Article Text

Abstract
OBJECTIVE To review 12 years of experience of balloon aortic valvoplasty in childhood.
DESIGN Early and mid-term clinical and instrumental evaluation of 104 consecutive balloon aortic valvoplasties performed from 1986 to 1998.
SETTING A tertiary referral centre for congenital heart disease.
PATIENTS 90 patients with congenital aortic stenosis: 20 neonates (group 1), 16 infants (group 2), and 54 children (group 3).
INTERVENTIONS Balloon aortic valvotomy.
MAIN OUTCOME MEASURES Doppler and peak to peak aortic gradient before and after valvoplasty, degree of aortic regurgitation before and after valvoplasty, early and late mortality, need for repeat intervention or surgery.
RESULTS Balloon aortic valvoplasty produced a gradient reduction of > 50% in 59 patients, 12 having a residual peak to peak gradient of > 50 mm Hg. Early mortality included three procedure related and six procedure unrelated deaths. There were no intraprocedural deaths. Grade III aortic regurgitation occurred in 20 patients. Five non-lethal complications occurred. At a mean follow up of 5.1 (group 1), 5.7 (group 2), and 7.6 years (group 3), survival was 75%, 88%, and 96%, respectively. Redilatation was performed in three patients in group 1, one in group 2, and 10 in group 3. Surgery was necessary for six in group 1, one in group 2, and eight in group 3. Freedom from events at last follow up was 50%, 75%, and 64%, respectively. There was a residual maximum Doppler gradient of < 30 mm Hg in 22 patients and > 60 mm Hg in 23; 50 patients have mild to moderate aortic regurgitation.
CONCLUSIONS Balloon aortic valvoplasty is effective and repeatable and offers good palliation for congenital aortic stenosis in childhood.
- aortic valve disease
- paediatric cardiology
- percutaneous valvotomy
- interventional catheterisation
Statistics from Altmetric.com
Balloon aortic valvoplasty is now considered a safe and effective technique which achieves satisfactory palliation for several years.1The predictors of persisting success remain unknown, though the principal determinants of early outcome have recently been examined.2 Few reports on long term results have been published, as this technique was performed for the first time in 19843 but was not in general use until some years later.
We report the mid-term results of 104 sequential aortic balloon dilatations performed at our institution since 1986 in 90 patients. The population was divided into three groups according to age, on account of the special features of aortic stenosis in the newborn4and the well known increased risk of the procedure in babies less than one year of age.2 ,5 In each group of patients, we separately evaluated early and late survival, need of reintervention, early and late development of aortic regurgitation, and late residual gradient.
Methods
The data reported summarise our 12 years of experience, during which the indications for balloon aortic valvoplasty, the technical approach, and our expertise were subject to several changes.
POPULATION
All patients with congenital aortic stenosis undergoing balloon aortic valvoplasty at our institution between 1 January 1986 and 1 July 1998 were enrolled in the study. No patient was excluded because of associated defects, but patients who had had a previous balloon aortic valvoplasty at other institutions were not included in the study. The population included 60 boys and 30 girls: 20 neonates (0–30 days) (group 1), 16 babies (1–12 months) (group 2), and 54 children and adolescents (> 1 year) (group 3).
CRITERIA FOR DILATATION
In group 1 balloon aortic valvoplasty was performed when critical aortic stenosis was present, defined by clinical (presence of low cardiac output, cardiogenic shock, congestive heart failure) and echocardiographic criteria (morphological evidence of left ventricular hypertrophy, with depression of left ventricular function, irrespective of the transvalvar gradient). A maximum aortic gradient of more than 70 mm Hg with preserved left ventricular function was also an independent indication for balloon valvoplasty.
Before 1993 balloon valvoplasty was indicated in all cases of severe aortic stenosis, except in those with obvious hypoplastic left heart syndrome. After 1993 the echocardiographic exclusion criteria suggested by Rhodes et al were followed.4
In groups 2 and 3, balloon dilatation was performed when two or more of the following conditions were present: maximum Doppler gradient equal to or higher than 80 mm Hg, a peak to peak systolic aortic gradient higher than 50 mm Hg, left ventricular hypertrophy on ECG or echo, and presence of symptoms. Balloon dilatation was not performed when aortic regurgitation of more than mild degree was present.
VASCULAR APPROACH
Up to 1989, most neonates with congenital aortic stenosis in our institution underwent cardiac surgery, though some had ineffectual attempts at balloon valvoplasty through the femoral artery. Subsequently, carotid cutdown was introduced for patients weighing 6 kg or less, while right axillary cutdown was preferred in patients weighing from 7 to 10 kg.5 ,6 In all other cases the femoral approach was employed.
METHODS
Medical records of each patient were reviewed, including hospital notes, bidimensional and Doppler echocardiographic reports, and catheterisation reports. We evaluated Doppler aortic valve gradient and the degree of aortic regurgitation on colour Doppler imaging, peak to peak systolic aortic gradient, and the degree of aortic regurgitation at angiography before and after balloon dilatation.
The aortic annulus was measured by bidimensional echocardiography and cineangiography, using the catheter size to correct for magnification. Initial balloon size was 80–100% of the angiographically measured aortic annulus.
If inadequate relief of the gradient was obtained (less than 50% reduction) in the presence of good systolic function and in the absence of more than mild aortic regurgitation, serial dilatation with a larger size of balloon was performed, to a maximum of 125%.
Aortic regurgitation was graded either echocardiographically or angiographically according to Moore et al,1 using a scale of 0 to 4: 0, absent; 1, trivial; 2, mild; 3, moderate; 4, severe.
DEFINITION OF SUCCESSFUL BALLOON AORTIC VALVOPLASTY
With preserved left ventricular function, success was defined as a gradient reduction of 50% or more, or a maximum residual gradient of 50 mm Hg or less.
With impaired left ventricular function, it was defined as immediate improvement of left ventricular function, irrespective of the gradient, employing an adequate balloon to annulus ratio.
FOLLOW UP
Follow up information, obtained directly from the patient at an annual visit, included state of health, need for drug treatment, need for repeat intervention, maximum Doppler gradient, and degree of aortic regurgitation. Reintervention included repeat balloon dilatation, surgical valvotomy, surgical valvoplasty, and valve replacement (homograft or prosthetic). Surgery for associated anomalies was also considered. When performed, follow up catheterisation data, including peak aortic gradient and degree of aortic regurgitation, were reviewed.
STATISTICAL ANALYSIS
Data are given as mean (SD). Age and weight are expressed as median values. Comparisons between groups were made using unpairedt test and analysis of variance, with Bonferroni correction for interval data. Comparisons in single groups were made using the McNemar test. For analysis of survival and freedom from events, the Kaplan–Meier test followed by a log rank test was performed.
Results
PATIENT CHARACTERISTICS
The characteristics of the patients are given in table 1. Weight was appropriate for age in all groups. One patient in group 1 was born at 35 weeks gestation, weighing 2.3 kg. Seven neonates were in a critical clinical condition because of low cardiac output, congestive heart failure, metabolical acidosis, or shock; nine were receiving prostaglandin E1; an emergency procedure was performed in five. In four, prenatal diagnosis allowed planned delivery and programmed intervention. In group 2, five patients were in a critical condition, while the remaining patients had elective procedures. All patients in group 3 had elective procedures.
Clinical characteristics, associated malformation, and interventions before balloon aortic valvoplasty (BAV) in the three groups of patients
IMMEDIATE RESULTS
Balloon aortic valvoplasty was completed in all cases and was successful in 16 of 20 in group 1, 16 of 16 in group 2, and 49 of 54 in group 3. Mean balloon to aortic annulus ratio was 0.98 in group 1, 0.97 in group 2, and 0.97 in group 3. Eleven patients in group 1, seven in group 2, and 10 in group 3 had sequential balloon dilatation during the same procedure.
Complications
Five serious complications occurred (5.5%): one perforation of the left ventricle and cardiac tamponade (group 1), one transient right stellate ganglion damage (group 1), one ventricular fibrillation (group 1), one asymptomatic occlusion of the right carotid artery (group 1), and one asymptomatic occlusion of the right femoral artery (group 3).
Mortality
No death occurred during the procedure; however, one patient in group 2 and two patients in group 3 had damage to the right internal iliac artery and died during or after surgical repair (3.3% procedural mortality rate). All cases occurred at the start of our experience.
Early mortality occurred in five of 20 from group 1 (p < 0.05), two of 16 from group 2, and two of 54 from group 3 (10% global early mortality). In group 1, three early deaths from low cardiac output occurred at 28 h, 48 h, and 35 d after balloon dilatation (in two of these redilatation was repeated at 2 and 30 days). Two more infants died 5 and 30 days after balloon dilatation, after surgery for aortic coarctation and surgical valvotomy. In group 2, one patient died from low cardiac output one month after balloon dilatation; a second died from laceration of the iliac artery. In group 3, two early deaths were caused by laceration of the iliac artery. In group 2 and 3 no early deaths occurred after 1988.
Gradient reduction
Peak systolic aortic gradient fell from 67.1 (26.8) to 26.3 (17.7) mm Hg in group 1 (p < 0.001), from 74.3 (25.1) to 29.7 (12.8) mm Hg in group 2 (p < 0.001), and from 82.3 (26.4) to 36.6 (19.2) mm Hg in group 3 (p < 0.001). Fifty nine patients had a reduction of more than 50% and 12 had a residual gradient greater than 50 mm Hg. Postprocedural echocardiography showed a reduction in maximum Doppler gradient from 67.5 (25.7) to 33.6 (14.03) mm Hg in group 1 (p < 0.001), from 81.2 (15.7) to 29.7 (12.9) mm Hg, in group 2 (p < 0.001), and from 84.6 (21.9) to 49.0 (18.2) mm Hg, in group 3 (p < 0.001). Peak to peak gradient and Doppler gradient were correlated (y = 0.57x + 31.8, r = 0.49, p < 0.001).
Aortic regurgitaton
Aortic regurgitaton occurred in 56 patients (53%), 15 from group 1, eight from group 2, and 33 from group 3 (p > 0.05) (fig 1). No patient in group 1 or 2, and 14 in group 3 (12 of whom had had a previous surgical valvotomy) had aortic regurgitation before balloon aortic valvoplasty; the procedure resulted in an increased grade of regurgitation in six of these. No correlation was found between the grade of aortic regurgitation and the ratio of balloon diameter to aortic annulus.
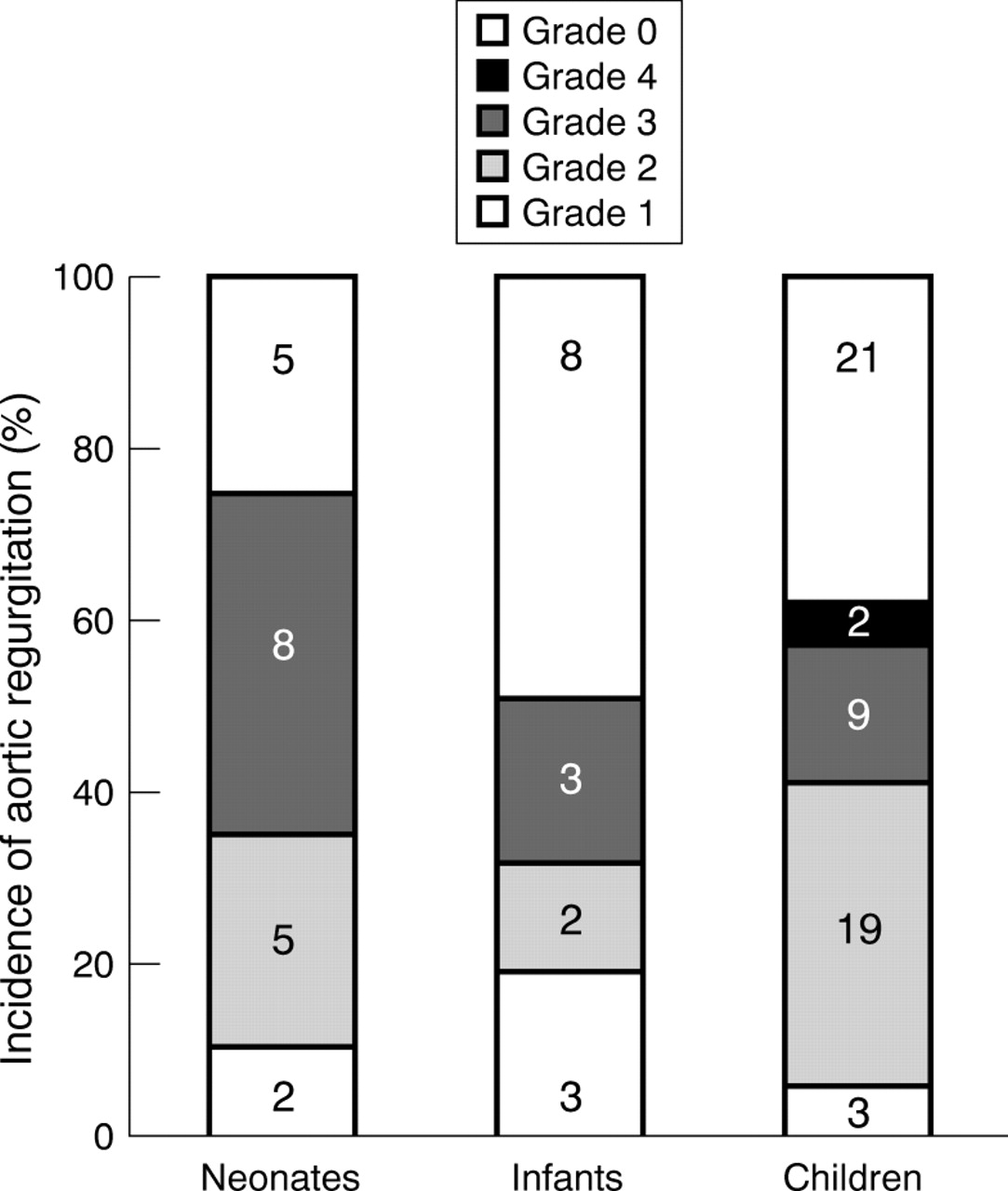
Incidence of aortic regurgitation immediately after balloon dilatation. The numbers of patients are given in the columns.
MID-TERM RESULTS
Length of follow up was 5.1 (2.4) years (range 1 to 9) in group 1, 5.7 (2.8) (1 to 10) in group 2, and 7.6 (3.2) (1 to 12) in group 3.
Follow up recatheterisation
Elective follow up catheterisation was performed in 13 patients at the start of our experience (between 1986 and 1989) at 9–12 months after the balloon dilatation. In this group, peak to peak gradient increased from 28.5 (15.3) to 36.2 (14.8) mm Hg (p > 0.05); in only one patient was the degree of aortic regurgitation increased. Three more patients underwent recatheterisation after 1989, immediately before aortic valve replacement.
Redilatation
Aortic balloon redilatation was performed in three of 20 patients (15%) from group 1, one of 16 (6%) from group 2, and 10 of 54 (18%) from group 3. In group 1 it was performed at 2, 30, and 35 days after the first balloon dilatation, because of restenosis (1) and persistent congestive heart failure because of an inadequate left ventricle (2). In the first patient it was successful, while the two babies with persistent congestive heart failure died shortly afterwards. In group 2, redilatation was successfully performed in one patient with restenosis 22 months after the first balloon dilatation. In group 3, 10 patients underwent repeated balloon aortic valvoplasty after 4.1 (2.0) years; this was successful in nine and unsuccessful in one patient, who had previously had a surgical valvotomy and underwent aortic valve replacement.
Cardiac surgery
Surgery was performed in six of 20 patients in group 1 (30%) (p > 0.05), one of 16 in group 2 (6%), and eight of 54 in group 3 (15%). In group 1 surgery consisted of resection of subaortic membrane (two patients, three years after balloon dilatation), repair of aortic coarctation (one patient, died after surgery a few days after balloon dilatation), surgical valvotomy (two patients, 30 days and three years after balloon dilatation, the first of whom died), and a Ross procedure (one patient, one year after balloon dilatation). A single patient in group 2 had successful surgical valvotomy six months after balloon dilatation. Surgery in group 3 consisted of aortic valve replacement (seven prosthetic (one death) and one Ross procedure), at 3.2 (2.8) years (range 1 to 7) after balloon dilatation and at a mean age of 14 years. The indication for aortic valve replacement was severe aortic regurgitation in six patients and concomitant aortic stenosis and regurgitation in two. One patient died after prosthetic replacement of the aortic valve.
Freedom from events and survival
The overall freedom from events at last follow up was better in groups 1 and 3 than in group 2, but the difference was not statistically significant (p = 0.07): 50% in group 1, 65% in group 2, 45% in group 3 (fig 2). Global late survival was significantly worse in group 1 (p < 0.05): 75% in group 1 (five early deaths, no late deaths), 86% in group 2 (two early, no late), and 95% in group 3 (two early, one late) (fig 3). The most recent event occurred at five, two, and seven years after balloon dilatation in groups 1, 2, and 3, respectively. The most recent death occurred at 150, 60, and 423 days, respectively, in the three groups. There were no cases of sudden death.
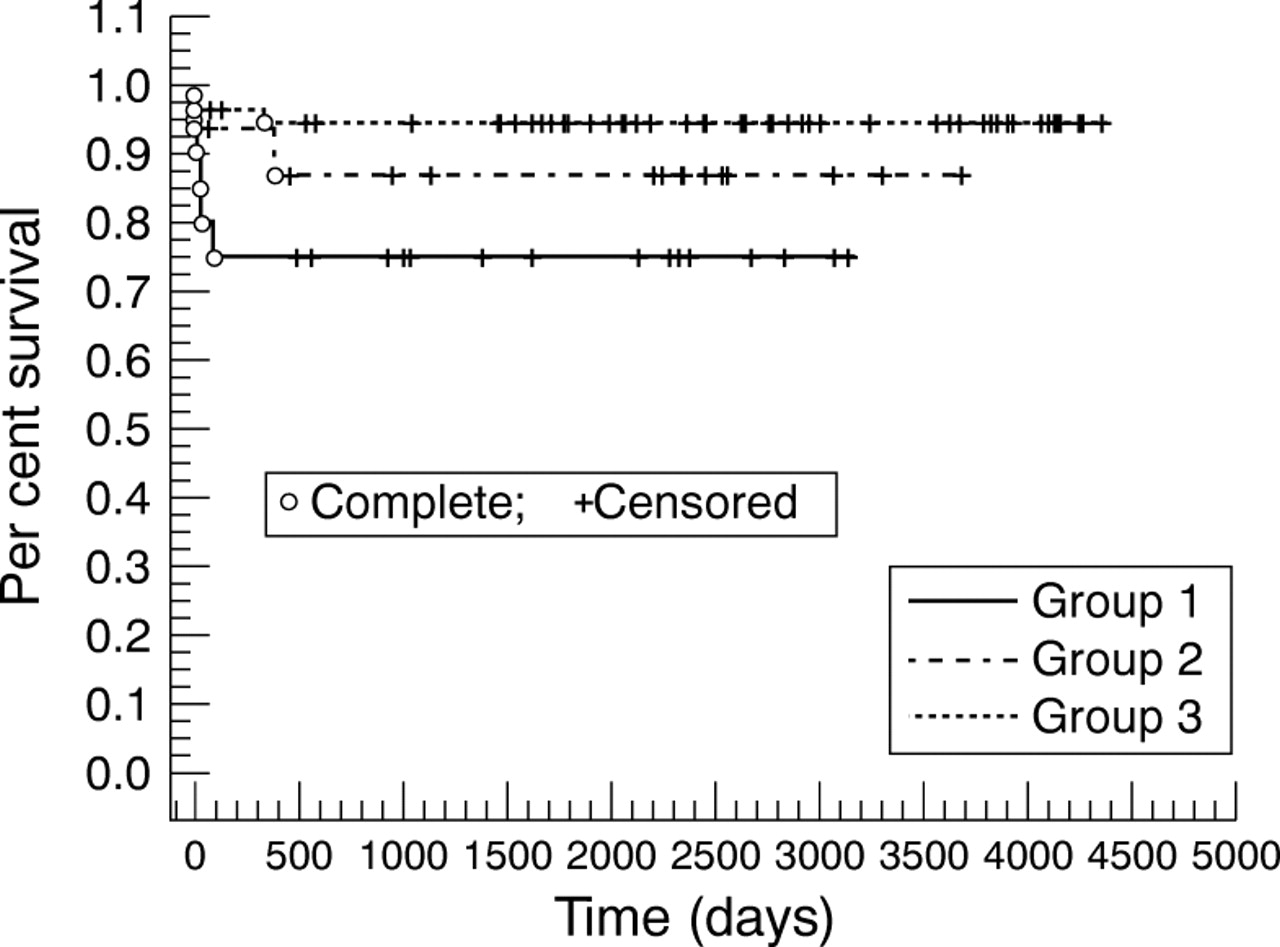
Survival curve in the three groups of patients.
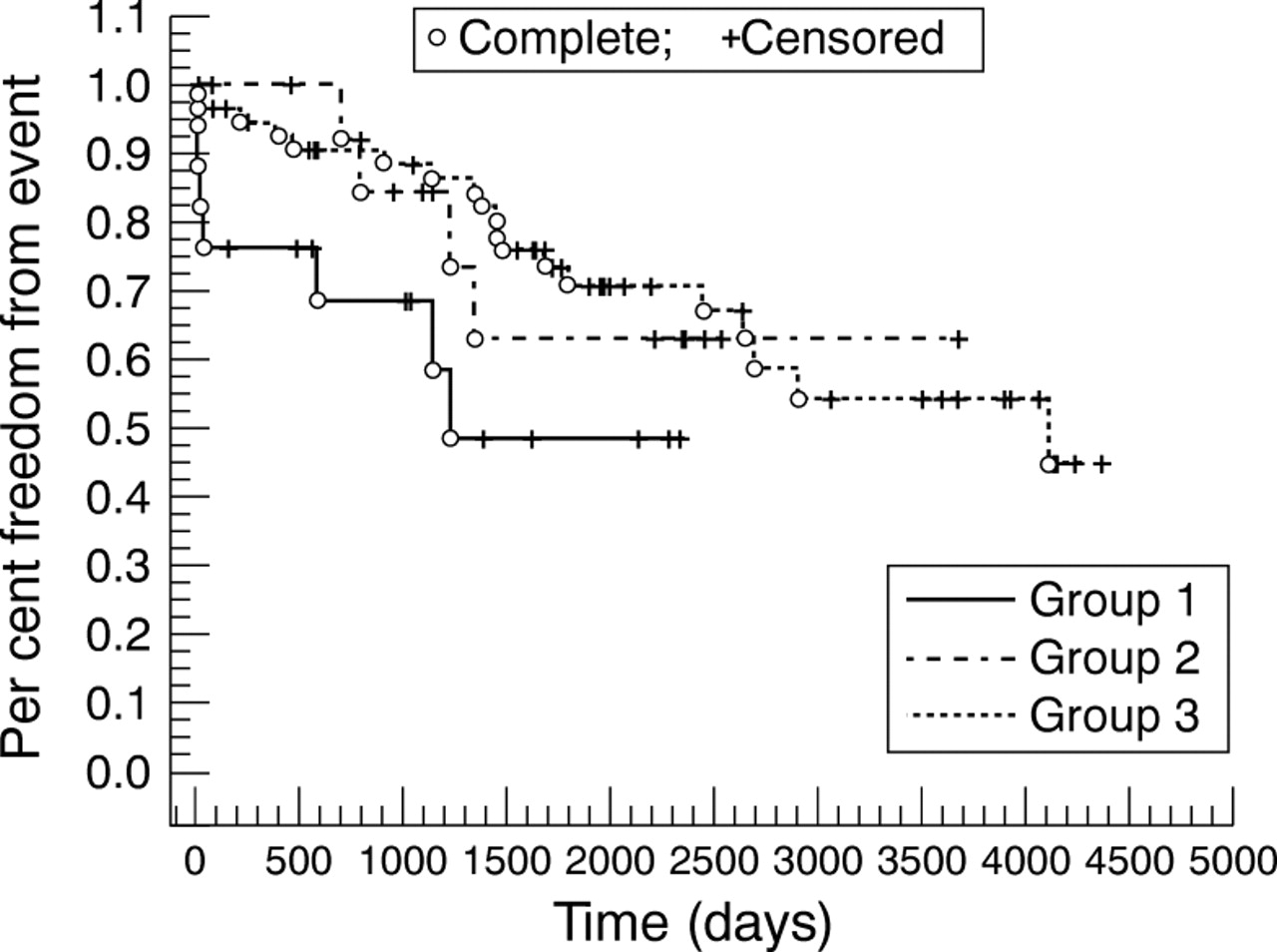
Freedom from events in the three groups of patients.
Echocardiographic assessment
The maximum Doppler gradient did not change significantly in any group. It varied from 33.6 (14.03) to 45.5 (22.6) mm Hg in group 1 (p = 0.053), being increased in six patients and unchanged in nine; three patients had a maximum Doppler gradient of less than 30 mm Hg and in four it was more than 60 mm Hg. In group 2, maximum Doppler gradient varied from 29.7 (12.9) to 39.2 (18.6) mm Hg (NS), being increased in only two patients; five had a gradient of less than 30 mm Hg and in two it was more than 60 mm Hg. In group 3, maximum Doppler gradient varied from 49.03 (18.2) to 48.3 (23.8) mm Hg (NS), being increased in seven patients; 14 patients had a gradient less than 30 mm Hg and in 17 it was more than 60 mm Hg.
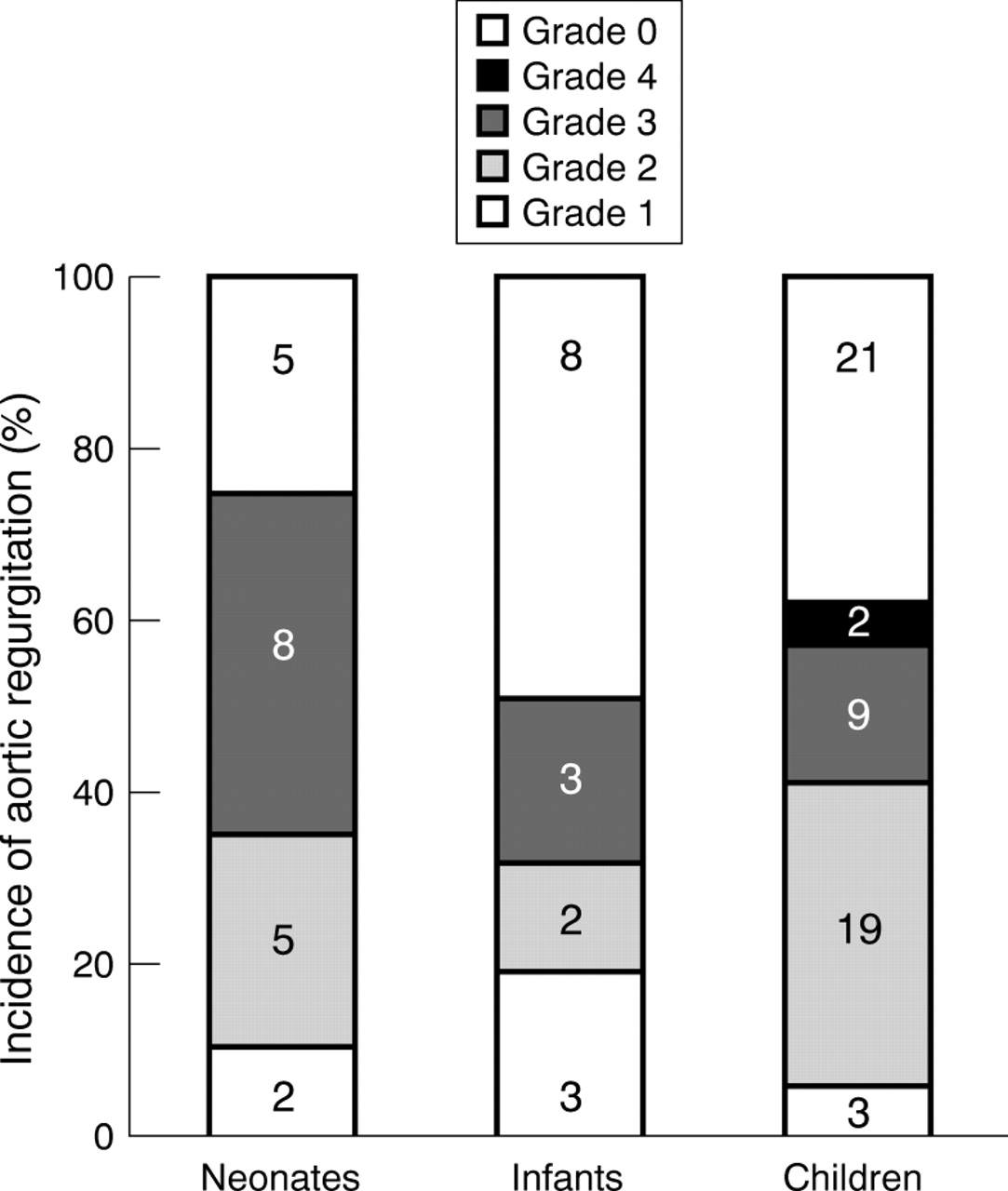
Aortic regurgitation occurred in 57 patients (70%): 15 in group 1 (100%) (p < 0.01), 10 in group 2 (71%), and 32 in group 3 (61%). In all but two patients it was mild to moderate (fig 4); however, eight patients had aortic replacement because of severe aortic regurgitation, accounting for an 11% global incidence of grade IV aortic regurgitation. The incidence of aortic regurgitation did not increase significantly during the observation period.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Incidence of aortic regurgitation at late follow up. Numbers of patients are given in the columns.
Discussion
STUDY LIMITATIONS
Our study has limitations related to the heterogeneity of the population examined, and to changes in equipment, technique, and indications for balloon aortic valvoplasty that occurred during the period of time examined.
Unlike other investigators,7 we divided our patients into three groups according to age. Patients in groups 1 and 2 are considered to be a separate group, with particular risks, clinical presentation, and outcome.2 ,4 ,8-10 These groups were included in our study in order to review the mid-term result of balloon aortic valvoplasty in children of various ages.
IMMEDIATE RESULTS
Most investigators refer to balloon aortic valvoplasty as a safe and effective procedure.1 ,7 ,11 ,12 In our series, global perioperative death was entirely related to vascular complications and was zero after 1989, when the carotid and axillary approach was introduced. A similar incidence of damage to the iliac or femoral artery was reported by Sullivan et al.13 No perioperative deaths occurred in group 1, which included seven neonates in a critical condition. This is noteworthy, as balloon aortic valvoplasty is known to incur a higher risk in this group.2 ,8 ,9 ,14 None of the serious complications observed was likely to be associated with late sequelae.
Overall early mortality was probably related to age, being significantly higher in group 1. When periprocedural deaths were excluded, early mortality was zero in groups 2 and 3, while it was unchanged in group 1, in accordance with data reported by other investigators.8 ,9 The higher incidence of death in neonates or babies with poorly tolerated critical aortic stenosis is well documented,4 ,9 ,15 and reached 50% in our patients with depressed left ventricular function. In group 1, early mortality was related to surgery in 40% of cases. It has been noted that aortic coarctation is an independent risk factor for balloon aortic valvoplasty in this group.2
The occurrence of aortic incompetence after balloon aortic valvoplasty is a well known and serious complication. It has been reported that aortic incompetence is more likely to occur in patients who have had previous surgical valvotomy.16 These data were not confirmed in our study or by Sreeram et al.17 We did not find any correlation between the balloon diameter to aortic annulus ratio and occurrence or increase in aortic regurgitation.1 ,16 Data reported by the valvulotomy and angioplasty of congenital anomalies registry showed, in contrast, some influence of the average balloon to aortic annulus ratio on aortic regurgitation.2 However, in that series of patients the maximum balloon to annulus ratio was 1.5, while in our series it was 1.25. The incidence of early severe aortic regurgitation in our series was extremely low (2.2%); however, Witsenburget al, employing a 0.9 to 1 annulus to balloon ratio, reported a 14% occurrence of early severe aortic regurgitation.7 Thus the possible role played by different valve morphologies has to be considered.1 ,18
A successful outcome was achieved in more than 80% in all the groups, in accordance with data reported by other investigators,8 ,15 confirming that balloon aortic valvoplasty is an effective procedure. The degree of gradient reduction was similar in all groups, suggesting that the procedure is technically feasible at any age.
MID-TERM RESULTS
Our data confirm that balloon aortic valvoplasty is compatible with excellent survival and a relatively slight need of reintervention at mid-term follow up.1 ,7 ,16
Survival in group 1 was significantly worse than in the other two groups, mostly because of early deaths (from cardiac failure or postoperatively). Sudden death was never observed in our series. This could reflect either the relatively short follow up or the good haemodynamic results obtained. Moore et alalso reported a low incidence of sudden death in their series.1
Freedom from events, including repeat balloon aortic valvoplasty or surgery, was not substantially different between the three groups, although patients in group 1 tended to have a higher mortality and a greater need for repeat balloon dilatation and surgery. Group 2 patients appeared to be more free of events than group 3 patients; however, we believe this was purely a result of a shorter follow up. Our data suggest that the use of balloon aortic valvoplasty as a palliative procedure, while offering excellent survival prospects, is likely to be followed by the need for repeat intervention.1 ,7 ,16 ,19
Redilatation after balloon aortic valvoplasty was common. Comparison with results from other institutions is impossible because of the extreme variability of criteria for redilatation. The interval between the first and subsequent valvoplasties was shorter in group 1 and 2 than in group 3. This could reflect the particular characteristics of aortic stenosis in small babies, while the relatively high incidence of redilatation in group 3 may be due to the longer follow up. In this group the relatively long interval between first and second balloon dilatations allowed appreciable body growth and the possibility of using larger balloons with a lower operative risk.
The need for surgery was significantly greater in group 1 and involved surgical valvotomy, surgery for associated diseases, or surgery for the development of a subaortic membrane, which was observed in two of 15 surviving neonates. To our knowledge the development of a subaortic membrane in neonates with critical aortic stenosis has not been reported before. These data contrast with those of Hawkinset al, who showed that the need for aortic valve surgery was unrelated to age at time of balloon valvoplasty.20
The incidence of surgery in group 3, similar to that previously reported,1 ,19 was greater than in group 2, probably because of a longer period of observation. Surgery in this group was, with no exceptions, related to valve replacement, mostly for pure severe aortic regurgitation, as reported by other investigators.19 Valve replacement was performed a considerable time after balloon valvoplasty, allowing the use of relatively large prostheses. To date, no patient has undergone prosthesis replacement.
The maximum Doppler gradient remained relatively stable in all groups. At the latest follow up, only 25% of the patients had a maximum Doppler gradient of more than 60 mm Hg, suggesting that balloon valvoplasty can have long lasting beneficial effects in the majority of patients over one year of age. The stability of the maximum Doppler gradient at mid-term follow up has been highlighted before.7 ,11 ,12 ,17 ,21
Aortic regurgitation is a well known early and late complication of balloon aortic valvoplasty. Historical comparisons are of limited value owing to different methods of assessing aortic regurgitation. Witsenburg et al report a 25% late incidence of severe aortic regurgitation7; most investigators, however, agree that moderate to severe aortic regurgitation occurs in only a minority of patients,16with progression of regurgitation in over 50% of cases.7 ,11 In our patients, the incidence of aortic regurgitation did not increase significantly with time, although some degree of regurgitation was found in all patients undergoing balloon aortic valvoplasty in the neonatal period. The incidence of severe aortic regurgitation in the overall series was relatively low.
CONCLUSIONS
Surgical repair of the aortic valve is considered an excellent technique to repair congenital aortic stenosis at any age. Randomised trials suggest that surgery offers results comparable to those of balloon aortic valvoplasty both in neonates and in older children.15 ,21 Our observations suggest that balloon aortic valvoplasty is also an effective technique, which can be employed even in critically ill neonates. Balloon valvoplasty is effective both as a primary procedure or after surgical valvotomy. Like surgical valvotomy, it must be considered as a palliative procedure, owing to the regular need for repeat intervention, especially in neonates.
More than 50% of patients subjected to balloon valvoplasty beyond one year of age are event free after 10 years. Most of these have mild to moderate aortic regurgitation, a maximum Doppler gradient of less than 60 mm Hg, and lead a normal physical and social life. Previous observations have stressed that such patients remain in stable health over periods of several years.20