Article Text

Abstract
Two cases of transient acute cardiomyopathy occurring in the immediate aftermath of intense emotional stress and without any identified aetiology are described. These two case reports, mimicking cases of acute cardiomyopathy described in patients with pheochromocytoma, suggest the possibility in man of acute catecholamine induced cardiomyopathy related to major emotional stress alone, a phenomenon so far reported only in animal experimental models.
- acute cardiomyopathy
- catecholamines
- stress
Statistics from Altmetric.com
The myocardial toxicity of high concentration endogenous or exogenous catecholamines has been demonstrated in animal models as well as during pheochromocytoma crises that are responsible for acute cardiomyopathy. Animal experiments have shown that stress induced endogenous catecholamine secretion could entail myocardial lesions,1 although that possibility has never been demonstrated in man. We report two similar cases of transient acute cardiomyopathy occurring in the immediate aftermath of major emotional stress without any other identified aetiology.
Case 1
A 70 year old woman with no previous cardiac history was admitted to hospital as an emergency on 14 September 1993 because of sudden cardiovascular collapse. In the early hours following her husband’s sudden death she suffered intense, constrictive retrosternal chest pain that lasted approximately 30 minutes. She sustained chest discomfort with sweating, nausea, and vomiting, followed by another transient acute chest pain lasting approximately 15 minutes, with brief unconsciousness. On admission three hours after the onset of symptoms, she no longer felt any chest pain but presented with a polypnea-like dyspnoea. Clinical examination showed temperature was 37.2°C, blood pressure 90/70 mm Hg, heart rate 115 beats/min, limb ends were cold and cyanosed, mottling was visible on the lower limbs, and crepitations could be heard in both lung fields. ECG showed stable sinus tachycardia, undervolted QRS with no R wave progress from V1 to V3, and discrete repolarisation abnormalities with T wave flattening or inversion (fig 1A). Chest radiography revealed pulmonary oedema. Baseline creatine kinase concentration was normal, blood glucose was high (12.7 mmol/), and there was hyperleucocytosis (15 × 106 cells/l), and neutrophil polynucleosis. Echocardiography revealed major hypokinesia of the medium and apical segments of the anterior, lateral, septal, and inferior walls. Only basal segments retained normal contractility. Ejection fraction was about 20%.

Electrocardiograms recorded in patient 1 at admission (A), one day (B), and eight days (C) after admission, and after three years of follow up (D). (A) ECG shows R wave low amplitude in right precordial leads and T wave flattening or inversion in lateral and inferior leads. (B) and (C) Diffuse repolarisation abnormalities with QT interval prolongation and marked negative T waves (pseudoischaemic) are evident. Note that in (C) R wave amplitude in right precordial leads has returned to normal. (D) ECG is normal.
The patient was initially treated with intravenous dobutamine and diuretics. Clinical evolution was rapidly favourable, with restored haemodynamics and drug weaning in less than 48 hours. Right heart catheterisation 24 hours after symptom onset revealed very slightly elevated pressures: right atrium, 6 (10/5) mm Hg; right ventricle, 35–5 to 10 mm Hg; pulmonary artery, 35–15–20 mm Hg; pulmonary artery wedge, 14 (17/11) mm Hg. Cardiac index under dobutamine and dopamine (5 μg/kg/min of each) was 2.5 l/min/m2. Creatine kinase did not increase significantly on the three days following admission. Repeat ECG showed an evolution towards major and diffuse repolarisation abnormalities, with transient lengthening of the QT interval, pronounced negativity of T waves that persisted at discharge (day 10), and increased QRS amplitude (figs 1B and C). Left ventricular function gradually improved until near normal on day 7. However, a slight anterior and apical hypokinesia persisted on echocardiography and the ejection fraction was about 50%.
No definite aetiology was found. There was no history of infection in the previous days or weeks and there was no inflammatory syndrome. Coronary arteriography was normal and methylergometrine maleate test did not trigger any coronary spasm. Urinary metanephrine and normetanephrine concentrations measured over three consecutive days before discharge were in the normal ranges. Abdominal computed tomography did not reveal any surrenal abnormalities.
Three months after that episode her ECG was totally normal (fig 1D). Over 30 months of follow up, the patient remained fully asymptomatic.
Case 2
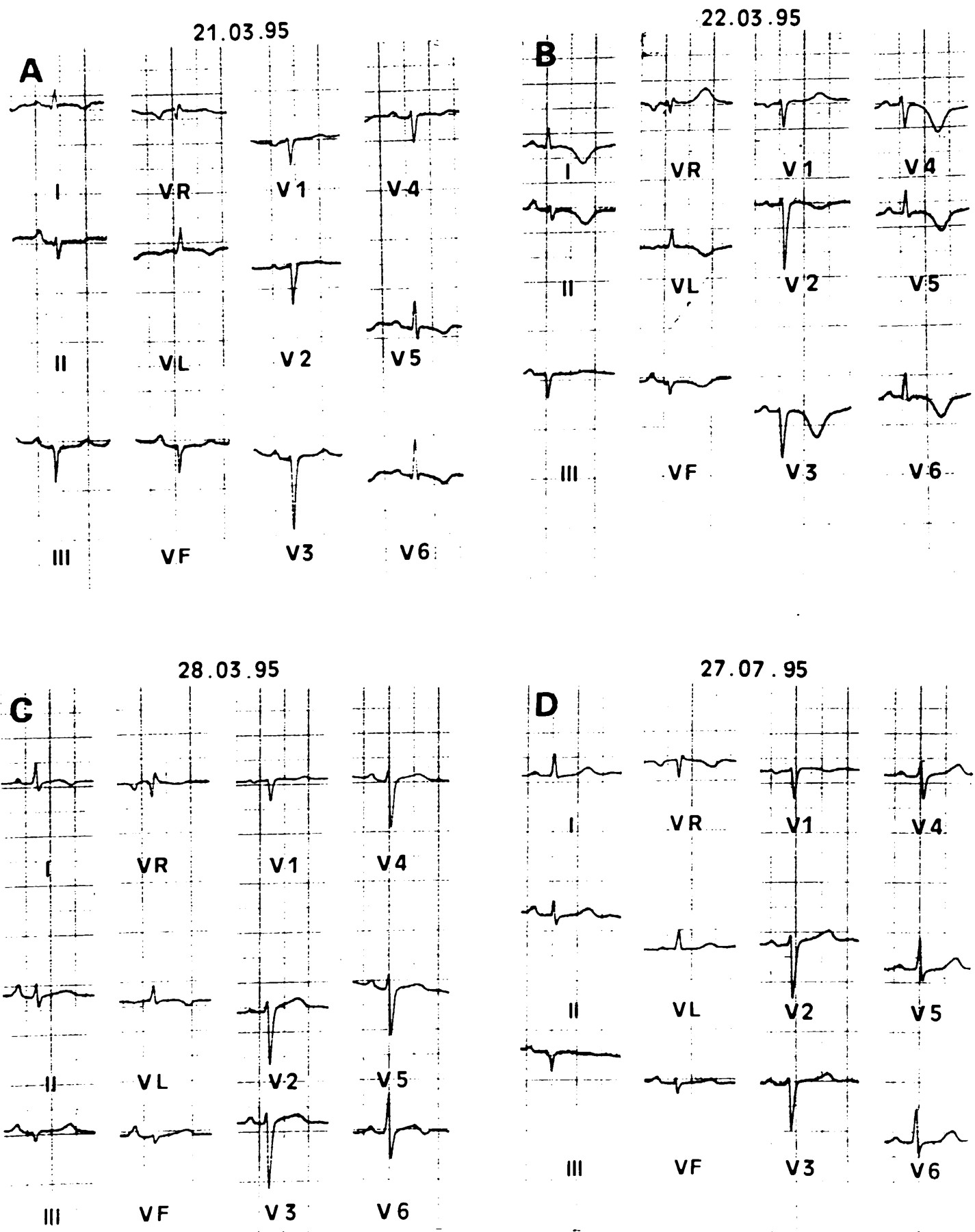
A 50 year old previously healthy woman presented in cardiac failure on 21 March 1995, a few hours after her son’s death by suicide. She first felt constrictive retrosternal chest pain radiating in the back and lasting about one hour at an intense level then gradually disappearing. It was accompanied by sweating, nausea, and vomiting. At admission, she exhibited polypnea-like dyspnoea, blood pressure was 80/50 mm Hg, heart rate 130 beats/min, and shock peripheral signs were evident with mottling and cyanosis. Her temperature was 37.1°C. Bilateral lung crepitations were heard at auscultation and chest radiography revealed pulmonary oedema. Total creatine kinase was initially normal and did not increase within the following three days. The only transient abnormalities found at routine biological work up were hyperglycaemia (12.1 mmol/l) and polymorphonuclear hyperleucocytosis (23 × 106/l). ECG revealed similar abnormalities as in the previous case, including sinus tachycardia, microvoltage, reduced R wave amplitude in right precordial leads, and diffuse repolarisation abnormalities. There was also a left axis deviation (fig 2A). Echocardiography showed a normally sized left ventricle whose function was severely altered by akinesia of the medium and apical segments of all walls, only the basal segments retaining their contractility. Ejection fraction was approximately 15%. On right heart catheterisation, performed at admission without any drug, pulmonary pressures appeared moderately high: right atrium, 6 (9/4) mm Hg; right ventricle, 34–3 to 6 mm Hg; pulmonary artery, 33–20–24 mm Hg; pulmonary artery wedge, 18 (23/16) mm Hg. Cardiac index was 2.9 l/min/m2.
{kind=link}
{kind=link}
Electrocardiograms recorded in patient 2 at admission (A), one day (B) and seven days (C) after admission, and after four months of follow up (D). Similar abnormalities and evolution as in figure 1 are seen with as well as left axis deviation. Pseudoischaemic repolarisation abnormalities are near normal at the end of the first week (C). (D) ECG is normal apart from a less important left axis deviation.
Her outcome was rapidly favourable with diuretic treatment, and signs of cardiac failure disappeared in less than 24 hours. Blood catecholamines were measured approximately eight hours after admission (almost 12 hours after the initial stress) and on the two following days, which revealed raised adrenaline and noradrenaline concentrations. At eight hours adrenaline was 228 pg/ml (normal < 50), noradrenaline, 887 pg/ml (normal < 350); on day 2 adrenaline was 101 pg/ml, noradrenaline 1011 pg/ml; on day 3 adrenaline was 50 pg/ml, noradrenaline, 429 pg/ml. Subsequent ECG revealed diffuse, ample, and sharp T wave inversion that gradually returned to normal (figs 2B and C). Ventricular function improved and only apical hypokinesia persisted at echocardiography on day 8. Ejection fraction was approximately 55%.
No definite aetiology was found. Coronary arteriography and methylergometrine test were normal. There was no history of infection of inflammatory syndrome. Urine catecholamines, measured over three consecutive days, surrenal computed tomography, and I131MIBG scintigraphy were normal.
Three months after that episode, the patient was well. ECG was normal (fig 2D) and the left ventricular function appeared normal on echocardiography
Discussion
These two cases describe peculiar acute cardiomyopathy, probably occurring under the influence of the catecholamine excess related to intense emotional stress. Their clinical characteristics and outcome were very similar and included:
sudden onset immediately following intense emotional stress
chest pain associated with sweating, nausea, and vomiting followed quickly by a state of shock with marked peripheral signs
acute respiratory distress related to severe pulmonary oedema that contrasted with the moderate rise in pulmonary capillary pressure, indicative of mixed cardiogenic and lesional origins
major impairment in myocardial contractility sparing the basal left ventricular segments, without any ventricular dilatation, and almost entirely reversed within a few days
diffuse, evolutive, and entirely reversible changes of the ECG, mimicking ischaemia
rapidly favourable outcome and recovery with hardly any sequelae.
No definite aetiology was found; coronary artery disease, myocarditis, and pheochromocytoma were ruled out. Beside the circumstances at onset, following intense emotional stress, the catecholamine induced characteristic of cardiomyopathy was suggested by its similarity with certain forms of cardiomyopathies described in relation to pheochromocytoma.
In that pathology, as well as dilated or hypertrophic cardiomyopathies that are probably linked to hypertension, authentic acute cardiomyopathies secondary to catecholamine release during a pheochromocytoma crisis have been described. In that model, the clinical pattern is often pejorative, with circulatory collapse and mixed pulmonary oedema, partly cardiogenic and partly linked to the direct effects of catecholamines on pulmonary vascularisation.2 Pulmonary sympathetic stimulation indeed increases the pore size in the pulmonary capillaries, leading to pulmonary alveolar transudation.3 Left ventricular dysfunction exhibits the same characteristics as in our two cases4 ,5: as a rule, the left ventricle is not dilated in those acute forms; the impairment of the left ventricular contractility is marked but spares basal segments, which may mimic extensive apical myocardial infarction; and it is reversible after recovery by removing the surrenal tumour. ECG changes, also reversible, can be mistaken for those found during acute coronary syndromes, affecting repolarisation with T wave flattening, lengthening of the QT interval, and even ST segment elevation.5 ,6 However, they are characterised by their diffusiveness that may extend to circumferential impairment.
In catecholamine induced cardiomyopathies linked to pheochomocytoma, myocardial lesions consist of a degeneration and focal necrosis of cardiac myocytes, secondarily associated with inflammatory reaction and fibrosis. However, the characteristic lesion is a particular myofibrillar degeneration called contraction band necrosis. Although, to our knowledge, no case of stress related catecholamine induced cardiomyopathy has been reported, experimental and even clinical data suggest their existence. Focal myocardial necrosis or myofibrillar degeneration lesions identical to those described here have been seen in experimental animal models subjected to major stress,1as well as in human models, especially during necropsies of patients dying suddenly by homicide following physical assault without directly lethal lesions.7
The pathogenesis of catecholamine induced cardiomyopathies is probably multifactorial. Excessive catecholamines may induce coronary vasoconstriction that leads to hypoxia and may explain the fact that the lesions are predominantly at the left ventricle apex, an area of distal coronary vascularisation.8 It has been clearly demonstrated, experimentally, that excessive exogenous or endogenous catecholamines (following stress in animals for the latter) modify sarcolemma permeability and severely increase sarcoplasm calcium concentration, which leads to myocyte necrosis.1 The reversibility of the lesions would be related to the shortness of myocardial exposure to excessive catecholamines, resulting in a state of stunning with cellular metabolic abnormalities rather than necrosis proper.
These two clinical cases, combined with certain experimental literature results, suggest the existence of acute catecholamine induced cardiomyopathies essentially related to stress in man.
Linked Articles
- Miscellanea