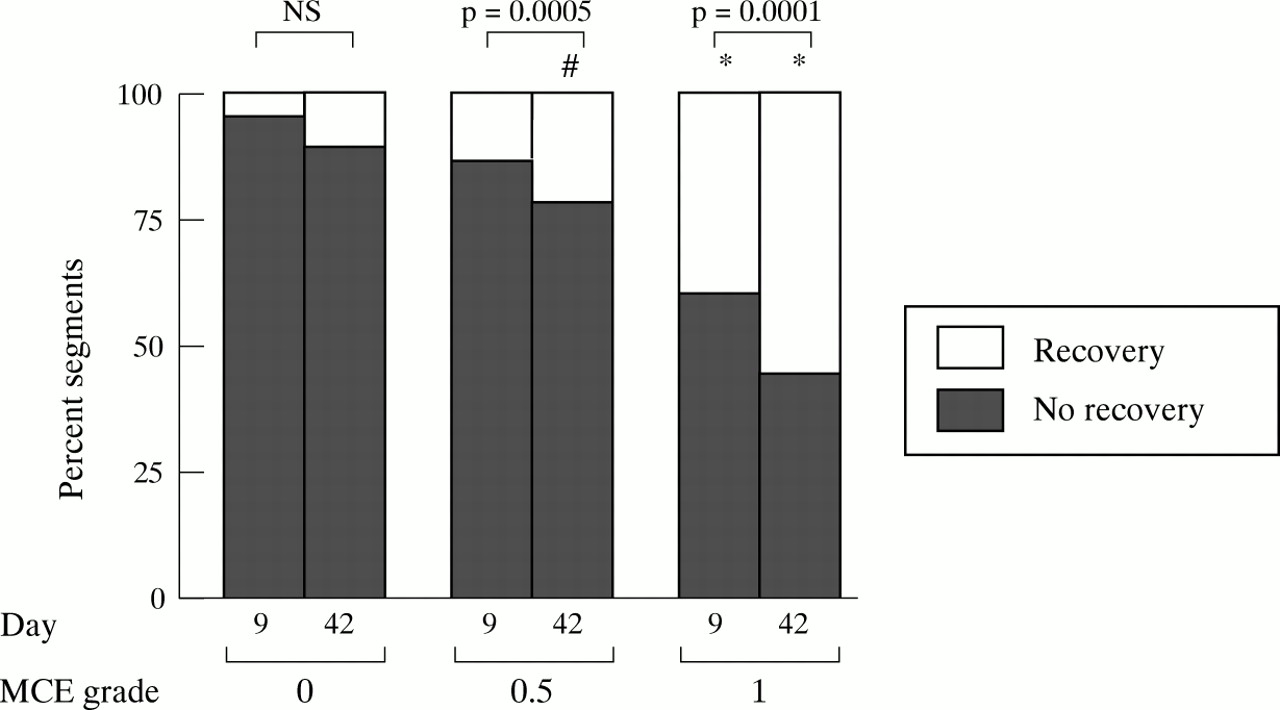
Segmental contractile function recovery according to the initial tissue perfusion pattern is shown in fig 4. Contractile recovery on day 9 was observed in 40% of MCE grade 1, while it was rare in MCE grade 0 and 0.5 segments (5% and 14% respectively). On day 42, 56% of MCE grade 1 segments showed functional recovery (p < 0.0001v MCE grade 0 and 0.5), as well as 22% of MCE grade 0.5 segments (p = 0.02 v MCE grade 0 at day 42). There was no significant improvement among MCE grade 0 segments (11%, NS v baseline and day 9) (fig 4). Therefore, the better the preservation of acute myocardial perfusion, as assessed by MCE, the earlier and more complete the functional recovery.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Bar graph showing segmental wall motion recovery (on day 9 and day 42) as a function of acute (day 0) myocardial contrast pattern. For each segment, recovery was defined as an improvement of at least one grade in the wall motion score from day 0 to day 9 or from day 0 to day 42. MCE, myocardial contrast echocardiography. *p < 0.05 v contrast grade 0 and 0.5 the same day; #p < 0.05 v contrast grade 0 the same day.
Absence of segmental contrast enhancement during acute MCE had a high negative predictive value for both day 9 and day 42 recovery of segmental contractile function (respectively 95% and 89%). The performance of MCE for predicting segmental wall motion recovery is shown in table 1.
Performance of contrast enhancement on acute myocardial contrast echocardiography (MCE) for the prediction of early (day 9) and late (day 42) wall motion recovery
INFLUENCE OF ACUTE MYOCARDIAL PERFUSION PATTERNS ON CONTRACTILE FUNCTION IN PATIENTS
Six patients (24%) showed no-reflow. They were older than patients without no-reflow (60 (10) v 48 (11) years, p = 0.02). There was a non-significant trend towards a longer time from symptom onset to angiographic demonstration of TIMI grade 3 flow in patients with no-reflow (260 (100)v 207 (50) min; p = 0.09). Both groups were similar with regard to reperfusion mode, peak creatine kinase, acute angiographic coronary collateral circulation, residual stenosis at day 9 angiography (for those treated with thrombolysis), day 9 and day 42 left ventricular ejection fraction (51% (7%)), and the use of nitrates, β blockers, or angiotensin converting enzyme inhibitors.
Regional contractile function in the area at risk improved in the early stage in patients without no-reflow (initial and day 9 wall motion score indices were, respectively, 2.8 (0.2) and 2.4 (0.4); p = 0.0005). A similar though less marked early improvement was also found in patients with no-reflow (2.9 (0.1)v 2.8 (0.2); p = 0.04). Regional contractility did not improve further by day 42.
Discussion
The findings of this study can be summarised as follows. Wall motion recovery is mainly an early process in segments with adequate tissue perfusion, involving 40% of these segments on day 9. Recovery can, however, also occur by six weeks—in 22% of the segments with incomplete initial tissue perfusion and 56% of the segments with complete initial perfusion. The absence of tissue perfusion is highly predictive of the absence of recovery of contractile function on both day 9 and day 42.
The fact that most of the functional recovery occurs early on is consistent with data of Ito et al,14 showing that in patients with angiographically proven early recanalisation, most improvement in contractile function occurs before the end of the second week. Significant recovery can, however, still be observed at six weeks in segments with homogeneous contrast enhancement. Myocardial stunning15 ,16 is a likely explanation for this phenomenon occurring in normally perfused segments.
The main new outcome of our study was a specific analysis of contractile function recovery in segments with incomplete initial perfusion, which we did by determining myocardial perfusion and contractile function at the segmental level. Recovery of contractile function in MCE grade 0.5 segments, although negligible at an early stage (day 9), was observed in a substantial proportion of segments at six weeks (22%). In these segments with heterogeneous contrast enhancement, myocardial stunning and superimposed abnormal perfusion account for reduced and delayed functional recovery.
Conversely, homogeneous (and so incomplete) tissue perfusion within the area at risk does not necessarily imply functional recovery at follow up. Several explanations could account for this phenomenon. Necrosis may not be homogeneously distributed in the myocardium, allowing residual tissue perfusion with incomplete contrast enhancement but no spontaneous functional recovery because there are insufficient myocytes.17 At rest, the contribution of the endocardium to ventricular wall thickening is more important than that of the middle or epicardial layer18 ,19; therefore, if the endocardium is necrotic, wall thickening will be diminished or even abolished despite adequate perfusion of the middle and epicardial layers in the absence of a flow limiting stenosis.20Abnormal function can occur in normally perfused segments adjacent to asynergic segments because of the tethering phenomenon.21Finally, as hypothesised by Iliceto et al,22 the ischaemic insult might be sufficient to induce necrosis in a large number of myocytes without inflicting irreversible damage to the entire microvasculature.
The high negative predictive value of the lack of perfusion (89%) for predicting the absence of functional recovery is consistent with previous studies.5-7 ,9 ,14 ,22 ,23 Microvascular integrity is thus a prerequisite for both early and late wall motion recovery in the infarcted area.
STUDY LIMITATIONS
MCE was not performed before opening the coronary artery, to shorten the time to recanalisation and to minimise the number of contrast medium injections (one in each coronary artery for each of the four echocardiographic views). This large number of echocardiographic windows was chosen to optimise the visualisation of the dyssynergic segments. The extent of initial abnormal wall motion was thus used as a surrogate of the area at risk.
As functional recovery of stunned myocardium can be delayed for more than six months after reperfusion,24 assessment of myocardial contractile recovery at six weeks could lead to underestimation of viable but severely stunned myocardium; it nevertheless minimises the risk of development of flow limiting restenosis or silent reocclusion. Hyperaemia often occurs immediately after reperfusion25 and could lead to overestimation of the extent of myocardial salvage; however, in the present study, MCE was not used to assess the extent of infarction but rather to attempt to predict functional recovery.
CONCLUSION AND CLINICAL IMPLICATIONS
Evaluation of acute microvascular perfusion allows us to predict early wall motion recovery with high specificity in the days following myocardial infarction. Emerging technical developments such as intravenous contrast agents and second harmonic imaging may allow routine and repeated assessment of microvascular perfusion at the bedside,26 ,27 obviating the need for invasive procedures. This would allow widespread use of acute tissue perfusion as a prognostic index, or for the assessment of pharmacological and mechanical reperfusion treatments.28 In patients with severe heart failure complicating acute myocardial infarction, this may help in the early triage of those who are unlikely to have rapid recovery of wall motion to ventricular assistance or heart transplant, for which proper timing is critical.29
Acknowledgments
We are deeply indebted to our colleagues from the catheterisation and echocardiographic laboratories for their invaluable help: Drs P Aubry, A Benhamer, A Boccara, L Feldman, D Himbert, G Karrillon, and P Seknadji. We also would like to thank T Laperche for his excellent secretarial skills.