Article Text

Abstract
OBJECTIVE To assess the mechanism of restenosis after balloon angioplasty.
DESIGN Prospective study.
PATIENTS 13 patients treated with balloon angioplasty.
INTERVENTIONS 111 coronary subsegments (2 mm each) were analysed after balloon angioplasty and at a six month follow up using three dimensional intravascular ultrasound (IVUS).
MAIN OUTCOME MEASURES Qualitative and quantitative IVUS analysis. Total vessel (external elastic membrane), plaque, and lumen volume were measured in each 2 mm subsegment. Delta values were calculated (follow up − postprocedure). Remodelling was defined as any (positive or negative) change in total vessel volume.
RESULTS Positive remodelling was observed in 52 subsegments while negative remodelling occurred in 44. Remodelling, plaque type, and dissection were heterogeneously distributed along the coronary segments. Plaque composition was not associated with changes in IVUS indices, whereas dissected subsegments had a greater increase in total vessel volume than those without dissection (1.7 mm3 v−0.33 mm3, p = 0.04). Change in total vessel volume was correlated with changes in lumen (p < 0.05,r = 0.56) and plaque volumes (p < 0.05,r = 0.64). The site with maximum lumen loss was not the same site as the minimum lumen area at follow up in the majority (n = 10) of the vessels. In the multivariate model, residual plaque burden had an influence on negative remodelling (p = 0.001, 95% confidence interval (CI) −0.391 to −0.108), whereas dissection had an effect on total vessel increase (p = 0.002, 95% CI 1.168 to 4.969).
CONCLUSIONS The mechanism of lumen renarrowing after balloon angioplasty appears to be determined by unfavourable remodelling. However, different patterns of remodelling may occur in individual injured coronary segments, which highlights the complexity and influence of local factors in the restenotic process.
- balloon angioplasty
- intravascular ultrasound
- remodelling
- restenosis
Statistics from Altmetric.com
Recurrence of stenosis is still an important drawback of percutaneous coronary interventions. The restenotic process is multifactorial and several elements have already been identified: thrombosis, inflammation, smooth muscle cell proliferation, and elaboration or degradation of the extracellular matrix.1 ,2 The clinical results of these processes are acute recoil, neointimal hyperplasia, and vascular remodelling, as determined by angiography and intravascular ultrasound.
The classical binary definition of restenosis is based on coronary angiography (> 50% diameter stenosis). Although clinical decision making is in essence a “binary” process, the restenotic phenomenon cannot be comprehensively analysed by luminographic methods.3 In this regard, intravascular ultrasound (IVUS) has become an essential tool owing to its ability to image structures of the vessel wall.4 Furthermore, IVUS-assessed vessel wall remodelling has been proposed as an important factor in the recurrence of stenosis after balloon angioplasty.5 ,6
The issue of restenosis has been scrutinised over recent years, but some questions remain. The relative contribution of remodelling and plaque growth to the restenotic process is still debatable.5-13 To assess the mechanism of restenosis, previous studies selected the cross section with the narrowest lumen area before the procedure,5 at follow up,6 or both.7 Although these specific sites have unquestionable validity in the clinical context, they may not represent the location of maximum arterial wall response to injury (maximum lumen loss). Furthermore, whether the pattern of arterial wall response to injury is homogeneously distributed along the entire target segment has yet to be investigated.
Three dimensional intravascular ultrasound imaging with volumetric quantification makes it possible to address these issues.14 Thus in the present study we used technological advances to assess the mechanism of restenosis after balloon angioplasty.
Methods
PATIENTS
During 1997 and 1998, 13 patients enrolled in prospective clinical studies who had de novo lesions in native coronary arteries successfully treated by conventional balloon angioplasty were eligible for the present investigation. Only patients with a scheduled six month follow up assessment and complete serial three dimensional IVUS acquisition were included. Patients treated with any other percutaneous device (cutting balloon, direct coronary atherectomy, rotational atherectomy, laser ablation, stents, or radiotherapy) or those taking any specific drugs under investigation were excluded. Angiographic inclusion criteria applied in the original studies consist of reference vessel diameter > 2.5 mm and < 4.0 mm, and lesion length < 20 mm.
Patients received aspirin (250 mg/day) and intravenous heparin (10 000 IU) before the procedure. Heparin was given to maintain an activated clotting time of > 300 seconds. Aspirin treatment was maintained after the procedure in all patients. Balloon angioplasty was performed according to standard clinical practice, and the selection of the balloon was left to the operator's preference. In this cohort, the mean balloon to artery ratio was 1.1. Postprocedure (after optimising the results of balloon angioplasty) and follow up IVUS imaging was acquired using the same motorised pullback system and after an intracoronary nitrate infusion.
The medical ethics committee of University Hospital Rotterdam approved the protocol. All patients gave written informed consent.
THREE DIMENSIONAL IVUS ASSESSMENT
Imaging of the coronary segments was done using a mechanical IVUS system (CVIS, Boston Scientific Corporation, Maple Grove, Minnesota, USA), with a sheath based IVUS 30 MHz catheter. ECG gating image acquisition and digitisation were performed by a work station designed for the three dimensional reconstruction of echocardiographic images (EchoScan, Tomtec, Munich, Germany). A description of this system has been given in detail elsewhere.15 Where image acquisition involved using the motorised pullback without ECG triggering, the complete IVUS run was recorded on super VHS video tape for off line three dimensional reconstruction.16
A Microsoft Windows based contour detection program, developed at the Thoraxcenter, was used for off line volumetric quantification.17 Briefly, this program constructed longitudinal sections from the dataset and identified the contours corresponding to the lumen and media boundaries. Intraobserver variability, assessed by analysing IVUS volumetric studies at least three months apart, has been reported—mean (SD): −0.4 (1.1)% and −0.65 (2.66)% in lumen volume, −0.4 (0.6)% and −0.19 (0.67)% in external elastic membrane volume, and −0.3 (1.0)% and −0.95 (2.81)% in plaque volumes using motorised pullback with and without ECG gating, respectively.15 ,16
Three dimensional IVUS image reconstruction and quantification has been validated previously.15 ,16 This IVUS technique may have advantages over conventional IVUS assessment, as follows:
visualisation and quantification of the entire coronary segment (not only of a single cross section) is possible, allowing longitudinal assessment of the restenotic process6;
in a coronary segment of 20 mm length, 100 cross section areas may be measured, which permits accurate identification of the sites with minimum or maximum lumen, plaque, and/or external elastic membrane areas; as the computer contour detection software automatically identifies these locations, comparisons between serial IVUS images can be performed in an unbiased fashion after both postprocedure and follow up measurements have been completed;
besides the use of motorised continuous pullback (with or without ECG triggering),18 precise location and matching of each cross section can be further assured by comparing the multiple longitudinal views displayed by the three dimensional reconstruction (fig 1);
after matched comparisons, the site with the maximum lumen loss can be readily identified, which may be essential for a mechanistic interpretation of the restenotic process.

Standard display of the results by three dimensional longitudinal reconstruction of the intravascular ultrasound cross sectional images using an ECG gated pullback. Upper outside panels: longitudinal reconstruction images immediately after the procedure (left side) and at follow up (right side). White arrows indicate the anatomical landmarks (side branches and calcium). Upper inside panels: matched cross sections immediately after the procedure (left side) and at follow up (right side). Lower panels: subsequent volumetric quantification immediately after the procedure (left side) and at follow up (right side). The area values of the lumen (lower line) and total vessel (upper line) form the boundaries of the grey zone, which represent the plaque–media complex, and a single line depicts the absolute area value of plaque–media complex. Black arrows indicate the site of the minimum lumen area (MLA).
The method for defining the segment of interest has been described previously.19 ,20 Using a Rubo DICOM viewer (Rubo Medical Imaging, Uithoorn, Netherlands), each angiographic sequence showing all balloon inflations may be displayed simultaneously on the screen and the location of the injured segment and its relation to anatomical landmarks (aorto-ostial junction and side branches) can be determined. Thus the target segment injured by balloon inflation (20 mm long) was defined. These coronary segments were divided into 2 mm long subsegments (each presenting 10 IVUS cross sections), as described previously.21 In this manner, the local pattern of the arterial response to injury can be investigated.
QUALITATIVE ANALYSIS
All individual cross sections were analysed qualitatively by two independent investigators blinded to the volumetric results. Thus the type of plaque was defined in every cross section as intimal thickening, soft, fibrous, mixed (soft fibrous, soft calcific, and fibrous calcific), and diffusely calcified, as proposed by Di Mario and colleagues.22 ,23 Each subsegment was categorised as normal (< 0.3 mm intimal thickening), soft, hard (fibrous and mixed), or diffusely calcified, when at least 80% of the cross sections within the subsegments were of the same type, as described previously.21 In those cross sections containing up to 90° calcium arc, the contour of the external elastic membrane was interpolated from the contours of the slice immediately proximal and distal to the cross section in question. Those subsegments with side branches involving > 90° of the circumferential arc in more than 50% of the cross sections, or those categorised as diffusely calcified, were excluded from the quantitative analysis. The presence of dissection, defined as a tear parallel to the vessel wall,22 was also noted in each subsegment.
QUANTITATIVE MEASUREMENTS AND DEFINITIONS
Total vessel volume determined by external elastic membrane boundaries and lumen volume was measured. Plaque volume was automatically calculated by subtracting lumen volume from total vessel volume. Delta values for each measurement were calculated (Δ = follow up − postprocedure). Relative (%) changes in IVUS indices (Δ volume/postprocedure volume) were also calculated in order to correct for differences in vessel size.
The location of the cross section with the narrowest lumen area at follow up was automatically reported. Retrospectively, the subsegment encompassing this specific cross section (minimum lumen area site) was identified and the matched subsegment of the postprocedure analysis was selected for comparison. Furthermore, the site with the maximum lumen loss was defined after the calculation of the Δ values.
Remodelling was defined as a continuous process involving any (positive or negative) changes in external elastic membrane volume as proposed previously.24 In the present study, enlargement or shrinkage of the vessel wall was assumed when total vessel volume increased or decreased, respectively, compared with postprocedure measurement by at least 2 SD (± 1.3%) of the intraobserver variability for repeat total vessel volume measurements.15 ,16 In this way the potential intrinsic error of the method may be avoided.25 ,26
STATISTICAL ANALYSIS
Quantitative data are presented as mean (SD), while qualitative data are presented as frequencies. Continuous variables were compared using the unpaired Student ttest. Categorical variables were compared using Fisher's exact test. Linear regression (Pearson's regression coefficient) was performed to assess the correlation between changes in IVUS indices. Multivariable linear regression models were built to identify predictors of changes in plaque volume and total vessel volume among qualitative and quantitative postprocedure IVUS variables. A probability value of p < 0.05 was considered significant.
Results
In 13 coronary segments injured by balloon inflation, 111 subsegments were analysed using three dimensional IVUS volumetric quantification. Baseline characteristics of the patients are shown in table 1. Nineteen subsegments were excluded from the final analysis owing to either diffusely calcified plaque (n = 10), which precluded the quantification of the total vessel volume, or side branches which involved more than 90° of the circumferential arc in more than 50% of the cross sections (n = 9).
Baseline and demographic characteristics
QUALITATIVE ANALYSIS
Table 2 shows the variability in distribution of both the type of plaque and the presence of dissection along the whole length of the target segments. Only three patients had the same type of plaque distributed throughout the analysed segment, whereas the presence of dissection in at least one injured subsegment was noted in nine patients.
Number of subsegments with specific intravascular ultrasound (IVUS) findings in each patient
Forty subsegments (36%) were defined as soft, 53 (48%) as hard, and 18 (16%) as normal/intimal thickening. Plaque composition was not related to changes in quantitative volumetric IVUS indices. Subsegments with hard plaques showed a greater incidence of dissection than those with soft plaques (49% v 23.7%, p < 0.001).
Overall, dissection was observed in 35 subsegments (31.5%). Subsegments with dissection had greater increase in total vessel volume than those without dissection (1.7 mm3 v −0.33 mm3, p = 0.04).
QUANTITATIVE ANALYSIS
Table 3 shows the mean values of changes (Δ) in IVUS indices for all subsegments of the entire target vessel, at the minimum lumen area location and at the maximum lumen loss site. The correlation between remodelling, changes in plaque volume, and late lumen loss are shown in fig 2.
Changes in intravascular ultrasound findings after six months

Correlation between remodelling (ΔTVV), changes in plaque volume (ΔPV), and changes in lumen volume (ΔLV). Upper panels: correlations in all subsegments (n = 111). Middle panels: correlations at the subsegments of minimum lumen area at follow up (n = 13). Lower panels: correlations at the maximum late lumen loss sites (n = 13).ΔTVV, change in total vessel volume;ΔPV, change in plaque volume;ΔLV, change in lumen volume. *Significant correlation (p < 0.01).
REMODELLING
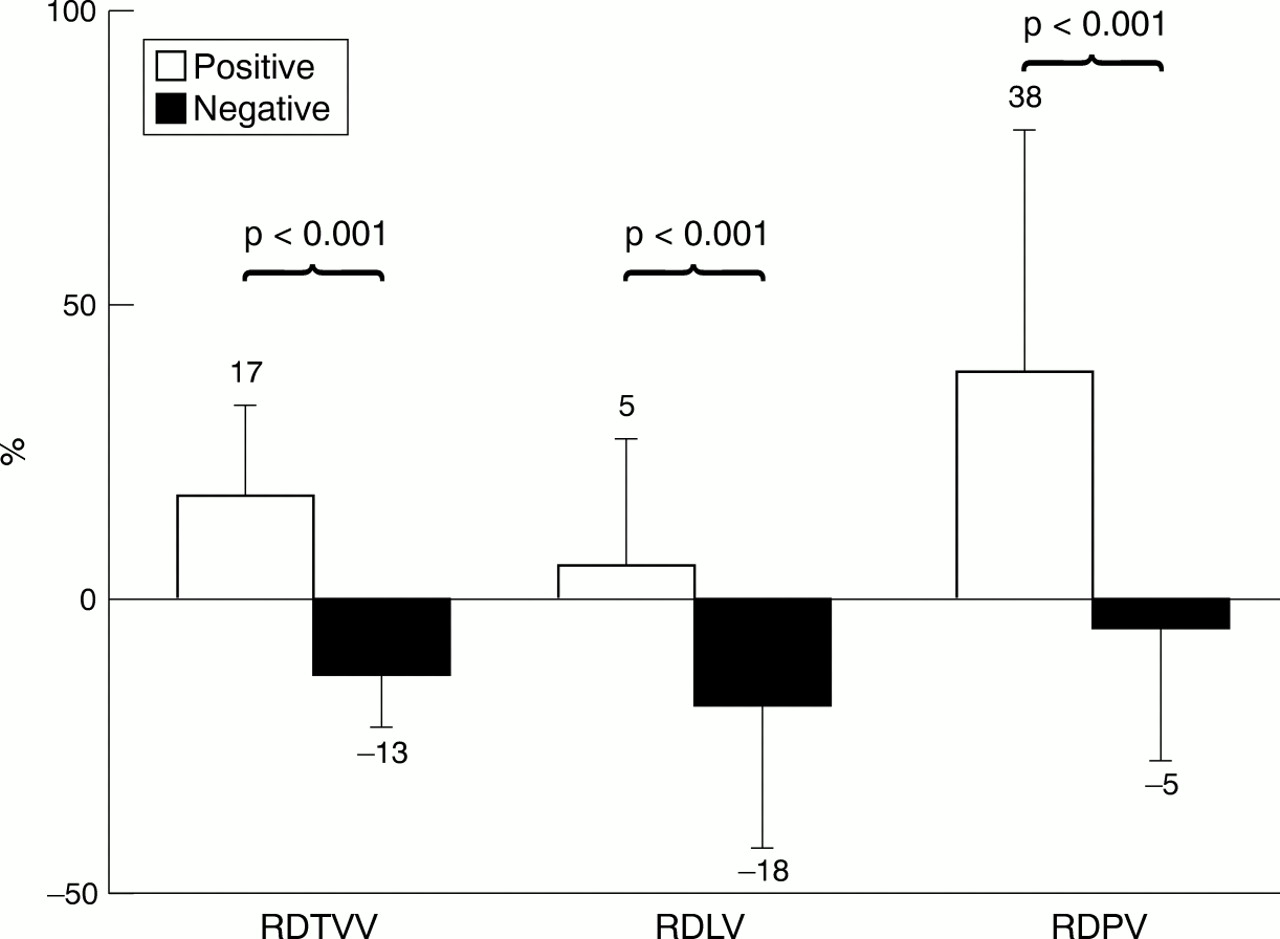
Positive remodelling was observed in 52 subsegments (46.8%), while negative remodelling occurred in 44 (39.6%). Both patterns of remodelling were observed along the entire injured segment in the majority of the patients (n = 10) (table 2). Although subsegments showing negative remodelling had a larger residual plaque volume after the procedure, the increase in plaque volume was greater in those subsegments with positive remodelling (fig 3). Indeed, subsegments with negative remodelling showed a decrease in plaque volume.

{kind=link}
{kind=link}
{kind=link}
Comparison of relative changes in total vessel volume (RDTVV), lumen volume (RDLV), and plaque volume (RDPV) between subsegments with negative (n = 44) and positive (n = 52) remodelling.
MULTIVARIATE ANALYSES
Postprocedure IVUS predictors of changes in both total vessel volume and plaque volume are shown in table 4. Residual plaque volume had a negative influence on remodelling, whereas the presence of dissection had a positive effect on total vessel volume increase. Postprocedure lumen volume was directly associated with plaque increase (table 4).
Postprocedure intravascular ultrasound (IVUS) predictors of changes in plaque volume and total vessel volume after six months
Discussion
In this study, where we assessed the local mechanism of restenosis using subsegmental volumetric quantification of the entire injured vessel, we showed the variability of both the qualitative IVUS indices and the patterns of remodelling within the same target segment (table2), as observed by Pasterkamp and colleagues in human femoral arteries.27 Furthermore, in the majority (n = 10) of the cases, the site with maximum lumen loss was not the same as the site of the minimum lumen area at follow up, and the mean (SD) distance between these two specific sites was 5.3 (4.8) mm. These findings highlight the importance of analysing the entire injured segment when studying the mechanism of restenosis using IVUS in the future.
Our results also confirm that unfavourable remodelling is the major determinant of lumen loss (fig 2). On the basis of the average values of changes in IVUS indices (table 3), lumen loss after balloon angioplasty appears to be determined mainly by an increase in plaque volume. Similar results were found in two recent prospective studies.7 ,28 The mean lumen loss in the balloon angioplasty group of the SURE (serial ultrasound restenosis) trial7 and the placebo group of the MVP (multivitamins and protocol) study28 mainly resulted from an increase in plaque area. In contrast, pioneer retrospective studies have described vessel shrinkage as causing 50–70% of lumen loss,5 ,6though average values may not represent the relative contribution of both remodelling and plaque growth to lumen loss. Using linear regression, as suggested previously,24 we observed that lumen loss was actually determined by changes in vessel size (fig 2). Whereas change in total vessel volume was highly correlated with lumen loss in all analyses, the change in plaque volume was only weakly related to change in lumen volume (fig 2).
Whether remodelling is an independent process or an adaptive response to compensate plaque growth is still debated.8 ,10 The correlation between changes in vessel size and plaque volume observed in the present investigation (fig 2) suggests that remodelling after balloon injury may represent an adaptive phenomenon, as described by Glagov and colleagues in atherosclerotic plaques.29 In fact, this correlation is in both directions: segments with positive remodelling showed an increase in plaque volume, whereas those with vessel shrinkage had a plaque reduction (fig 3). Similar findings have been reported previously.30 These studies support the hypothesis that plaque retraction may be the ultimate determinant of negative remodelling.31 However, other factors such as inflammation32 and shear or tensile stress33may exert an influence in both remodelling and plaque progression.
Local tensile stress, which is determined by lumen radius, may have stimulated plaque progression in subsegments with a large residual lumen maintaining the baseline shear stress, as suggested by Glagov and colleagues.33 ,34 Similarly, shear stress may be implicated in the negative correlation between residual plaque volume and vessel remodelling, and in the positive influence of dissection on vessel enlargement (table 4).33 However, direct measurements of both tensile stress and shear stress in vivo are exceedingly complex and require sophisticated and laborious technology for any definitive conclusions to be drawn.35
The previous hypothesis, based on angiographic studies, that non-occlusive residual coronary dissection has a favourable long term outcome may be supported by the present IVUS study,36 ,37because a positive influence of residual dissection on vessel enlargement was observed (table 4).
Plaque composition as characterised by IVUS was not correlated with any changes in IVUS indices, as reported by others.5 ,6Conversely, hard or calcific plaques have been implicated in negative remodelling in both atherosclerotic and restenotic lesions.21 ,26 ,38 Methodological differences may explain the divergent results, as these latter studies did not assess the influence of plaque composition on change in IVUS variables over time, as performed in the other studies5 ,6 and in the present investigation.
In summary, the findings we report here, involving three dimensional IVUS quantification of local changes in the vessel wall volume, illustrate the complexity and variability of the arterial wall response to balloon injury and the importance of local factors (shear stress, growth factors, inflammation, degree of injury, and so on) in determining this response.2 ,39
LIMITATIONS
As in previous IVUS investigations,5 ,6 the small number of patients is a limitation of our study. However, this is the first study employing a unique new method of assessing the local process of restenosis in 111 matched subsegments injured exclusively by balloon inflation. The lack of preprocedure IVUS imaging limits the ability of baseline remodelling on the ultimate vessel response to balloon injury.