Article Text

Abstract
The histopathology of in-stent restenosis (ISR) following γ brachytherapy is described. Such histology has not been reported previously. An 82 year old man presented with recurrent ISR three months after γ brachytherapy to an area of ISR within a native circumflex vessel. The recurrent ISR was treated with directional coronary atherectomy; the histopathology of this directional coronary atherectomy specimen is discussed. These histopathological examinations showed abundant extracellular matrix material. Surprisingly, there was a relatively small cellular (myofibroblastic) component, with an absence of endothelial cells and little evidence of active proliferation. ISR after γ brachytherapy may be a pathologically distinct entity.
- stents
- restenosis
- brachytherapy
- histology
Statistics from Altmetric.com
The histology of coronary artery lesions may shed light on their pathogenesis. We here describe the histopathology of in-stent restenosis (ISR) following γ brachytherapy. Such histology has not been reported previously.
CLINICAL DETAILS AND INTERVENTIONAL PROCEDURE
An 82 year old man presented with recurrent angina three months after γ brachytherapy for ISR. He had a history of coronary artery bypass grafting and aortic valve replacement three years previously, with vein grafts to the posterior descending artery and obtuse marginal branch of circumflex artery, as well as a left internal mammary artery graft to the left anterior descending vessel. He also had a history of multiple myeloma, hyperlipidaemia, and coeliac disease.
Six months before his most recent admission, he had presented with recurrent angina. Posterolateral ischaemia was shown on thallium study, associated with an occluded obtuse marginal branch vein graft. He therefore underwent stenting of a 90% lesion in the proximal native circumflex artery extending up to the left main coronary artery, with a 3.0 × 15 mm BiodivYsio stent (Biocompatibles, Farnham, Surrey, UK). After doing well initially, he returned with a recurrence of angina three months after stent placement. Angiography then showed an occlusive type IV ISR1 within the circumflex vessel extending proximally into the distal left main coronary artery (fig 1A). A cutting balloon angioplasty was performed using a 3.5 × 15 mm cutting balloon (Interventional Technology, San Diego, California, USA) inflated to 10 atm followed by a 3.25 × 13 mm Highsail balloon (Guidant, Indianapolis, Indiana, USA) inflated to 18 atm. Intravascular ultrasound suggested a lesion length of 23 mm and a 10 seed Cordis γ radiation ribbon was positioned across the lesion with a dwell time of 17 minutes (fig 1B). Angiography at the conclusion of the procedure showed a very satisfactory result (fig 1C).

Coronary angiography in right anterior oblique (RAO) projection, showing circumflex (Cx) coronary artery. (A) First episode of Cx in-stent restenosis (ISR) with an occlusive type IV ISR lesion evident between the arrows in the Cx extending into the distal left main coronary artery (LMCA; marked). The left anterior descending coronary artery stump (LAD st) and guiding catheter (GC) position are marked. (B) After cutting balloon dilatation was performed, intracoronary γ brachytherapy was undertaken, with seed positioning seen between the marked arrows in the Cx. (C) Final angiographic result after brachytherapy and balloon dilatation. (D) Further ISR seen three months after brachytherapy. There is a 90% type III lesion between the marked arrows at the same site. (E) Final angiographic appearances after directional coronary atherectomy (DCA) and further balloon angioplasty.
The patient’s symptoms initially improved, but he returned to the hospital three months later with recurrent angina and ischaemia on exercise testing. Angiography showed a 90% stenosis of type III ISR1 (fig 1D) at the same site. This was treated with directional coronary atherectomy and subsequent balloon angioplasty, again with a good angiographic result (fig 1E).
STAINING
Fragments retrieved from the atherotome were immediately placed in 10% buffered formalin and routinely processed for paraffin embedding. Five micrometre sections were cut and treated with haematoxylin and eosin, periodic acid-Schiff, Mallory trichrome, Wilders stain for reticulin, Verhoeff elastic, giemsa, and alcian blue stains. Sirius red staining for collagen subtypes was performed as previously described.2
Immunohistochemical stains included antibodies to smooth muscle actin (Sigma, Aldrich, St Louis, Missouri, USA), muscle specific actin (HHF 35, ENZO Diagnostics, Faringdale, New York, USA), desmin (Dako, Glostrup, Denmark), CD31 (Dako), CD34 (Becton Dickinson, Franklin Lakes, New Jersey, USA), CD68 (KP-1, Dako), factor VIII (Dako), Ki-67 (Zymed, San Francisco, California, USA), and proliferating cell nuclear antigen (PCNA; Dako). After blocking with horse serum, the tissue was treated with primary antibodies followed by horse antirabbit/mouse secondary antibody and streptavidin with peroxidase (BioGenex, San Ramon, California, USA) for antibodies to muscle specific actin, Ki-67, and PCNA or avidin-biotin horseradish peroxidase complex (Dako) for the other primary antibodies. Slides were developed with 3-amino-9-ethyl-carbazole (Sigma) and counterstained with Gill’s haematoxylin (Fisher Scientific).
HISTOPATHOLOGY
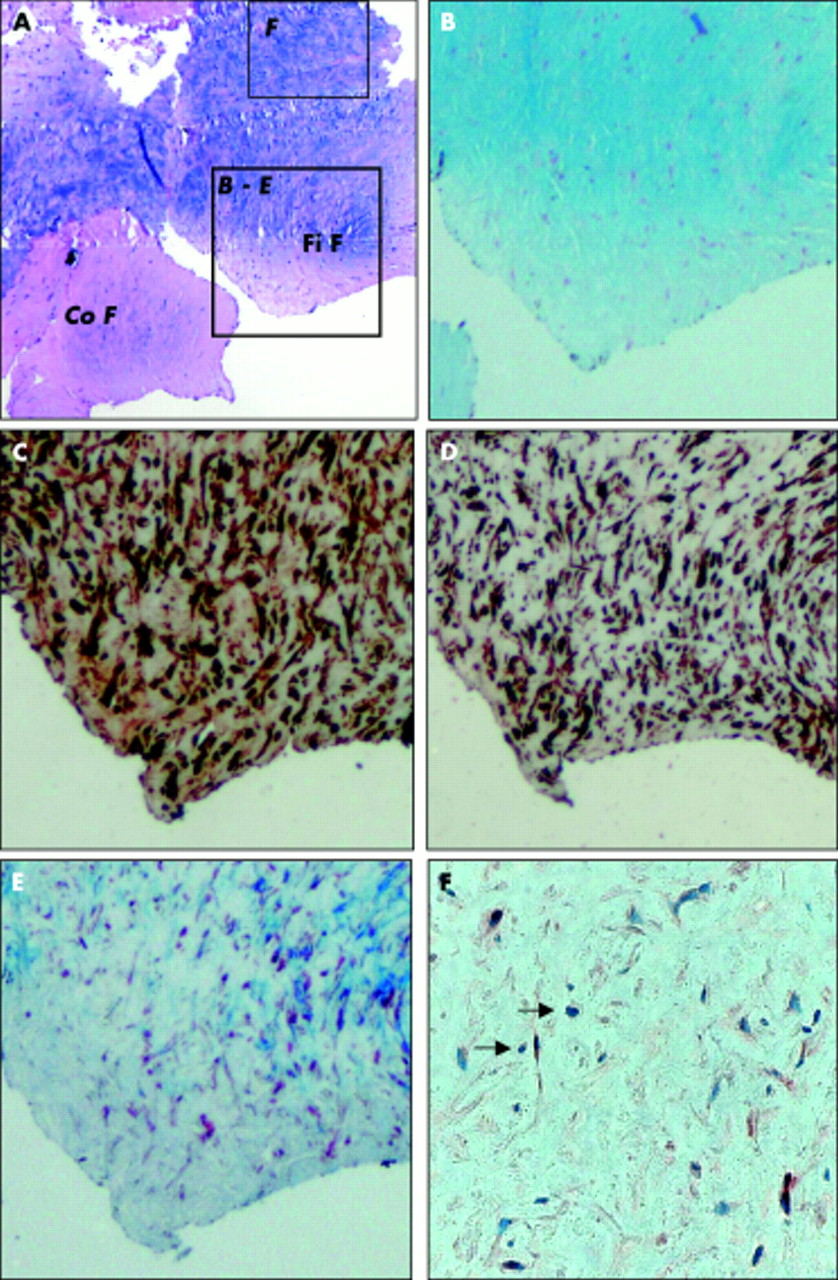
Two patterns of collagen were present, one consisting of old collagen fibres and the other of new collagen fibres (fig 2A). The precise collagen type was not discernable from the limited amounts of tissue available, although there was evidence of type III collagen, sparsely distributed in some areas (fig 3). A trichrome stain showed the coarse nature of old collagen in contrast to the finely fibrillar nature of new collagen. Within the latter were numerous plump spindled and polygonal cells. These spindled cells stained positively for smooth muscle actin and muscle specific actin but not for desmin. This staining pattern suggests a myofibroblastic phenotype. Reticulin was present in both areas of collagen on reticulin staining. Giemsa and alcian blue stains showed the presence of abundant non-fibrillar extracellular matrix enveloping the plump spindled cells. A Verhoeff stain showed no evidence of elastic tissue. The special stains thus defined the lesion of ISR as being paucicellular and rich in ground substance, consisting of differing patterns of collagen and non-fibrillar proteoglycans.

Histopathology. (A) Haematoxylin and eosin stain (× 2) showing two distinct zones of coarse, old collagen fibres (Co F) and fine, fibrillar, new collagen fibres (Fi F). Marked square (B-E) indicates areas from which figs 2B–E are taken. Marked rectangle (F) indicates area from which fig 2F is taken. (B) Alcian blue (× 6.4) staining showing diffuse dense staining consistent with abundant extracellular matrix (ECM). (C, D) Muscle specific actin (× 6.4) and smooth muscle actin (× 6.4) suggest that spindle and polygonal cells are of a myofibroblastic phenotype. (E) Trichrome stain (× 6.4) suggests fibrillar nature of new collagen. (F) Proliferating cell nuclear antigen stain (× 40) shows patchy, focal positivity (marked by arrows) localised to area F.

{kind=link}
{kind=link}
{kind=link}
Histopathology. Sirius red (× 40) staining of additional tissue fragments imaged under polarised light. Background appears blue, type III collagen appears green (marked with arrow).
Immunohistochemical stains for CD31, CD34, and factor VIII were negative (data not shown), suggesting that endothelial cells were absent from the lesion. PCNA staining showed scattered, focally positive polygonal cells, indicative of patchy active cellular proliferation. Ki-67 staining, however, was negative (data not shown). These findings suggest that γ brachytherapy may have prevented the development of a more proliferative cellular fibrosis and prevented endothelial participation in the fibrous reaction.
DISCUSSION
This is the first documented histological examination of ISR occurring after γ brachytherapy. Although these novel findings are limited to the study of a single patient, they may provide insights into the mechanism(s) by which γ brachytherapy affects the development of recurrent arterial restenosis. Three features of the pathology are noteworthy.
The first feature is the abundance of extracellular matrix. Data regarding ISR in humans with no prior radiation treatment are sparse and conflicting. One study compared lesions of ISR after five months with atheromatous plaque and found that almost all of the ISR tissue was composed of smooth muscle cells.3 A second study found large amounts of extracellular matrix in ISR specimens nine months after the procedure.4 A clinical picture with some resemblance to that of our patient has been previously reported, in which a proteoglycan-rich matrix developed in a coronary artery lesion at the edge of a stent in a patient six months after excimer laser angioplasty and γ brachytherapy—the so called “candy wrapper” lesion.5 The tissue from our patient was, however, from a truly restenotic lesion within the stent and was examined at the even earlier time point of three months. This offers further evidence of an association between brachytherapy and the large amount of extracellular ground substance in these lesions of restenosis after treatment with radiation.
The second feature is the absence of evidence of widespread cellular proliferation. There was evidence of focal cellular proliferation, as detected by PCNA staining; however, this apparent component of cellular proliferation lacked confirmation of Ki-67 positive staining. Prior studies of ISR without radiation suggest that Ki-67 positive cells resemble those of native coronary athersclerotic lesions, and studies examining proliferation using PCNA in peripheral vessels have provided similar results.4,6 Proliferating cells—as detected by bromodeoxyuridine uptake—in ISR in the vessels of rabbits treated with β radiation increased in number compared with controls, although the number of positive cells decreased with increasing radiation dose.7 Radiation may either stimulate or inhibit cellular proliferation, depending on dose,8 and intravascular ultrasound imaging has suggested that acellular necrotic areas can develop after brachytherapy.9 It is therefore possible that radiation results in a complete abrogation of cellular proliferation in some areas and patchy, focal zones of proliferation in others.
Thirdly, the two patterns of collagen are intriguing. The more coarse pattern is consistent with older collagen; in contrast, the finely fibrillar morphology may depict a newer collagen. The histopathology thus shows evidence of temporal diversity in the development of ISR—the finer collagen being from the more recent episode following brachytherapy. It is clearly possible that the two collagen patterns reflect simply these differences in timing of the ISR process, being unrelated to brachytherapy per se. Unfortunately, lack of an adequate amount of tissue precluded further definition of collagen type and maturation, as well as specific characterisation of the non-fibrillar extracellular matrix, although some evidence of sparse type III collagen was present. Such additional studies, as well as electron microscopy, may contribute further information towards the understanding of the pathogenesis of lesions of ISR as more tissue becomes available.
In summary, these data show that ISR three months after γ brachytherapy consists of abundant extracellular matrix material, including collagen. Surprisingly, there is a relatively small cellular (myofibroblastic) component in the lesion, with an absence of endothelial cells and little evidence of active proliferation. The possibility exists that ISR after γ brachytherapy is a pathologically distinct entity.
Acknowledgments
HC Lowe is a CJ Martin Fellow of the NHMRC of Australia.