Article Text

Abstract
The role of viruses in the genesis of both dilated cardiomyopathy (DCM) and acute myocarditis remains uncertain. Modern molecular techniques such as polymerase chain reaction (PCR) and in situ hybridisation are sensitive means of detecting viral genomic material in human myocardial tissue and may help to resolve the quest. Meta-analysis of the papers in the literature records studies of both acute myocarditis and DCM where molecular techniques were used to demonstrate enteroviruses. This review studies information from the published literature as well as statistical analysis of the cumulative molecular data relating enteroviruses to DCM, and to compare these findings with the information available on the role of enteroviruses in acute myocarditis. Twelve papers reported studies in acute myocarditis, of which 11 found higher percentages of enteroviral RNA positivity in the diseased population, giving an overall odds ratio of 4.4. Seventeen papers reported studies in DCM, with 11 recording higher positivity rates in these patients. Cumulative analysis of these data suggests an overall odds ratio of 3.8. The causative role of enteroviruses in acute myocarditis, particularly in children, is supported by meta-analysis of the available literature. The data on DCM is suggestive of an association but a proportion of the studies are negative.
- enteroviruses
- dilated cardiomyopathy
- myocarditis
- meta-analyses
Statistics from Altmetric.com
Reports of an association between enteroviruses and myocarditis date back to 1956 when coxsackie B4 virus was isolated from the heart tissue of a neonate with fatal infection.1 Four decades later debate continues on the role of enteroviruses in acute and chronic myocardial disease.
Coxsackie B viruses are ubiquitous enteroviruses that spread rapidly within the community causing small epidemics with a high proportion of subclinical cases. Symptomatic infection ranges in severity from mild undifferentiated febrile illness or upper respiratory tract infection to severe systemic disease of neonates. Historically, it was the childhood cases of myocarditis that attracted attention to this group of agents.1-4 Early reports of epidemics in maternity homes where virus was isolated from peripheral sites of neonates,2 ,3 were followed by studies confirming the presence of coxsackieviruses in the heart tissue of infants with myocarditis.1 ,5 Later work showed that infection during pregnancy may result in fetal damage6-8 and large scale serological studies confirmed that mothers of infants with cardiological abnormalities were more likely to be infected with coxsackievirus B than were controls.4
Studies of a causal link between enteroviruses and adult cases of myocarditis proved more difficult. Virus isolation from adult heart tissue is very uncommon,9-11 and until recently many epidemiological studies relied on either virus culture from peripheral sites or serological investigations for diagnosis. As enteroviruses circulate freely in the community and virus can be cultured from the pharynx and faeces for several weeks following infection, diagnostic value cannot be attached to virus isolation from these sites. Serological studies are also fraught with difficulties as high titre antibodies can persist for prolonged periods in some individuals. Moreover, unlike young children, adults with prior exposure to enteroviruses may show a heterotypic rise in antibody titres confusing the diagnosis. Despite these problems, comparison of recent serological studies12-14 shows that 33–36% of adults with acute myocarditis have either rising titres of neutralising antibodies to coxsackie B viruses or have enterovirus specific IgM class antibodies indicative of a recent infection. The rate of infection in the control groups in these reports varies between 4% and 10%.
The advent of molecular techniques for the detection of viral RNA facilitated studies of heart tissue in non-fatal cases, providing an indication of the prevalence of these agents in acute myocarditis. Using in situ hybridisation, Hilton et al found 20% of childhood cases of acute myocarditis to carry enteroviral RNA in heart tissue.15 This result was confirmed by Martin et al who, using polymerase chain reaction (PCR), found eight of 38 heart biopsies taken from children with acute myocarditis and none of 17 controls carried enteroviral sequences.16Recent work by Towbin et al has extended these findings and shown that 23 of 135 paediatric patients were enterovirus positive by PCR.17
The benefits of using molecular techniques were of particular importance in studies of adult cases of myocarditis. Some of the difficulties associated with the traditional methods of diagnosis were overcome with the widespread use of PCR. Although diverse rates of viral RNA detection in heart tissue have been reported,18 ,19 there is now general agreement that there is an association between coxsackievirus B infection and myocarditis. The techniques applied to the study of viral aetiology in acute disease have also been used in the study of dilated cardiomyopathy (DCM). It is the aim of this report to study information from the published literature and carry out statistical analysis of the cumulative molecular data relating enteroviruses to DCM and compare these findings with the information available on the role of enteroviruses in acute myocarditis.
Methods
Analysis of the literature that records the use of molecular biological techniques such as PCR and in situ hybridisation for the detection of viral genomic material in acute myocarditis and DCM was carried out. Totally negative studies were included but those without a control group were excluded. The results were expressed as bar charts showing the percentage of samples found to be positive and the standard error of the binomial distribution.
Results
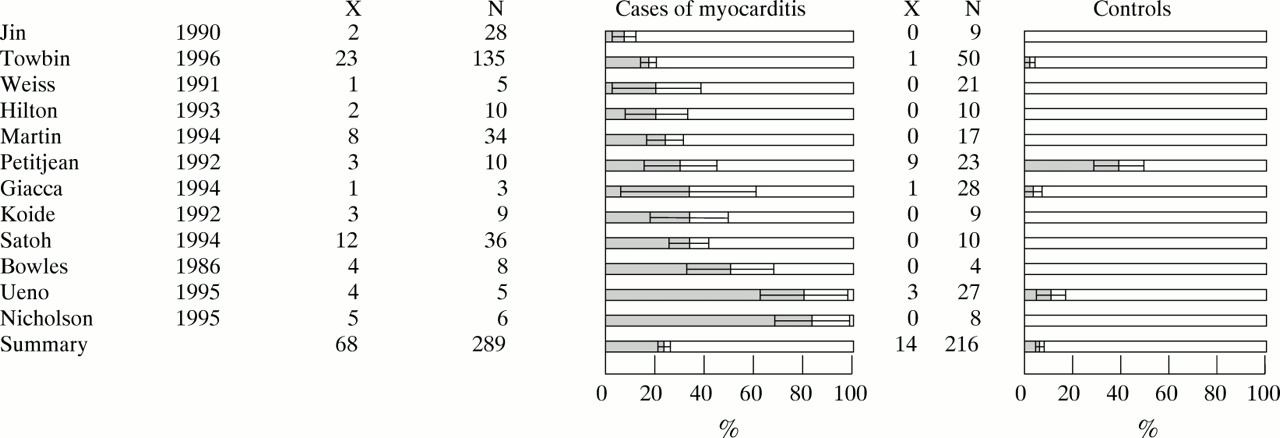
In acute myocarditis, analysis of the molecular data for both adult and childhood cases shows that 11 of 12 studies reviewed record a higher number of patients with myocarditis positive for viral genomic material compared with controls (fig 1).15-26 The cumulative data from these studies shows that 23% of patients with disease (68 of 289 cases) and 6% of controls (14 of 216 individuals studied) were positive for enteroviral sequences, giving an odds ratio of 4.4 (95% confidence interval (CI), 2.4 to 8.2).
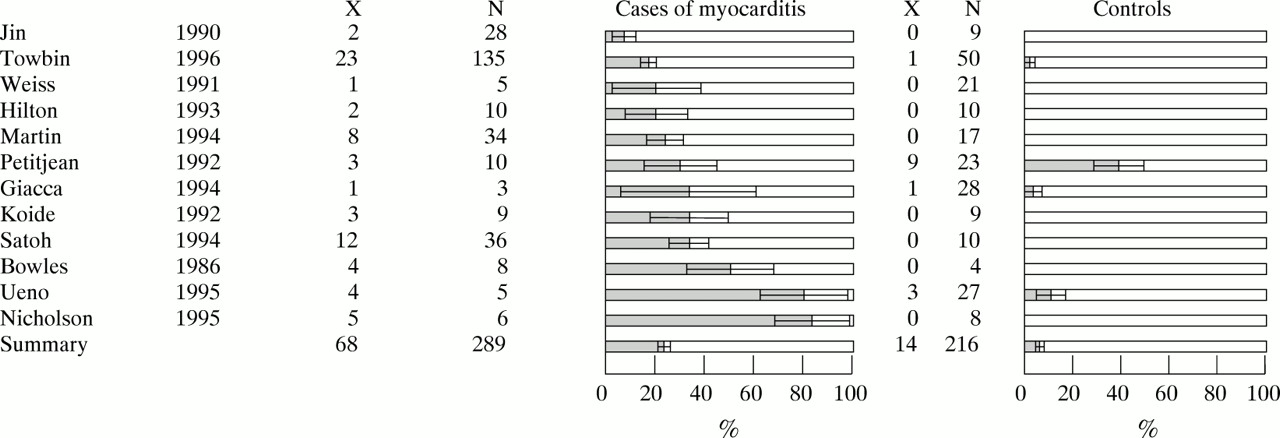
Evidence for association of enteroviruses with idiopathic myocarditis. The bar charts show the percentage of samples found to be positive with error bars showing the standard error of the binomial distribution. (X is the number of samples with enteroviral sequences and N the total number studied.)
Figure 2 summarises most recent studies of DCM where patients and control groups have been compared using molecular tech- niques.18 ,20-22 25-37 Overall, 406 patients with DCM and 438 control subjects have been investigated with approximately 23% of the patients and 7% of controls showing evidence of enteroviral infection. The odds ratio was calculated to be 3.8 (95% CI, 2.1 to 4.6). The percentage positivity in patients with DCM varied between 0%20 ,27 ,28 and 75%.37

{kind=link}
{kind=link}
Evidence for association of enteroviruses with dilated cardiomyopathy. The bar charts show the percentage of samples found to be positive with error bars showing the standard error of the binomial distribution. (X is the number of samples with enteroviral sequences and N the total number studied.)
Discussion
Although an odds ratio of 3.8 is suggestive of an association between virus infection and DCM, on closer analysis, six of 17 reports found no significant differences between cases and controls (fig 2). Other studies included in this report used small numbers of patients making statistical analysis of the data difficult. Three of these investigations that found 20%, 28%, and 75% viral RNA carriage rates in the DCM group and no enteroviral sequences in the controls, included fewer than 10 patients.25 ,31 ,37 Five of the eight remaining reports that used PCR to detect viral material did not sequence the amplification products. As the amplification procedure is particularly prone to contamination, often from the reference strain used in the laboratory, sequencing of the products is informative, confirming the origin of the virus. In one study where sequencing was undertaken the amplification products were found to be identical to the coxsackevirus B3 positive control used in the routine assay.22 In another carefully controlled study where fivefold differences in enteroviral RNA positivity were recorded with sequencing data confirming the results, patients with inflammatory heart disease were grouped together with cases of DCM.35Although this study has been included in the overall analysis of the role of enteroviruses in DCM, it is by no means certain that the positive patients were not cases of acute myocarditis.
A factor that further influences the interpretation of these studies is the choice of controls. As enteroviruses cause small epidemics there is likely to be variation in the virus carriage rates in different populations. In studies where serological analysis have been carried out often a significant difference in the IgM positivity rates between patients with DCM and controls have been observed.29 ,38 ,39 However, Keeling et alfound that if the serological status of patients was compared with their own family members or close associates then 37% of the disease population and 28% of the controls were IgM positive.38Taking into account the numbers involved in each group a relative risk of 1.5 can be deducted. In the same study risk seemed much higher if patients were compared with an unselected control population (33% of the patients with DCM and 5% of the controls). When conducting serological investigations it is possible to obtain samples from close relatives or work associates exposed to the same environment and therefore likely to have experienced similar infections. Such comparisons are impossible when heart biopsy samples are analysed for viral RNA. Epidemiological data on unmatched groups, for a virus known to cause small local epidemics, may therefore be biased.
The studies cited here and numerous case reports based on traditional virus isolation, serology, and molecular techniques have strengthened the belief that there is a link between myocarditis and enterovirus infections. The relation between these viruses and chronic heart disease however remains uncertain. There are reports of coxsackievirus infections in mice resulting in histological changes resembling congestive cardiomyopathy40 and in hamsters resulting in cardiomegaly.41 Experimental work in animals has otherwise been mainly concerned with the study of myocarditis and the mechanisms of induction of disease during the acute phase of illness. Although there are animal models of DCM, these are on the whole hereditary42 or chemically induced cases.43-46 There is a paucity of experimental data on the possible progression of disease from viral myocarditis to DCM.
If enteroviruses are involved in DCM, the question arises as to the mechanism of such damage. Large scale cell death as a consequence of lytic viral infection is unlikely to cause the symptoms, as the proportion of cells infected with virus would be higher than that observed using the in situ hybridisation method.29 Indeed a number of studies have resorted to the very sensitive technique of nested PCR22 ,35 for viral detection, suggesting that by the stage clinical symptoms of DCM become apparent, the quantity of persistent RNA in the heart tissue is either small or localised. While the pathological changes seen in acute myocarditis are compatible with injury caused as a consequence of infection with a lytic virus and the immune response following such infection, the structural alterations required at cellular level to cause DCM are more difficult to interpret in the context of a viral disease. Immune mediated damage to the heart as a mechanism of pathogenesis for DCM is at present speculative. Studies in mice have shown that coxsackieviruses are able to lyse myocytes47 with maximal myocyte damage occurring either concurrently with the highest virus titres, in the case of coxsackievirus B1 and B4,48 or with the initiation of an immune response following coxsackievirus B3 infection.49It is feasible therefore that virus may cause damage either by rapid necrosis of the heart tissue or by a more subtle immunological mechanism. As virus slowly replicates and moves from cell to cell, infected areas of the tissue may be progressively destroyed by the action of cytotoxic T lymphocytes. The interaction between persistent infection and immune response to the agent may cause sufficient cellular damage to initiate disease. Experimental studies in mice have shown that different components of the immune system play a role in the survival of the infected animals. Mice lacking CD4 positive cells are more likely to develop myocarditis but those without functional T cytotoxic cells survive longer50 and are less likely to develop myocarditis. Which component of the immune response is most active during a low grade infection in man and against which viral proteins is at present unknown.
An alternative hypotheses for which there is some epidemiological and experimental evidence is the possibility that infection with enteroviruses may trigger an exaggerated immune response not only to the viral antigens but to the host tissue. Experimental work on mice with severe combined immunodeficiency has shown that transfer of peripheral blood leucocytes of patients with chronic myocarditis to these animals causes an impairment of left ventricular function51 suggesting a cell mediated autoimmune response in the patient. Damage by autoantibodies has also been considered with a number of studies reporting higher frequencies of antibodies directed against cardiac myosin in patients with DCM.52 ,53 Whether these antibodies cause cellular damage is unknown.
The precise role of each viral strain in acute or chronic infection is also uncertain. Virus isolations from fatal cases of myocarditis provide information on the serotype of the agent involved but do not give an indication of the incidence of myocarditis following infection with these commonly occurring viruses. On the other hand, most studies that have compared diseased heart tissue with controls using molecular techniques have employed group specific primers and probes, and have not attempted to distinguish between different members of the enterovirus family.18 ,26 ,30 ,36 ,37 Experimental work on mice has shown that some strains of coxsackievirus B3 are more cardiovirulent than others54 and that pathogenicity may differ significantly not only between clinical isolates but also in different species or strains of animals.55
Acknowledgments
This research was supported by a grant from the British Heart Foundation. The authors thank Jocelyn Lovegrove for statistical advice.