Article Text

Abstract
Objective To assess the occurrence of arterial remodelling types and its relation with the severity of luminal stenosis in atherosclerotic coronary arteries.
Patients and methods Twenty one de novo coronary lesions of 20 patients, who were scheduled for percutaneous transluminal coronary angioplasty (PTCA), were investigated with intravascular ultrasound before PTCA. Local arterial remodelling at the lesion site was studied by measuring the cross sectional area circumscribed by the external elastic lamina (EEL) relative to the reference site: (EEL area lesion/reference EEL area) × 100%. Three groups were defined. Group A: relative EEL area of less than 95% (shrinkage), group B: relative EEL area between 95% and 105% (no remodelling), group C: relative increase in EEL area of more than 105% (compensatory enlargement).
Results All three types of remodelling were observed at the lesion site: group A (shrinkage) n = 8, group B (no remodelling) n = 5, group C (compensatory enlargement) n = 8. The mean (SD) relative EEL area at the lesion site in group A and C was 83(9)% and 132(30)%, respectively. In group A, 33% of the luminal area stenosis at the lesion site was caused by shrinkage of the artery. In contrast, group C showed that 87% of the plaque area did not contribute to luminal area stenosis because of compensatory arterial enlargement.
Conclusions These results show that both compensatory enlargement and paradoxical shrinkage occurs in the atherosclerotic coronary artery. Next to plaque accumulation, the type of atherosclerotic remodelling is an important determinant of luminal narrowing.
- coronary arteries
- atherosclerosis
- remodelling
- intravascular ultrasound
Statistics from Altmetric.com
It has been shown by Glagov1 and Zarins et al 2 that adaptive vessel wall enlargement in response to plaque accumulation occurs in the left main and left anterior descending coronary artery. Histopathological3and intravascular ultrasound studies3-5 have shown that this process of compensatory enlargement is not limited to the left coronary artery. Pasterkamp et al 3 have shown that in the femoral artery paradoxical arterial wall shrinkage may be observed as well. Compensatory enlargement was mainly operative in arteries with less than 25% luminal area stenosis, whereas shrinkage of the vessel wall was predominant in arteries with more than 25% luminal area stenosis. Therefore, arterial wall shrinkage may accelerate lumen narrowing in atherosclerosis. This seems to be a different mechanism of lumen obliteration than plaque formation alone and may illuminate new insights on atherosclerosis and its treatment. To determine if arterial wall shrinkage is also present in the atherosclerotic coronary artery, we performed an intravascular ultrasound study in patients before percutaneous transluminal coronary angioplasty (PTCA). Furthermore, we investigated the relation between the type of arterial wall remodelling and the severity of luminal area stenosis.
Methods
STUDY POPULATION
Twenty three patients (16 men, 7 women; mean (SD) age 59 (9)) were selected for an intravascular ultrasound study before a scheduled PTCA procedure. Only patients with single or double coronary artery disease and a significant stenosis in the proximal or mid coronary artery segment on coronary angiography were selected. Twenty four de novo atherosclerotic lesions were studied. All patients had angina pectoris class II–IV, classified according to the New York Heart Association criteria.6 Informed consent was obtained from each patient before the intravascular ultrasound procedure.
INTRAVASCULAR ULTRASOUND SYSTEM AND IMAGING PROCEDURE
The intravascular ultrasound procedures were performed with the Cardiovascular Imaging System (CVIS, Sunnyvale, California) coupled to a 2.9 F MicroView 30 MHz coronary imaging catheter (CVIS, Sunnyvale, California). This mono-rail imaging catheter consists of a single rotating 30 MHz ultrasonic transducer at the distal end of a rotating drive shaft. After coronary angiography the selected lesion was crossed with the imaging catheter over a 0.014 inch guidewire. Then the guidewire was retracted and the transducer advanced into the echolucent distal shaft (14.5 cm length) of the catheter. Intravascular ultrasound images were obtained by slowly moving the transducer inside the echolucent shaft of the catheter back and forth across the lesion and its adjacent segments. Simultaneously with fluoroscopy, the intravascular ultrasound images and voices of the physicians were recorded on two high resolution S-VHS video tapes for offline analysis. For optimal correlation between the fluoroscopy and intravascular ultrasound images a time code was added to each signal by two synchronised video frame counters, or both video signals were online mixed into one signal and recorded.
QUANTITATIVE INTRAVASCULAR ULTRASOUND MEASUREMENTS
The intravascular ultrasound images were analysed with a digital analyser as described previously.7 In each stenosed arterial segment, three sites were selected for quantitative intravascular ultrasound analysis. The site with the most severe lumen obliteration on the intravascular ultrasound images and two reference sites in each proximal and distal adjacent segment were taken. The reference sites had no side branches in between and had no or minimal lumen narrowing on angiography and intravascular ultrasound.
In the three cross sections we traced the lumen area (mm2) and the area circumscribed by the external elastic lamina (EEL area) (mm2). The external elastic lamina was defined as the outer border of the echolucent zone, which represents the interface between media and adventitia.8 ,9 The media and atherosclerotic plaque area was defined as plaque area (mm2) and calculated by subtracting the lumen area from the EEL area. Reduction of the lumen area at the lesion site could theoretically result from plaque area increase or reduction of the EEL area (arterial wall shrinkage). To compare EEL area at the lesion with its reference area we defined the reference EEL area (EEL ref) as (EEL area proximal + EEL area distal)/2. When proximal or distal side branches were present adjacent to the lesion, only the EEL area distally or proximally of the lesion was taken respectively. When large amounts of plaque were seen adjacent to the lesion only the EEL area with no or minimal plaque was used for further calculations. Arterial wall remodelling was studied by the change in EEL area (relative EEL area) and calculated as: (EEL area lesion/EEL ref area) × 100%. The lesions were divided into three groups based on the change of EEL area. Group A: decrease in EEL area of more than 5% (shrinkage), group B: change in EEL area between −5% and 5% (no remodelling), group C: increase in EEL area of more than 5% (compensatory enlargement).10 Plaque contribution was defined as percentage plaque area increase to luminal area decrease at the stenosis in comparison with its reference sites and calculated by: (plaque area stenosis − plaque area reference)/(lumen area reference − lumen area stenosis) × 100%. Per cent luminal stenosis was calculated as (1−(lumen area lesion/lumen area reference)) × 100%.
SELECTED ABBREVIATIONS AND DEFINITIONS
EEL area = area encompassed by the echodense adventitial layer. EEL area ref = (EEL area proximal + EEL area distal)/2. Relative EEL area = (EEL area lesion/EEL area ref) × 100%. Luminal stenosis = (1 − (lumen area lesion/lumen area reference)) × 100%. Plaque contribution = (plaque area stenosis − plaque area reference)/(lumen area reference − lumen area stenosis) × 100%.
STATISTICAL ANALYSIS
All values are presented as mean (SD). Comparison of data among the three different groups was performed using ordinary one way analysis of variance with Duncan range test at the post hoc test in both comparisons. A p value of less than 0.05 was considered statistically significant.
Results
Three lesions (three patients) were excluded from analysis because of insufficient intravascular image quality caused by calcification (n = 2), or more than 50% luminal stenosis by plaque in the reference sites (n = 1). Final analysis was performed on 21 lesions in 20 patients (15 male, five female; mean (SD) age 59 (9)). Table 1lists the patient and lesion characteristics.
Patient characteristics
All three types of remodelling were observed at the lesion site: group A (shrinkage) n = 8, group B (no remodelling) n = 5, group C (compensatory enlargement) n = 8. Figures 1 and 2 show intravascular image examples of arterial shrinkage and compensatory enlargement, respectively. Table 2 lists the intravascular ultrasound characteristics. No statistical differences were present between the reference cross sectional areas in the different three groups. Group A showed a mean (SD) shrinkage of the vessel of 17(9)%, whereas group C showed a mean enlargement of 32(30)%
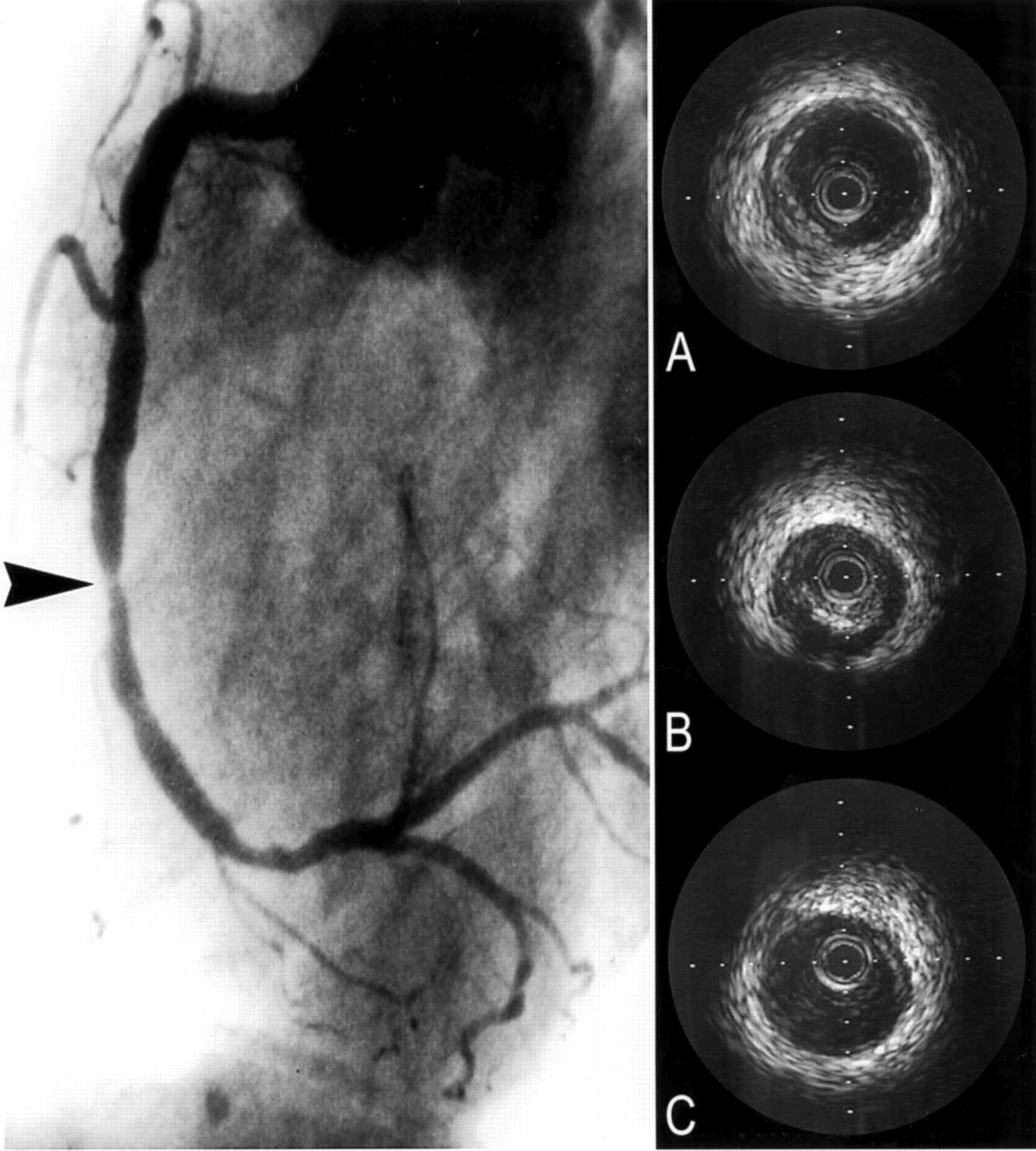
Angiogram and intravascular ultrasound images of the right coronary artery in one patient. The arrow indicates the lesion. The intravascular ultrasound images show the proximal reference (A), lesion (B), and distal reference (C) site. At the lesion site arterial shrinkage is present.
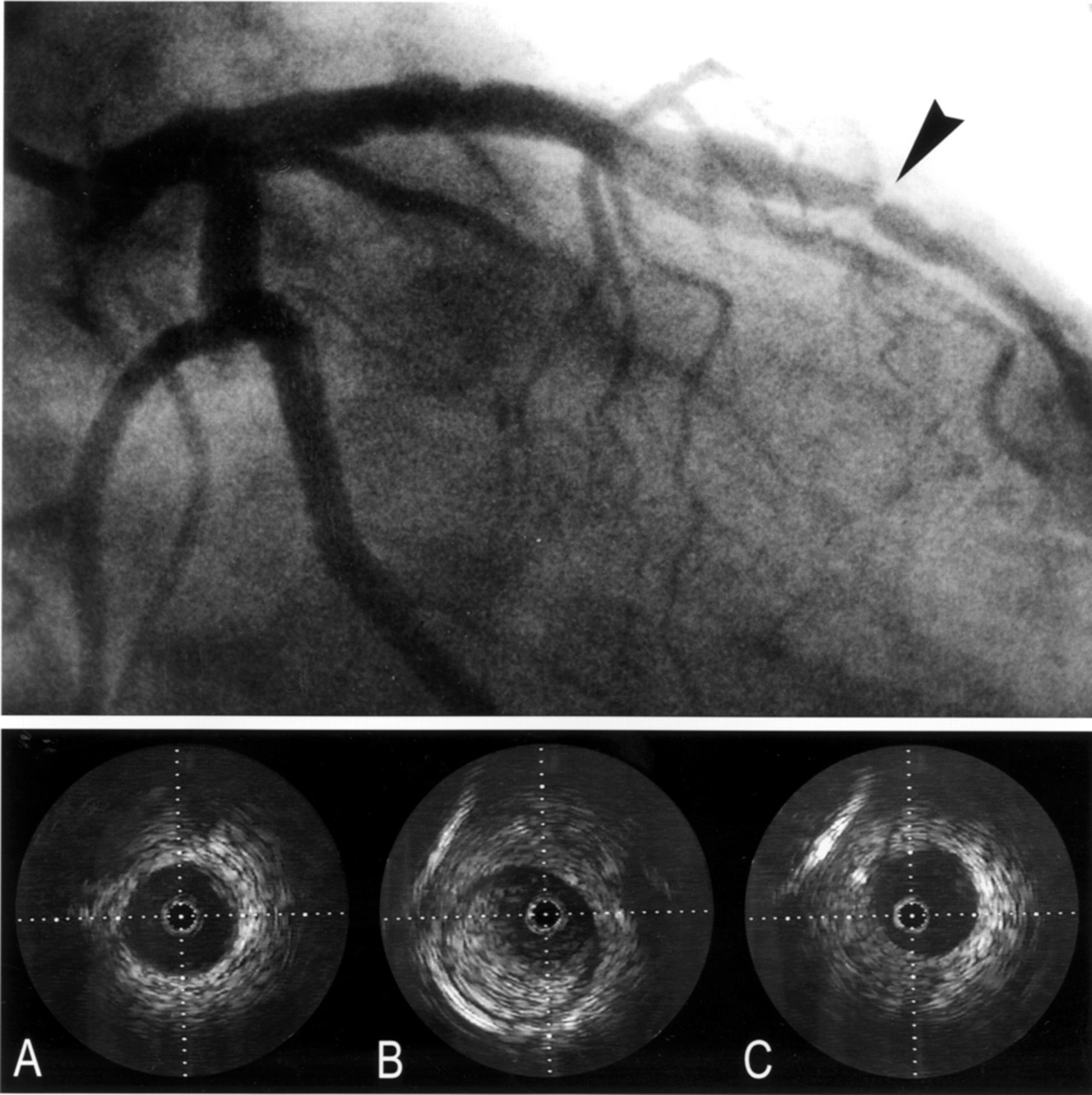
Angiogram and intravascular ultrasound images of the left anterior descending coronary artery in another patient. The arrow indicates the lesion. The intravascular ultrasound images show the proximal reference (A), lesion (B), and distal reference (C) site. At the lesion site arterial compensatory enlargement is present.
Baseline intravascular ultrasound (IVUS) results
In group A, plaque contribution to the lumen area stenosis at the lesion site was 67% and shrinkage of the arterial wall attributed for the remaining 33%. Whereas in group C, plaque contribution to the stenosis at the lesion site was 187%, resulting from a 87% lumen area increase by compensatory enlargement (fig 3).

{kind=link}
{kind=link}
{kind=link}
This bar graph represents the average percentage plaque contribution (grey bar) and the percentage remodelling contribution (white bar) to the luminal area at the lesion site by intravascular ultrasound in the different three remodelling groups. (A) shrinkage; (B) non-remodelling; (C) compensatory enlargement group. In group A, 67% of the luminal area decrease was contributed by plaque. The remaining 33% luminal area decrease was attributed to paradoxical shrinkage of the lesion. In group B with no remodelling, the stenosis was formed alone by plaque. In group C, plaque contribution was 187% caused by compensatory enlargement of 87% in lumen area.
Increase of percentage luminal area stenosis with intravascular ultrasound showed a trend (p = 0.051) towards shrinkage or lack of compensatory enlargement in the population studied (table 1).
Discussion
In this intravascular ultrasound study, we report that coronary arteries show opposite types of arterial wall remodelling in response to atherosclerotic plaque formation. Apart from eight of 21 (38%) coronary artery lesions with compensatory enlargement, we also observed eight (38%) lesions with arterial wall shrinkage. In group A, 33% of luminal area narrowing had to be attributed to vessel wall shrinkage.
Our results are in concordance with previous studies we performed in the femoral artery.3 An in vivo ultrasound study by Nishioka et al 11 reported similar results with regard to different types of arterial wall remodelling (54% compensatory enlargement, 26% shrinkage, and 20% no remodelling) in 35 primary atherosclerotic coronary lesions. They reported a similar 39% lumen stenosis by shrinkage in the group with arterial wall shrinkage.
Furthermore, we noticed a significant trend in the type of arterial wall remodelling and severity of luminal narrowing. Shrinkage dominated in lesions with severe luminal area stenosis, whereas compensatory enlargement dominated in lesions with less than 65% luminal area stenosis. As shown by Pasterkamp et al,3 in femoral arteries compensatory enlargement of the arterial wall dominated in lesions with less than 25% luminal area stenosis. In this study, only lesions with more than 50% luminal area stenosis were studied and compensatory enlargement was dominated in lesions with less than 65% lumen stenosis. No relation was found between the type of arterial remodelling and clinical parameters. The occurrence of unstable lesions and post infarct lesions were equally distributed among the remodelling groups.
The mechanism responsible for arterial wall remodelling is unknown. Remodelling is a focal phenomenon, which in one artery can go either way.3 Because this is not a serial intravascular ultrasound study, we did not have information about the natural history of the different lesions. Hence, it is unknown whether shrunken lesions were shrunk from the very start of the local disease or whether in time, enlarged lesions may transform into shrunken lesions and vice versa. Several mechanisms for compensatory enlargement, which seems to be a teleologically understandable response, have been proposed.12 The prevailing theory is when initial plaque growth tends to narrow the lumen, local shear stress increases and the endothelium reacts by increasing nitric oxide production with chronic vasodilatation as a consequence.13 This hypothesis seems only valid for eccentric lesions, as expansion may only be achieved by the non-diseased part of the arterial wall. Thus, adequate expansion of the atherosclerotic arterial wall may be impaired or impossible in concentric lesions. The mechanism of paradoxical shrinkage is even less understood. Perhaps the presence of circumferential dysfunctional endothelium or basal release of a local vasoconstrictor agent may attribute to arterial wall shrinkage.14 ,15
Arterial wall remodelling and in particular shrinkage sheds new light on the process of luminal narrowing by atherosclerosis and may have therapeutic consequences. Hence, it is conceivable that the initial stenosis that is influenced by different remodelling mechanisms, may respond differently to angioplasty and may be more or less prone to restenosis. In restenosis, shrinkage may be the most important mechanism instead of intima hyperplasia.16 ,17
STUDY LIMITATIONS
The comparatively large number of right coronary artery lesions studied (14 of 21) may have influenced the presence and rate of arterial wall remodelling. In a histopathological study of human coronary arteries some differences in grade of arterial wall remodelling among the arteries occur.18 Furthermore, the reference site contained a certain amount of plaque (table 2). This may have provoked some arterial wall remodelling at the reference site that could have influenced the calculated degree of relative change in EEL area at the lesion site.
Crossing of the stenotic lesion with the ultrasound catheter could have caused a further drop in post stenotic pressure and therefore could have influenced the distal reference cross sectional area measurements. Furthermore, when side branches were present proximal or distal from the lesion only one reference cross section was taken. Subsequently tapering of the vessel segment was not taken into account. However, when we corrected for the degree of tapering as observed by Javieret al 19—that is, a 10% loss of vessel size (EEL area) over 10 mm of arterial length from the proximal reference point—then still eight of the 21 (38%) analysed lesions would be categorised as being “shrunken”.
In conclusion, paradoxical arterial shrinkage occurs in the human coronary artery and seems to be an important determinant of severe lumen narrowing.