Article Text

Abstract
Background The decision to repair mild-to-moderate functional tricuspid regurgitation (TR) during left-side heart surgery remains controversial.
Objectives To avoid heterogeneity in patient population, patients with TR undergoing isolated mechanical mitral valve (MV) replacement for rheumatic mitral diseases were evaluated.
Methods Between 1997 and 2009, 236 patients with mild-to-moderate functional TR underwent first-time isolated mechanical MV replacement for rheumatic mitral diseases with (n=123; repair group) or without (n=113; non-repair group) tricuspid valve (TV) repair. Survival, valve-related complications, and TV function in these two groups were compared after adjustment for baseline characteristics using inverse-probability-of-treatment weighting.
Results Follow-up was complete in 225 patients (95.3%) with a median follow-up of 48.7 months (IQR 20.2–89.5 months), during which time 991 echocardiographic assessments were done. Freedom from moderate-to-severe TR at 5 years was 92.9±2.9% in the repair group and 60.8±6.9% in the non-repair group (p<0.001 and 0.048 in crude and adjusted analyses, respectively). After adjustment, both groups had similar risks of death (HR=0.57, p=0.43), tricuspid reoperation (HR=0.10, p=0.080) and congestive heart failure (HR=1.12, p=0.87). Postoperative moderate-to-severe TR was an independent predictor of poorer event-free survival (HR=2.90, p=0.038).
Conclusions These findings support the strategy of correcting mild-to-moderate functional TR at the time of MV replacement to maintain TV function and improve clinical outcomes.
- Surgery-valve
- tricuspid valve disease
- prosthetic heart valves
- echocardiography
- dissection
- atrial fibrillation
- cardiac surgery
- heart transplant
- surgery-coronary bypass
- surgery-paediatric
Statistics from Altmetric.com
- Surgery-valve
- tricuspid valve disease
- prosthetic heart valves
- echocardiography
- dissection
- atrial fibrillation
- cardiac surgery
- heart transplant
- surgery-coronary bypass
- surgery-paediatric
Introduction
Functional tricuspid regurgitation (TR) is commonly associated with mitral valve (MV) diseases, and the presence of significant TR is reported to be an indicator of poor prognosis after the surgical correction of MV diseases.1 2 Concomitant tricuspid valve (TV) repair or replacement at the time of MV surgery has been recommended in patients with severe functional TR to improve long-term clinical outcomes.3–7
However, the decision to repair mild-to-moderate functional TR during MV surgery remains controversial. Although TR can regress after successful MV surgery without TV repair,2 8 functional TR may progress even after successful MV surgery, suggesting that even if mild, TR should be treated surgically.9 10
Postoperative TV functions may be affected by residual or recurrent left-sided heart lesions such as mitral regurgitation/stenosis following mitral repair or structural valve degeneration following bioprosthetic valve implantation. Thus, the differences in left heart surgery type can influence as confounders in analysing the impact of TV repair on the outcomes of functional TR. However, most studies dealing with this subject have been limited by examining heterogeneous left-sided heart lesions or by including different surgical techniques (repair, bioprosthetic or mechanical valve replacement) that might influence the outcomes, making the study results difficult to interpret. Therefore, to avoid heterogeneity in patient populations and to minimise the confounding effects of residual or recurrent left-sided heart lesions, we evaluated patients with mild-to-moderate functional TR undergoing isolated mechanical MV replacement for rheumatic mitral diseases.
Methods
Study population
From July 1997 to July 2009, 916 patients with mild-to-moderate functional TR associated with MV disease underwent MV replacement using a mechanical prosthesis, with or without concomitant TV surgery, at our institution. Functional TR was defined as TR without definite organic leaflet or subvalvular deformities, such as TV prolapse, Ebstein anomaly, rheumatic and infective endocarditis. Patients who underwent concomitant cardiac surgery for congenital heart defects, aortic valves, aorta, cardiac tumours, pericardial diseases or coronary artery bypass grafting (n=521), and those with a history of previous cardiac surgery were (n=135) were excluded to reduce heterogeneity in the patient population. One patient who underwent TV replacement with mechanical prosthesis for moderate TR was also excluded, as were 23 patients with non-rheumatic causes of MV diseases (n=23). Of the remaining 236 patients, 123 underwent concomitant TV repair (repair group) and 113 received MV replacement alone (non-repair group). The decision to perform a TV repair was affected by the degree of TR and the presence of atrial fibrillation but was ultimately at the discretion of attending surgeon. The surgeons who performed TV repair tend to combine the Maze procedure more frequently in the presence of atrial fibrillation.
This study was approved by our institutional ethics committee/review board, which waived the requirement for informed patient consent owing to the retrospective nature of this study.
Echocardiography
Two-dimensional echocardiography and Doppler colour-flow imaging were performed using a Hewlett–Packard Sonos 2500 or 5500 imaging system equipped with a 2.5 MHz transducer (Hewlett–Packard, Andover, Massachusetts, USA). All patients underwent preoperative echocardiography within the 2 months before surgery. The degree of TR was evaluated using the apical four-chamber view, and graded as mild, moderate or severe when the distal jet area was <5 cm2, 5–10 cm2 or >10 cm2, respectively.11
Surgical procedures
The conventional approach consisted of a median sternotomy, ascending aorta and bicaval cannulation and a longitudinal right-sided left atriotomy. Moderately hypothermic (28–32°C) cardiopulmonary bypass was used, and myocardial protection was achieved with cold or tepid blood cardioplegia.
All patients received a bileaflet mechanical valve and surgeons attempted to retain subvalvular tissue whenever possible. Sixty-seven patients (54.5%) in the repair group and 27 (23.9%) in the non-repair group underwent a concomitant Maze procedure, performed using a modified Cox-Maze III technique.12–14 All patients were evaluated intraoperatively by transoesophageal echocardiography.
Of the patients in the repair group, 54 (43.9%) had ring annuloplasty and 69 (56.1%) had suture annuloplasty. Ring annuloplasty involved a Carpentier ring (Edwards Lifesciences, Irvine, California, USA) in 10 patients (median size 32 mm, range 28–36 mm), a Duran ring (Medtronic, Minneapolis, Minnesota, USA) in 38 patients (median size 27 mm, range 25–33 mm) and an Edwards MC3 annuloplasty ring (Edwards Lifesciences) in six patients (median size 28 mm, range 26–32 mm). Kay annuloplasty (n=10) or a De Vega procedure (n=59) was performed for suture annuloplasty according to each surgeon's preference.
Follow-up
Data were obtained through March 2010 during regular visits to the outpatient clinic or by telephone interviews. Operative mortality was defined as death within 30 days of surgery or in-hospital death.
The primary end points of this study were defined as all-cause death and cardiac-related morbidities, with the latter including hospitalisation due to congestive heart failure (CHF) and a requirement for TV reoperation. The secondary end point was the presence of significant TR defined by moderate-to-severe degree on postoperative echocardiographic evaluation.
Anticoagulation therapy was adjusted during outpatient visits at 3-month intervals to achieve a target international normalised ratio (INR) of 2.0–3.0. Patients with inadequate INR values were evaluated weekly or monthly until the target INR was achieved.
Statistical analysis
Categorical variables are presented as frequencies and percentages, and continuous variables as means±SD or medians with ranges. Between-group differences in baseline clinical and echocardiographic characteristics were compared using the t test or the Mann–Whitney U test for continuous variables and the χ2 test or Fisher's exact test for categorical variables, as appropriate. Cumulative incidence rates of individual and composite outcomes were estimated using the Kaplan–Meier method and compared using the log-rank test. To reduce the impact of treatment selection bias and potential confounding in an observational study, we performed rigorous adjustment for significant differences in patient characteristics using weighted Cox proportional-hazards regression models and inverse-probability-of-treatment weighting (IPTW)15 16; weights for patients undergoing MV replacement alone were the inverse of (1 minus propensity score) and weights for patients undergoing both TV repair and MV replacement were the inverse of the propensity score. Propensity scores were estimated by multiple logistic-regression analysis.15 All prespecified covariates were included in full non-parsimonious models for MV replacement plus TV repair versus MV replacement alone (table 1). The discrimination and calibration abilities of each propensity score model were assessed by C statistics and the Hosmer–Lemeshow test. The model was well calibrated (Hosmer–Lemeshow test; p=0.340) with reasonable discrimination (C statistic=0.906). Univariable and multivariable risk factor analyses for postoperative moderate-to-severe TR were performed using the Cox proportional-hazards model. Variables with a p value ≤0.20 in univariable analyses were candidates for the multivariable models. Multivariable analyses involved a backward elimination technique and only variables with a p value <0.10 were used in the final model. To evaluate the influence of postoperative residual or recurrent TR on clinical outcomes, the time-updated Cox models incorporated postoperative TR and some important risk covariates that had significant effects (p<0.1) on clinical outcome.17
Baseline patient characteristics
All reported p values are two-sided, and values of p<0.05 were considered statistically significant. SAS software V.9.1 (SAS Inc) was used for statistical analysis.
Results
Baseline profiles
Mean age at surgery was 52.0±10.5 years, and 79 patients (33.5%) were male. Baseline characteristics of patients are shown in table 1. Patients in the repair group were more likely to have moderate TR and a larger left atrium than those in the non-repair group. Atrial fibrillation was more common in the repair group, and a greater proportion of patients with atrial fibrillation in the repair group underwent the concomitant Maze procedure than in the non-repair group. After adjustment, there were no significant differences in baseline profiles between the two groups. Clinical follow-up was complete in 225 patients (95.3%), with a median follow-up duration of 48.7 months (range 0.2–147.6 months, IQR 20.2–89.5 months).
Clinical outcomes
Perioperative results
Aortic clamping (87.9±30.5 min vs 64.6±30.9 min, p<0.001) and cardiopulmonary bypass (131.8±45.2 min vs 103.4±39.7 min, p<0.001) times were significantly longer in the repair group than in the non-repair group. There were two operative deaths (0.8%), but no significant between-group differences in operative mortality or morbidity (table 2).
Operative outcomes
Primary clinical end points
There were 14 late deaths, including 10 cardiac deaths. Non-cardiac causes of death were malignancy for three patients and traffic accident for one.
One patient in the repair group and four in the non-repair group required a TV reoperation. The patient in the repair group had mild TR preoperatively, but TR worsening to a very severe degree with deterioration in vital signs was seen on postoperative day 1. The reoperation was performed immediately, which showed that TR worsening was caused by a distorted TV annulus due to a prosthetic ring. TV replacement with a tissue valve was performed, with no further complications. The three patients in the non-repair group underwent TV reoperations owing to progressive worsening of TR, which constituted symptoms of heart failure. The reoperations included TV repair (ring annuloplasty) in one patient and TV replacement with a mechanical prosthesis in two, performed 35.1–104.4 months after the initial operation. Coaptation failure secondary to marked annular dilatation with severe leaflet tethering in the latter two patients seemed not merit the repair technique. Another patient in the non-repair group underwent reoperative aortic valve replacement plus TV repair (De Vega technique) owing to infective endocarditis involving the aortic valve, accompanied by moderate functional TR, at 5.4 months postoperatively.
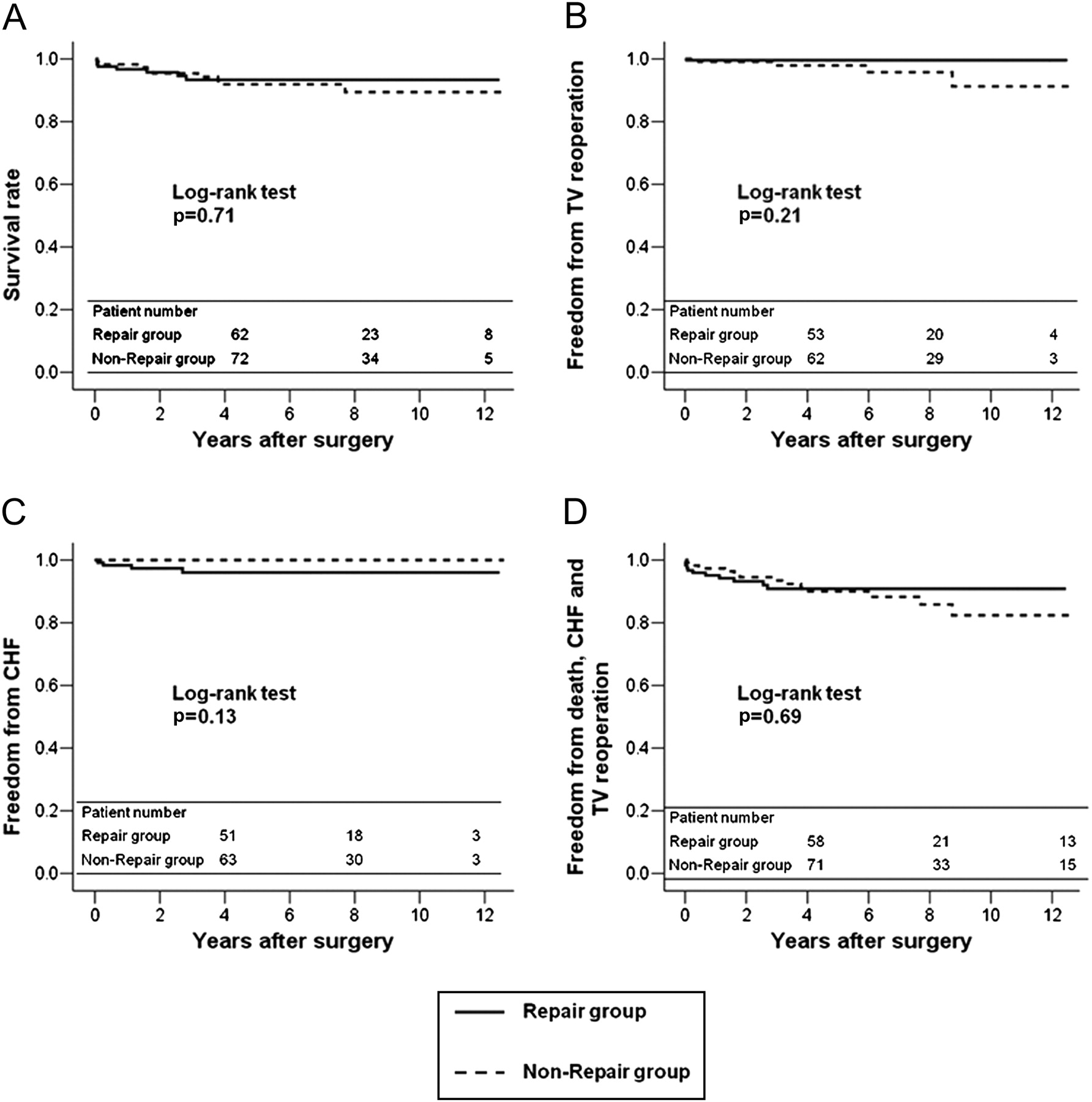
Figure 1 depicts the unadjusted rates of freedom from all-cause death, TV reoperation, readmission due to CHF and the composite of primary clinical end points. Both groups showed similar rates of freedom from all-cause death (p=0.71), TV reoperation (p=0.21), readmission due to CHF (p=0.13) and the composite of primary end points (p=0.69).

Unadjusted Kaplan–Meier curves of clinical end points in the repair and non-repair groups. (A) Overall survival. (B) Freedom from tricuspid valve reoperation. (C) Freedom from congestive heart failure requiring readmission. (D) Freedom from the composite of death, tricuspid valve reoperation and congestive heart failure requiring readmission. CHF, congestive heart failure; TV, tricuspid valve.
When patient outcomes were adjusted using IPTW, patients in the repair group were at similar risks of death (HR=0.57, 95% CI 0.14 to 2.28; p=0.43), TV reoperation (HR=0.10, 95% CI 0.01 to 1.31, p=0.080), CHF (HR=1.12, 95% CI 0.29 to 4.40, p=0.87) and the composite of primary end points (HR=0.48, 95% CI 0.16 to 1.47, p=0.20) as patients in the non-repair group.
Other late outcomes
The incidence of other late events is shown in table 2. In the repair group, one patient underwent aortic valve replacement owing to the development of aortic steno-regurgitation and one underwent mitral replacement owing to paravalvular leakage of the previously implanted MV. In the non-repair group, one patient underwent mitral replacement owing to infective endocarditis and one underwent aortic valve repair owing to rheumatic aortic regurgitation. There were no significant between-group differences in the incidences of stroke, non-TV reoperation, anticoagulation-related haemorrhage and infective endocarditis.
Secondary end point: echocardiographic assessment of postoperative TV function and its influence on late outcomes
Of the 234 early survivors, 206 (88.0%) were echocardiographically followed up for more than 6 months (median 29.3 months, range 6.0–136.8 months, IQR 12.7–69.8 months), 109 in the repair group and 97 in the non-repair group (p=0.56). Overall, 991 echocardiographic assessments (mean, 4.2 per patient) were analysed.
A total of 34 patients (14.4%), six in the repair and 28 in the non-repair group, experienced moderate-to-severe TR during follow-up. The 5-year rates of freedom from moderate-to-severe TR were 92.9±2.9% in the repair group and 60.8±6.9% in the non-repair group (p<0.001; figure 2A). Regardless of preoperative degree of TR, the repair group showed better rates of freedom from significant TR than the non-repair group (figure 2B,C). When the cumulative incidence of postoperative TR was adjusted using IPTW, patients in the repair group were at a significantly lower risk of developing significant TR than patients in the non-repair group (HR=0.32, 95% CI 0.11 to 0.99; p=0.048).

Freedom from postoperative moderate-to-severe TR in the repair and non-repair groups. (A) Entire cohort. (B) Subgroup of patients with preoperative mild TR. (C) Subgroup of patients with preoperative moderate TR. TR, tricuspid regurgitation.
Multivariable analysis showed that not performing TV repair (p<0.001) and advanced age (p=0.002) were independent risk factors for postoperative significant TR (table 3).
Univariable and multivariable risk factor analyses for postoperative moderate-to-severe tricuspid regurgitation
Figure 3 shows the unadjusted Kaplan–Meier curves of clinical end points according to the presence of postoperative moderate-to-severe TR. On unadjusted comparisons, patients with postoperative significant TR had similar risks of death (p=0.89) and CHF (p=0.69), but significantly greater risks of TV reoperation (p<0.001) and the composite of primary end points (p=0.020) than patients without postoperative significant TR.

{kind=link}
{kind=link}
{kind=link}
Unadjusted (A–C) and adjusted (D) survival curves of clinical end points relative to the presence of postoperative moderate-to-severe TR. (A) Overall survival. (B) Freedom from tricuspid valve reoperation. (C) Freedom from composite of death, tricuspid valve reoperation and congestive heart failure requiring readmission. (D) Adjusted freedom from composite of death, tricuspid valve reoperation and congestive heart failure requiring readmission. CHF, congestive heart failure; TR, tricuspid regurgitation; TV, tricuspid valve.
When the effects of postoperative significant TR on clinical outcomes were adjusted using time-updated Cox models, the presence of TR was significantly associated with the composite of death and cardiac-related complications (HR=2.90, 95% CI 1.06 to 7.73, p=0.038), and with advanced age (HR=1.06, 95% CI 1.04 to 1.18, p=0.002) (figure 3D).
In the repair group, the 5-year freedom from significant TR rates was similar in the 54 patients who underwent ring annuloplasty (89.3±5.3%) and in the 69 patients who underwent suture annuloplasty (94.0±3.4%, p=0.46), indicating that the use of ring annuloplasty did not significantly affect postoperative TV function.
Discussion
We have shown here that although TV repair did not significantly decrease the incidence of adverse clinical outcomes, it was effective in improving postoperative TV function in patients with mild-to-moderate TR undergoing MV replacement for rheumatic MV diseases. TV repair had a beneficial effect on postoperative TV function, regardless of whether preoperative TR degree was mild or moderate. Furthermore, significant postoperative TR was associated with poor long-term outcomes.
As the left atrial and pulmonary arterial pressure increase over time secondary to MV diseases, longstanding pressure overload to the right ventricle induces right ventricular enlargement, tricuspid annular dilatation and leaflet tethering, especially in patients who develop right ventricular dysfunction.8 18 19 These pathological changes on TV geometry cause functional TR, with a prevalence of about 20–30% in patients undergoing MV surgery.20–22
Although concomitant TV repair has been less commonly performed owing to findings that functional TR frequently improves after successful correction of MV disease,2 8 recent evidence suggests that TV repair should be considered when functional TR is severe, because uncorrected functional TR is associated with poor long-term clinical outcomes.1 20–23 The 2006 American College of Cardiology/American Heart Association guidelines for the management of patients with valvular heart disease indicate that TV repair is beneficial for severe TR in patients requiring MV surgery (recommendation class I, level of evidence B).4 These guidelines, however, highlight the paucity of data on whether surgical correction of TR is indicated for patients undergoing MV surgery when the TR is less than severe (class IIb, level of evidence C).
A significant proportion of patients is reported to develop moderate-to-severe TR after left heart valve surgery if TR is left untreated even if the TR is mild. Matsuyama et al reported their series of 174 patients undergoing mitral surgery without TV repair.10 During a mean follow-up of 8.2 years, 16% patients experienced moderate-to severe TR.
In a retrospective study involving 638 patients who had less than moderate functional TR undergoing left-side heart surgery without TV surgery, late significant TR was detected in 7.7% of patients during a mean follow-up period of 64 months.24 Patients who developed significant TR had poorer event-free survival than those without significant TR. As several factors were predictive of late significant TR, the authors suggested performing TV repair in selected patients with these risk factors even in mild TR. Since the severity of TR is dependent on right ventricular haemodynamics, a group suggested considering TV annular diameter as a criterion of concomitant TV surgery rather than presence of TR itself.25 In their series of 311 patients, 48% had TV annular dilatation (>70 mm in diameter), for which concomitant TV repair was routinely performed.26 Concomitant TV repair improved postoperative functional status and TV function.
Calafiore et al reported their series of 110 patients who underwent mitral surgery in the presence of moderate-to-severe TR.27 TR was treated with annuloplasty technique in 51 and untreated in 59. During a median follow-up of 68–85 months, untreated TR emerged as a significant risk factor for poor survival and symptom-free survival. In another study on the impact of TV repair for functional TR in patients undergoing MV replacement, concomitant TV repair prevented TR progression and CHF in patients.28 Of note, the present study did not show differences in survival or incidence of CHF between the repair and non-repair groups. The discrepancies in the influence of TV repair on survival or CHF between this study and the cited studies are probably attributable to different study populations. Inclusion of patients with severe TR may have magnified the effect of TV repair on clinical outcomes in the cited studies. Since there is a general consensus for performing TV repair for severe TR in patients undergoing MV surgery, we did not include patients with severe TR, a difference that may explain the discrepancy regarding the preventive effects of TV repair on adverse outcomes.
Although ring annuloplasty has been reported to be better than suture annuloplasty for the repair of TR,29 we found that both techniques showed similar efficacy in restoring and maintaining TV function. Patients who had undergone suture annuloplasty had a more severe degree of TR—78.3% (54/69)—and 58.2% (32/55) of ring annuloplasty patients had moderate TR (p=0.023). Other preoperative profiles were quite similar for both groups, indicating that the condition of suture annuloplasty patients was no better than that of ring annuloplasty patients. The relatively short follow-up period may explain the similar results in TV function between the two techniques. However, this might also be attributed to differences in patient populations, in that our patients had only mild-to-moderate functional TR, such that suture annuloplasty without a ring device might have resulted in benefits similar to those of ring annuloplasty.9
TV repair durability is reported to be affected by technical completeness and also by preoperative degree of TV tethering, and postoperative ventricular function and pulmonary arterial pressure. Individuals with such risk factors may require close surveillance even after successful TV repair.30
Limitations
This study is subject to the limitations inherent in retrospective studies of observational data from a single centre. The non-randomised design might have affected our results owing to unmeasured confounders, procedure bias or detection bias, even with the use of rigorous statistical adjustment.
Sophisticated variables, such as tricuspid annular dimension, TV tethering distance and TV tethering area, could not be estimated, and right ventricular dysfunction was not quantified.
Although we found that TV repair decreased the incidence of postoperatively significant TR and that postoperative TR was associated with poor long-term outcomes, we did not demonstrate a direct relationship between TV repair and improved clinical outcomes. This may be because of the relatively small number of patients and events, limiting the statistical power of this study. Since late TR and heart failure may appear up to 10–20 years after the initial operation, studies on larger patient populations with longer follow-up might overcome this limitation.
Conclusions
Compared with MV replacement alone, concomitant TV repair was associated with better postoperative TV function in patients with mild-to-moderate functional TR undergoing MV replacement with mechanical prosthesis for rheumatic mitral diseases. These findings support the strategy of correcting mild-to-moderate functional TR at the time of MV replacement to maintain TV function, a strategy that may help to improve long-term clinical outcomes.
Acknowledgments
The authors thank Sung-Cheol Yun, PhD, from the Division of Biostatistics, Center for Medical Research and Information, University of Ulsan College of Medicine, for assistance with the statistical analyses.
References
Footnotes
Competing interests None.
Ethics approval Ethics approval was provided by the Asan Medical Center, Seoul, Korea.
Provenance and peer review Not commissioned; externally peer reviewed.