Article Text

Abstract
The outcome of acute myocarditis with cardiogenic shock is poor. In some children in whom aggressive medical treatment fails, artificial replacement of heart function may offer lifesaving support until the myocardium has recovered. Four previously healthy children (three boys aged 4, 6, and 1 years; one girl aged 5) developed acute myocarditis with ventricular failure and multiorgan dysfunction caused by low cardiac output. Biventricular assist devices (BVAD) were implanted for prolonged support. In three children cardiac function improved and after up to 21 days mechanical support could be withdrawn. They had full recovery of heart function. In the fourth patient there was no myocardial recovery after a period of 20 days. He underwent orthotopic heart transplantation with an uneventful postoperative course. Prolonged circulatory support with BVAD is an effective method for bridging until cardiac recovery or transplantation in children.
- fulminant myocarditis
- cardiogenic shock
- biventricular assist device
- paediatric cardiology
Statistics from Altmetric.com
Acute myocarditis and cardiogenic shock predict poor survival. However, complete recovery in most children occurs if cardiopulmonary circulation can be maintained during the acute phase. Death occurs because of acute cardiac decompensation from inflammation, necrosis, or myocytolysis in the early phase, and might be prevented by a circulatory support system in the acute phase.1 We report four children surviving acute fulminant myocarditis and prolonged circulatory support with biventricular assist devices (BVAD).
Patients and methods
Between 1995 and 1998 four children with progressive cardiac failure due to severe myocarditis were treated with BVAD for long term circulatory support. Treatment was approved by institutional review board and written informed consent was given by the parents.
The BVAD “Berlin Heart” consists of two extracorporeal pneumatically driven blood pumps made out of polyurethane (right 25 ml, left 30 ml stroke volume), within a multilayer flexible polyurethane membrane separating this pump chamber into a blood and an air chamber (fig 1). Three leaflet polyurethane valves prevent blood reflux. Four silicon cannulae connect the blood pumps with the right atrium and pulmonary artery, and the left atrium (or left ventricle transmitral) and ascending aorta. A Dacron cover in the middle part of the cannulae allows rapid ingrowth of patients’ tissue as a biological barrier against infections (fig 2). The pumps are driven by a pulsatile electropneumatic system, all blood contacting surfaces are heparin coated.
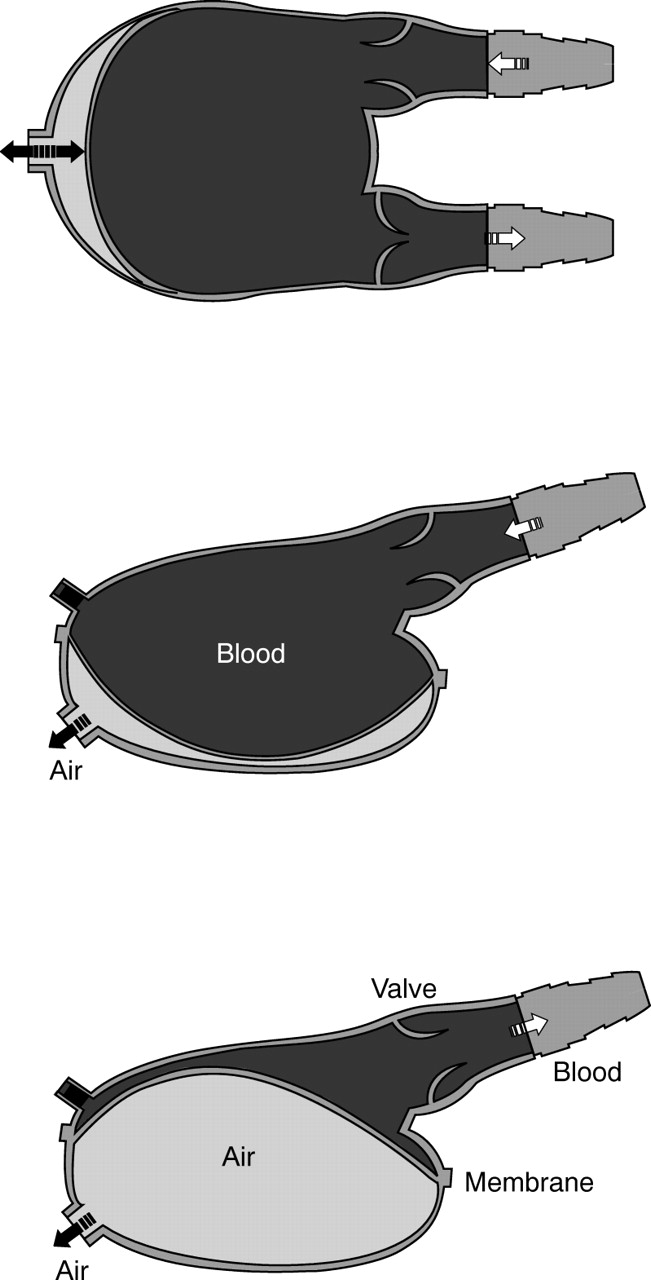
BVAD: top view and side view of the housing in diastolic and systolic position.

Paediatric assist systems. Two pumps for newborns (10 ml stroke volume) with different cannulae. One pump for infants (30 ml ) with Dacron covered middle part of the cannulae.
Indications for placing patients on BVAD were cardiogenic shock despite aggressive medical treatment and artificial respiration, profound multiorgan failure, and repeated resuscitation. In the first two patients weaning was achieved by changing BVAD for extracorporeal membrane oxygenation (ECMO) with an oxygenator (Carmeda Maxima; Medtronic, Düsseldorf, Germany), centrifugal pump (Biomedicus; Medtronic), reservoir (Duraflow 2; Baxter, Unterschleißheim, Germany), and heparin coated tubes. One patient was transplanted from BVAD without any attempt to wean, and in the last patient direct weaning from BVAD was successful.
Protein S-100 was measured with a specific monoclonal antibody (Sangtec, 100 IRMA; AB SangtecMedical, Bromma, Sweden).
All children had previously been in good health until the acute onset of fever, followed by a fulminating course (table1).
Patient characteristics
CASE REPORTS
Patient 1—A 4 year old boy (weight 16.5 kg) returned from a two year stay in India two weeks before onset of symptoms. Fever, eosinophilia, infection of the upper respiratory tract, and pneumonia were followed by global myocardial failure. Patient 2—A 5 year old girl (weight 23 kg) developed peripheral oedema, myalgias, vomiting, and pulmonary oedema three days after the onset of fever, 200 ml pericardial effusion were drained by pericardiocentesis. Serum IgM was positive for coxsackie B virus (fig 3). Patient 3—A 6 year old boy (weight 19 kg) had pertussis-like disease followed by vomiting, fever and cardiogenic shock three weeks after onset of first symptoms. Patient 4—A 15 month old boy (weight 10 kg) developed fever and an infection of the upper respiratory tract one week after vaccination (mumps, morbilli, rubella). Two days later hospitalisation because of generalised oedema, followed by resuscitation in cardiogenic shock 24 hours later (fig4).

Patient 2 with BVAD (photograph published with permission of the child’s parents).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Course of patient 4 before, during, and after BVAD. Platelets and protein S-100, a specific glia brain cell protein as a biochemical marker are shown.
BEFORE BVAD
All patients had been treated in other paediatric intensive care units and transferred to our centre for further diagnosis and suggestion of emergency mechanical circulatory support. All children had biopsy proved acute myocarditis with extensive myocytolysis, inflammation, necrosis of more than 50% of the myocytes, interstitial oedema with eosinophils, and a distinct vasculitis. Possible causes of cardiomyopathy (carnitine deficiency, storage disease, mitochondrial defects, bacterial and fungal infection) had been considered and found negative in specific laboratory tests. Aggressive management consisting of inotropic support with catecholamines, afterload reduction, phosphodiesterase inhibitors, diuretic treatment, and sodium bicarbonate supplementation resulted in insufficient circulatory responses in all four children. Multiorgan dysfunction caused by low cardiac output required Fio 2 1.0 on mechanical ventilation and peritoneal dialysis for renal failure. Chest radiography demonstrated enormously enlarged hearts and the ECGs showed reduced QRS complex voltages, tachycardia, and ventricular arrhythmia. Poor ventricular function, high grade tricuspid and mitral valve regurgitation, and a left ventricular ejection fraction below 12% was seen on echocardiography. Each child had cardiac arrest before assisted circulation was started. Patient 1 was brought to the operating theatre under continuous cardiac massage.
DURING BVAD
Stabilisation of circulation and renal function was achieved a few hours after implantation of BVAD. Inotropic support was stopped and the ensuing mild hypertension was regulated with vasodilators if necessary. In all children there was total skin and partial sternum closure allowing mobilisation. Heparin was infused continuously to achieve an activated clotting time of 140–160 seconds. No episodes of thrombosis or embolisation were observed. Antibiotic treatment with good antistaphylococcal cover was given during the whole period. No sign of severe infection was detected.
COMPLICATIONS
Two patients developed necrotising pancreatitis (maximum lipase 2800 U/l) after resuscitation, which reversed during the time on BVAD. Mediastinal re-exploration was required in two children because of intrapericardial bleeding. In patient 2 diffuse intraperitoneal bleeding was observed, which worsened (up to 3.8 litres/day and was retransfused using a cell saving device) during the weaning period on ECMO, probably due to heparin treatment. This haemorrhage ceased after decannulation and protamine infusion.
Results
Patients 1 and 2 could be weaned from mechanical support. Continuous improvement of systolic myocardial function began after five days on BVAD. The BVAD was changed to ECMO for easier gradual weaning on day 21 (patient 1) and day 11 (patient 2).
During weaning, ventricular function was measured daily by transoesophageal echocardiography in relation to systolic blood pressure, and filling volumes and pressures as pump flow was decreased. After successful decannulation cardiac index measured by thermodilution was between 2.7 and 3.4 l/min/m2 during the following days.
In patient 3 there was recovery of all organs except for the heart. The generalised oedema was eliminated quickly, he was extubated two days after implantation of the BVAD. The patient regained full consciousness and was mobilised, eating and drinking by himself, and playing with his parents. After the first week he was allowed to leave the bed once a day, stand up and walk around his bed, but he remained on the intensive care unit. When no myocardial recovery was detected by echocardiography during 20 days on BVAD, he underwent orthotopic heart transplantation with an uneventful postoperative course.
Weaning of patient 4 was done without ECMO directly from BVAD after 11 days of circulatory support. We reduced pump volume and frequency for one week while we measured blood pressure and cerebral blood flow by pulsed Doppler sonography in the arteria cerebri media. We found a slight increase of protein S-100 (fig 4).
OUTCOME
All children survived and had full recovery of heart (or transplant) function and no neurological sequel. Follow up examination after 28, 17, 12, and 4 months in patients 1, 2, 3, and 4, respectively, showed all patients remaining well, integrated in their normal life with normal heart function.
Discussion
When aggressive standard treatment fails in children with fulminant myocarditis, prolonged circulatory support is necessary for potential survival to allow recovery of the heart or to provide support until transplantation.1-4
We report our experience with BVAD in four children with acute myocarditis. In these children with an anticipated mortality of 100%, long term circulatory support was successful in all cases. After up to 21 days on circulatory assistance, three children recovered heart function. These three long term survivors with good cardiac function confirm the hypothesis that many children with myocardial dysfunction due to acute myocarditis have reversible cardiac failure and can recover if the circulation is supported during the critical weeks of inflammation and healing.3 ,5
Indications and criteria for placing children on BVAD are very strict. Only after failure of aggressive medical management and repeated resuscitation do we use this circulatory assistance for rescue. Our results, with full recovery of three patients’ hearts, show that the gain of time and unloading the heart with BVAD might induce this functional improvement.6 Müller et al described the benefit of ventricular unloading by different assist devices, and cardiac recovery of five adults with idiopathic dilated cardiomyopathy.7 Long term follow up of our paediatric patients is necessary to rule out dilated cardiomyopathy, which has been seen in survivors of severe myocarditis without unloading by artificial pumps.8-10 The acute fulminant myocarditis occasionally resolves without residual ventricular dysfunction.11 However, in some patients a previous myocarditis probably results in a so called idiopathic dilated cardiomyopathy.8 Whether immunosuppressive treatment alters the natural history of myocarditis is unknown.12 ,13
Brain protection and early identification of cerebral injury is important because our infants were resuscitated before BVAD implantation. During mechanical support there is the danger of thrombosis in the left sided assist system with low anticoagulation and cerebral bleeding with very high anticoagulation. As a biochemical marker for cerebral events we measured protein S-100, a specific glia cell protein (fig 4). In adults, S-100 is only released into serum following cerebral damage. In newborns and small infants the permeability of the blood–spinal fluid barrier causes a slight increase over the normal ranges.14 In patient 4 we saw only a small increase of S-100, comparable to the age related ranges found after cardiac surgery with cardiopulmonary bypass.14This child had no cerebral event and was discharged without any neurological sequel.
The use of ECMO after cardiac surgery has been shown to be lifesaving in children with myocardial failure.15-18 When pulmonary function is normal, ECMO is not always the optimal method for prolonged circulatory support because of complexity of equipment, bleeding complications, capillary leak syndrome, and non-pulsatile flow. One of the three children treated by Del Nido et alrecovered spontaneously and was decannulated on the seventh day of ECMO, one died on ECMO on day 12, and another was transplanted on the fifth day.17 In two of our children with BVAD the first echocardiographical signs of myocardial improvement were seen on day 5 and the chance for recovery would have been missed with early transplantation. The advantages of ECMO in contrast to BVAD are easier cannulation, oxygenator support in pulmonary insufficiency, and the possibility of slow reduction of circulatory support.19The most common complication of ECMO is bleeding related to heparinisation. BVAD limits haemorrhagic complications as less anticoagulation with heparin is required. With ECMO the activated clotting time is usually maintained between 170 and 200 seconds19 compared to 140–160 seconds in our children on BVAD. Thrombocytopenia is another reason for bleeding on ECMO.18 In our children on BVAD there was no severe thrombocytopenia, thrombocytes regaining normal ranges. No platelet transfusion was given.
Once the normal functional pattern of the initially akinetic ventricles was observed, we changed to ECMO for a short period for easier gradual weaning after a period up to 21days on BVAD. That was necessary in the first 2 patients because the cannulae reached into the ascending aorta and pulmonary artery, resulting in increased resistance. Over a 5–6 day period the ECMO flow was reduced in a stepwise fashion. Following initial experience, our cannulae for small children have undergone several modifications. In patient 4 we used special end-to-side cannulae without obstruction of the vessels and developed controlled weaning from BVAD over a period of one week.
The advantages of BVAD are a much longer gain in time to restore organ function, elimination of oedema, extubation, mobilisation, improvement in nutrition, and the chance of letting the children regain consciousness to assess neurological status. Reduced capillary leak in BVAD may be due to the pulsatile flow and to less contact with synthetic surfaces.
Prolonged circulatory support with BVAD in children suffering from acute myocarditis with cardiac shock unresponsive to medical treatment is an effective method for bridging until cardiac recovery.20 If there is no improvement in myocardial function on BVAD, there is an increased chance for transplantation as we have observed in children with various life threatening diseases.5 ,18
Acknowledgments
We are grateful to the staff of the intensive care unit for their continuing encouragement. Supported by Deutsche Forschungsgemeinschaft grant No.He 1669–2/1.