Article Text

Abstract
OBJECTIVE To determine the clinical features and long term prognosis of infective endocarditis in patients who were not drug addicts.
DESIGN Prospective case series.
SETTING A university hospital that is both a referral and a primary care centre.
PATIENTS 138 consecutive cases of infective endocarditis diagnosed and treated from January 1987 to March 1997.
RESULTS Mean patient age was 44 (20) years old. 95 patients (69%) had native valve endocarditis and 43 (31%) had prosthetic valve endocarditis. Staphylococci were the causal microorganisms in 34% of cases and streptococci in 33%. Severe complications occurred in 83% of patients and 51% of patients underwent surgery during the active phase (22% was emergency surgery). Inpatient mortality was 21%. During a follow up of 56 (44) months, 10 patients (9%) needed late cardiac surgery and seven (5% of the whole series) died. Overall 10 year survival was 71%. There were no significant differences in survival depending on the type of treatment received during the hospital stay (medical or combined medical–surgical).
CONCLUSIONS A high early surgery rate is related to good long term results and does not increase in-hospital mortality. Medical treatment, however, also offers favourable long term results in cases of responsive infective endocarditis where poor prognostic factors are absent.
- infective endocarditis
- staphylococci
- streptococci
Statistics from Altmetric.com
Untreated infective endocarditis is one of the few universally fatal infectious diseases. The poor prognosis of the disease is not only attributable to the considerable morbidity and mortality during the active phase of the disease, but also to late complications and sequelae occurring once the infection has been eradicated.1 ,2 Prognosis in patients surviving the initial stages of infective endocarditis is dependent on three main factors: substantial risk of recurrence (recently estimated at 0.3–2.5/100 patient years); the need for valve replacement during follow up as a result of valve lesions caused or exacerbated by endocarditis; and, lastly, death particularly from heart failure.3 ,4
As a result of advances in diagnosis, improved antimicrobial treatment, and earlier detection and management of complications, the short term prognosis for this disease has improved over the past few years. Improvements in microbiology techniques, together with the recent introduction and development of transoesophageal echocardiography, have made a substantial contribution to ensuring early diagnosis, providing accurate information on possible complications and their monitoring.5-7 Very few series, however, refer to long term survival in infective endocarditis in the era of transoesophageal echocardiography.6 ,8
We conducted a prospective study involving cases of infective endocarditis in non-intravenous drug users and their short and long term survival.
Patients and methods
A prospective study was conducted involving all consecutive cases of infective endocarditis in non-intravenous drug users diagnosed and treated at our centre between January 1987 and March 1997. Our hospital is a tertiary centre providing health care cover for both the local population (480 000 inhabitants) and the surrounding area, making a total referral population of 1 389 000 inhabitants.
The following data were recorded for each patient: age, sex, predisposing heart disease, evaluation of the predisposing heart disease, site of infection, type of endocarditis, valve involved, causal organism, echocardiographic findings, cardiac and extracardiac complications, treatment given during hospitalisation, surgical requirements, and mortality. Recurrence of the disease, the need for surgery, and death were evaluated during the follow up period.
Until 1994, all cases of infective endocarditis were diagnosed on the basis of the criteria proposed by Von Reyn and colleagues9and on the criteria of Durack and colleagues10 thereafter. All intravenous drug users were excluded from the study. Early prosthetic valve endocarditis (PVE) was considered when the episode occurred in the first two months following heart surgery, while intermediate and late PVE was diagnosed when the episode developed 2–12 months and more than one year after surgery, respectively. Transoesophageal echocardiography has been available in our hospital since 1990. All patients received antibiotic treatment in accordance with the susceptibility of the causal organism. Treatment was administered for 4–6 weeks according to both the causal agent and the type of infective endocarditis involved. Surgical treatment was indicated during hospitalisation in the following circumstances: moderate to severe heart failure; significant valve regurgitation with major ventricular volume overloading; repeated major emboli (two or more); severe mechanical complications; in episodes caused by virulent organisms which cannot be eradicated by antibiotic treatment alone (fungi, Brucella species,Coxiella species); in cases of early PVE; endocarditis on pacemaker leads; and in cases of persistent sepsis despite theoretically adequate antibiotic treatment. Emergency surgery was defined as surgery for patients with life threatening conditions that could not be postponed for more than 24 hours, and elective surgery comprised those interventions that could be delayed for longer time periods without risk to the patient.
All survivors to the in-hospital phase were included in the prospective follow up. Blood cultures, one and two months postdischarge, were performed with a clinical check up and an echocardiographic study to assess anatomy and any haemodynamic sequelae of the disease. When blood cultures were negative two months after discharge, the infection was considered to be cured. Death occurring during the six weeks postdiagnosis was considered as early mortality. A positive blood culture for the same causal organism two months after discharge was classed as relapse, while recurrence was taken to be a new episode of infective endocarditis caused by a different organism or by the same organism as the initial infection but arising over two months postdischarge. During follow up, some patients required valve replacement either because of the course of their underlying heart disease or because of the haemodynamic repercussions of valve lesions caused by the infection.
STATISTICAL ANALYSIS
All qualitative variables are expressed as percentage and quantitative variables as mean (SD). The differences between patient groups have been evaluated by Fisher's exact test or χ2test for qualitative variables, while Student'st test was used for unpaired data in the case of quantitative variables.
Overall survival curves (including early mortality) and long term survival curves for patients surviving the active phase are given. The Kaplan-Meier actuarial method was used for the survival curves. Comparison of the survival curves of the different subgroups was made using the Mantel log rank test. Values of p < 0.05 were considered significant.
Results
GENERAL CHARACTERISTICS
Our series comprises 138 cases of infective endocarditis in 126 non-intravenous drug users. The diagnosis of infective endocarditis was made according to the aforementioned criteria. The diagnosis of infective endocarditis was definite in 124 cases (pathologically definite in 70 cases—those who underwent surgery—and clinically definite in 54 cases). Fourteen patients (10%) were classified as possible endocarditis. When retrospectively applying the Duke criteria, none of our patients was rejected. Mean patient age was 44 (20) years, with ages ranging from 2 months to 72 years. Thirteen of the cases were patients under the age of 14 years. Ninety five (69%) cases were native valve endocarditis (NVE) and 43 (31%) cases were PVE (table1).
General characteristics in 138 cases of infective endocarditis in non-drug addict patients
A presumed portal of entry was identified for 38% of the cases. Dental procedures had been performed in 13 patients (9%). In four cases (3%) the portal of entry was the genitourinary tract (three cases of prostatectomy and one case of urinary catheter related infection) and in three cases (2%) it was the digestive tract (two patients with colon cancer and one with active ulcerative colitis). Other entry routes were: cutaneous abscesses caused byStaphylococcus aureus in two patients; intravenous catheters in eight patients; heart surgery, which was performed 7–10 days before the start of infective endocarditis symptoms in six patients (prosthetic valve replacement in five and correction of tetralogy of Fallot in one patient); and haemodialysis in six patients. Predisposing heart disease was present in 68 patients with NVE (80%) (table 1). The most common heart condition in NVE was aortic regurgitation (10%), followed by mitral valve prolapse, aortic stenosis, and congenital heart disease (8% each). Infection occurred on the left side of the heart in 86% of the cases, with no significant differences between the mitral and aortic valves. A previous infective endocarditis event was more common in PVE than in NVE patients (23%v 2%, p < 0.001). Fifty eight patients (42%) were referred to our institution because of infective endocarditis or suspicion of infective endocarditis. The median duration of the first symptom before diagnosis was shorter in local patients (26 days, range 7–130 days) than in referred patients (37 days, range 20–210 days) (p < 0.05).
Table 2 shows the aetiology of infective endocarditis. No causal organism was found in 16 patients (11 patients in the first half of the study and five in the last five years, p < 0.1). Twelve of these patients (75%) had received antibiotics in the week before blood culturing. Staphylococcus was the most frequent organism responsible in the NVE group, while in PVE cases streptococcal infection was more common.
Infective microorganisms in 138 cases of endocarditis in non-drug addict patients
There were four cases of infective endocarditis on pacemaker leads. In one case an abscess at the tip of the lead in the right ventricle implant site was detected. In the rest, echocardiography showed bacterial growth on the lead around the tricuspid valve. All episodes were caused by S aureus. Three patients were operated on in the active phase. Two of them had a favourable outcome and the third patient died from postoperative malignant ventricular arrhythmias. The fourth patient refused surgery but had a favourable outcome with medical treatment only.
ECHOCARDIOGRAPHIC DATA
All patients were examined by transthoracic echocardiography and, from 1990 onwards, the last 94 patients were also examined by transoesophageal echocardiogram (68%). Echocardiography detected vegetations in 86% of the cases (59% with transthoracic echocardiography and 92% with transoesophageal echocardiography, p < 0.01) This difference was greater in the PVE group (24%v 81%, p < 0.001) than in NVE group (75% v 97%, p < 0.05). When only those cases that were verified at surgery were taken into consideration, transthoracic echocardiography gave a sensitivity of 66% compared with 100% sensitivity for transoesophageal echocardiography (p < 0.01). Sensitivity was similar for mitral and aortic valve infective endocarditis. Beside the vegetations, echocardiography revealed further findings or complications in 30 patients (22%). Surgery was indicated during the active phase according to the echocardiographic findings in all these patients (table 3).
Other echocardiographic findings in a series of 138 cases of infective endocarditis in non-drug addict patients
IN-HOSPITAL COMPLICATIONS
Cardiac and extracardiac complications were a frequent finding (83%). The most common complication was the onset of heart failure (40%), followed by embolism (30%), neurological disorders (20%), persistent sepsis (19%), acute renal failure (12%), metastasic abscesses (11%), and mycotic aneurysms (6%). There were no differences between NVE and PVE as regards complications (table4).
Cardiac and extracardiac complications in both types of infective endocarditis in a series of 138 cases in non-drug addict patients
TREATMENT
All patients received antibiotic treatment. Forty seven patients with NVE (50%) and 23 patients with PVE (53%) underwent surgery during the active phase. Elective surgery predominated over emergency procedures (29% v 22%). Seven patients (5%) died on the day of admission before receiving any treatment. The most common indication for surgery was congestive heart failure (48%), followed by persistent sepsis (26%). Other indications included underlying heart disease (7%), repeated embolism (4%), glomerulonephritis with acute renal failure despite antibiotic treatment (4%), and the causal organism (2%). Surgery was more frequently required in aortic infective endocarditis (40/59 patients, 67%) than in mitral infective endocarditis (22/59 patients, 38%) (p < 0.05).
The most frequent cause contraindicating surgery during the hospitalisation stage was a good response to medical treatment alone or a favourable prognosis a priori (27%), patient age (8%) or any formal contraindication to surgery (3.5%). There was one case of patient refusal and one involving a patient diagnosed with a carcinoma of the colon with endocarditis involving a pacemaker lead, who refused any kind of surgery but who later responded well to antimicrobial treatment.
EARLY MORTALITY
Twenty nine patients (21%) died in hospital (19 patients (20%) with NVE and 10 patients (23%) with PVE, no significant difference). The highest mortality rate was registered among early PVE with four of the eight cases dying (50%). Four of the 14 intermediate PVE cases (28%) died as did two of the 20 late PVE patients (10%). Mortality was 20% among patients receiving antibiotic treatment alone and 21% for patients in the combined medical–surgical treatment group. The seven patients who died during the first 24 hours after admission and who received no treatment at all have been included in the antibiotic treatment group. The most common cause of early mortality was of surgical origin (45%), followed by heart failure and cardiogenic shock (24%), brain haemorrhage (14%), postoperative pneumonia (7%), sepsis (6%), and pulmonary embolism (3.5%).
Mortality was 23% in the staphylococcal endocarditis group, 14% in the streptococcal group, and 16% in the other microorganism group. Eight of the 15 patients in which the causal agent could not be identified also died. The causal agent was identified in only 69% of the patients who died during the hospitalisation stage, compared with 94% of the survivors (p < 0.001). Other short term bad prognostic factors were older age (p < 0.01), the onset of cardiac complications (p < 0.01), and the need for emergency surgery (p < 0.05). Prognosis was not affected by the type of infective endocarditis (NVE or PVE) or by site and causal agent.
FOLLOW UP
The average follow up for the 109 patients surviving the active phase was 56 (44) months (range 12–135 months).
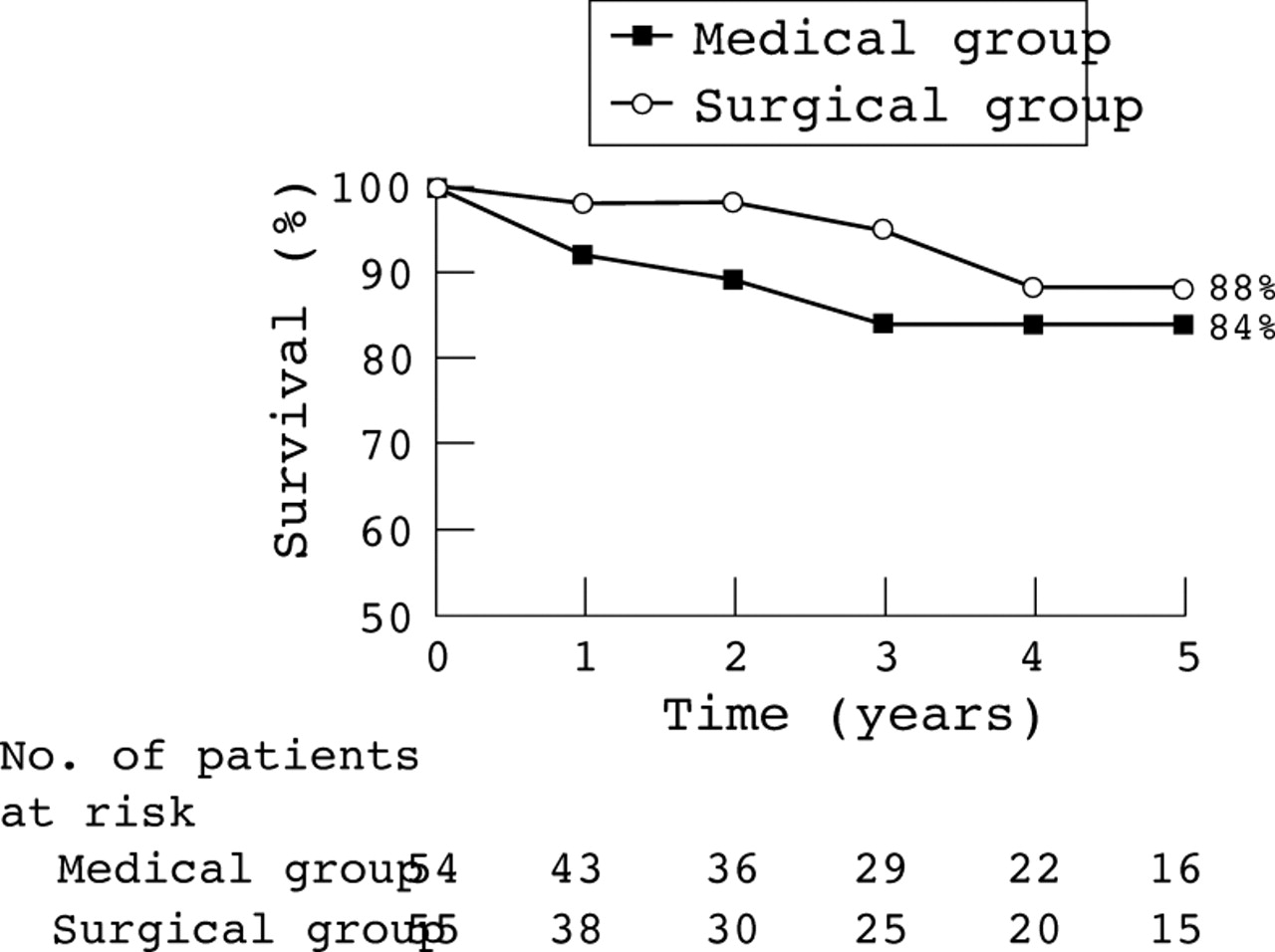
Overall survival (including mortality during the in-hospital phase) was 75% at one year and 71% at five and 10 years (fig 1). Excluding those patients who died during the active phase, one year survival was 96% with a five and 10 year survival rate of 92%. Follow up event free survival at one year was 92%, and 82% at five and 10 years (fig 2). Overall survival for NVE was 78% at one year and 76% at five years, and for PVE it was 67% and 59%, respectively (p < 0.01). In the cases of late PVE, one year survival was 85% and five year survival was 80% (fig 3). One year and five year survival rates for NVE in survivors to the active phase were 98% and 96%, while in PVE they were 90% and 82%, respectively (p < 0.05) (fig 4). Regarding the type of treatment received during hospitalisation, follow up event free survival was similar in both groups (medical and surgical) (fig5).

Kaplan-Meier survival curves. Follow up event free survival in a series of 138 cases of infective endocarditis.
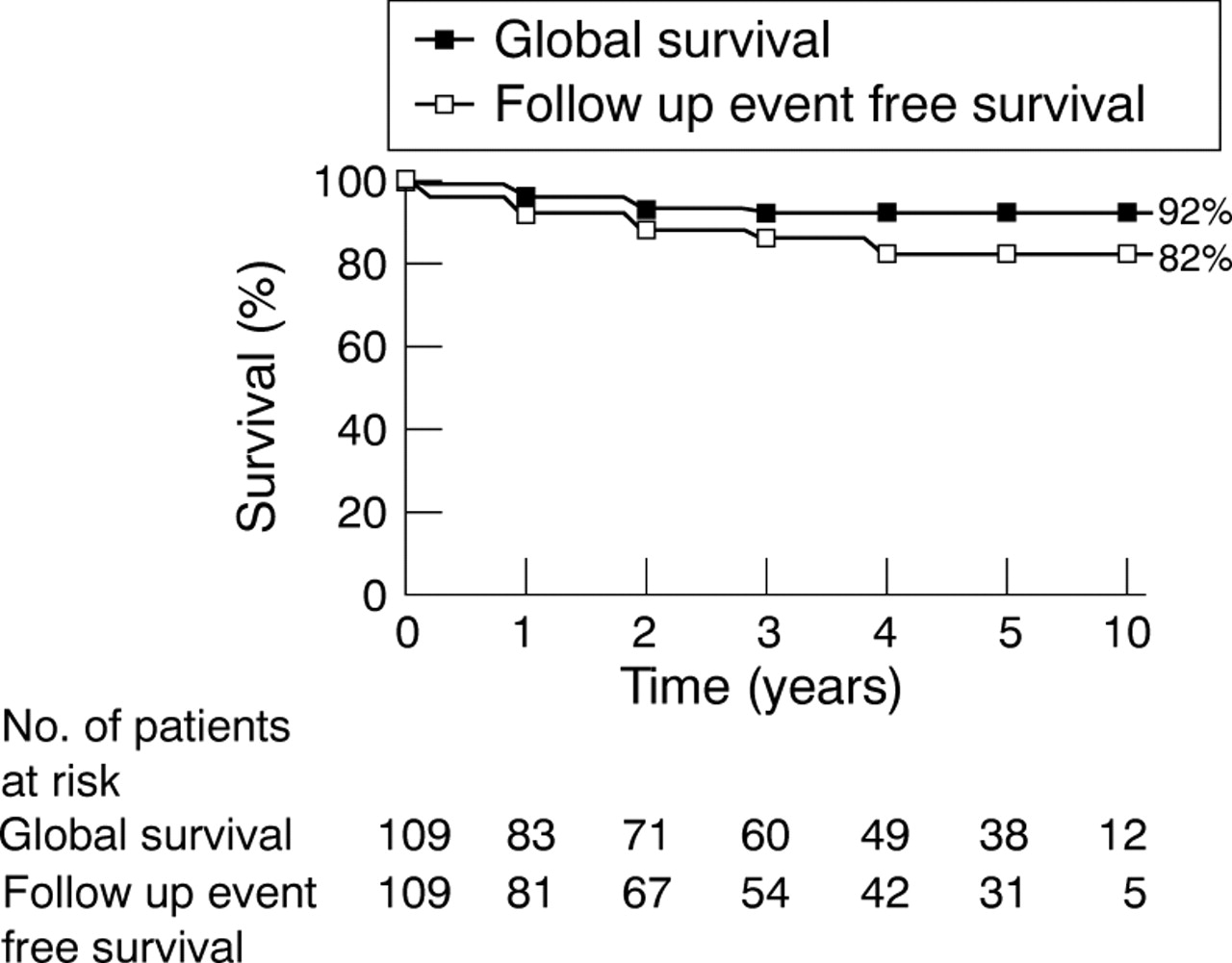
Kaplan-Meier survival curves. Follow up event free survival in 109 survivors to the active phase.

Overall survival curves according to the type of infective endocarditis. Differences between native (NVE) and prosthetic (PVE) valve endocarditis, and between late and one year PVE, are significant.

Overall survival curves in 109 survivors to the active phase according to the type of infective endocarditis. Differences between NVE and all PVE are significant but not between NVE and late PVE.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Follow up event free survival curves in 109 survivors to the active phase depending on the treatment (medical or combined medical–surgical) received in the active phase. No significant differences in survival were observed.
There was recurrence of infective endocarditis in seven of the 109 survivors (6%). Four of these seven patients also underwent surgery (two of these infective endocarditis cases were caused by Q fever). Of the remaining three patients, one died before surgery because of a brain haemorrhage while the other two responded satisfactorily to medical treatment alone. There was no relapse.
Ten patients (9%) required late surgery during follow up, and only one patient (1.4%) required a second operation (because of a severe regurgitation leak). In most cases, surgery was performed in the first two years following the infective endocarditis. All presented a favourable postoperative course, and no deaths occurred. Eight of these 10 patients received valve replacements while the remaining two underwent a percutaneous procedure (percutaneous mitral valvuloplasty in two patients with rheumatic mitral stenosis). Surgery was performed on six of the patients because of progression of the underlying heart disease, while the indication for surgery in the remaining four patients was the recurrence of the infective endocarditis.
Seven patients died during follow up (5% of the total in the series), mainly during the first two years after the episode. In two of these cases, death was related to a new episode of infective endocarditis; in a further two cases (one of which also involved prior severe left ventricular dysfunction) the cause was sudden death. One patient, who had refused surgery, died from a brain haemorrhage caused by a ruptured mycotic aneurysm, while a further two patients died from congestive heart failure associated with severe pulmonary hypertension.
At the end of the follow up period, 89 patients were alive and free of events—64% of the series.
Discussion
This 10 year study, comprising 138 cases of infective endocarditis in non-drug addict patients treated at our hospital, is similar in size to other series recently reported.11-14 Possible referral bias affecting series like ours, conducted in tertiary hospitals, should not be overlooked.
Complications of the infective endocarditis during the active phase were very frequent, occurring in 83% of the cases. These figures, similar to those reported by other authors,1 ,2 ,15 ,16reflect the diversity of clinical manifestations and the severity of the disease. As a general rule, complications in NVE are less frequent. In our series, however, rates were similar to PVE complications, probably related to aggressive microorganisms, a nosocomial origin, or to the delay in diagnosing the disease.
Our series shows a high incidence of surgery performed during the active phase of the disease (51%), regardless of the type of infective endocarditis, and on an elective basis, following stabilisation of the condition. Seven patients died in the first few hours after admission before surgery could be considered. The delay in diagnosing the disease is an important factor affecting the high rate of surgery. A delayed diagnosis may either be caused by non-specific initial symptoms, by ignorance of some of the relatively common causal agents in our area (for example, Coxiella burnetti) or by the unavailability of transoesophageal echocardiography at all hospitals in the area. A delay in diagnosis and therefore in the institution of antimicrobial treatment is associated with a higher rate of complications, thus requiring a greater number of surgical procedures. Comparing our incidence of surgery performed during the active phase with those reported in other series,6 ,8 ,17-19 early elective surgery is performed more frequently at our centre—that is, once the disease has been stabilised by instituting appropriate antibiotic treatment. Trends in literature over the past two decades, however, reveal an increase in the number of patients undergoing surgery during the active phase. For example, in the series of Von Reyn and colleagues,9 18% of patients underwent surgery. In the series of Malquarti and colleagues,20 conducted between 1970 and 1982, 26% of NVE cases were operated. More recent publications report rates for surgery of 15–34%.6 ,8 ,18In the series presented here, 50% of NVE and 53% of PVE cases underwent surgery during the active phase.
Unlike in other studies,6 ,13 ,14 the most frequent cause of early mortality is not heart failure or persistent sepsis but is surgical in origin, related to a high number of early surgical procedures. Most deaths occur in cases of emergency surgery—that is, in haemodynamically unstable patients with severe complications. Patients who only received medical treatment, however, responded favourably and did not, therefore, require surgery. In the light of these factors, the results for each of the two groups are not easily comparable, since a favourable clinical course would give a bias towards the medical treatment group; however, those patients who died during the first few hours after admission and therefore did not undergo surgery have also been included to counteract bias. Higher mortality was seen in cases where the causal agent was not identified (50% of patients with negative blood cultures). Other factors indicating early mortality were age, the presence of cardiac complications, persistent sepsis, and the need for emergency surgery. There was no significant difference in mortality between patients following medical treatment (20%) or those undergoing surgical treatment (21%). Although they vary from one series to another, surgical mortality rates have tended to decrease over recent decades owing to technological developments, with rates as low as 14% being recently reported.21 ,22
In the very few studies dealing with follow up on infective endocarditis, a large number of patients required late surgery, which contrasts with our findings. In the reports mentioned above, late surgery rate ranged from 27–47%.8 ,18 ,19 In our series, with a mean follow up of 56 months, only 10 patients (9% of the survivors) underwent late surgery as patients had undergone elective surgery during the active phase of the disease. Only one patient had to be reoperated on. Low late surgery rate may be related to low late mortality rate (5%) which is lower than those reported by other authors. At the end of the follow up period, 67% of patients were alive and event free, which contrasts with figures of 22–38% reported by others.8 ,18
Overall survival (including in-hospital mortality) in the series of Delahaye and colleagues,3 conducted between 1970 and 1982, was 57% at five years while our series yields an overall five year survival rate of 71%. When related to the type of infective endocarditis involved, in the series of Calderwood and colleagues,19 conducted between 1975 and 1983, the five year survival rate for PVE was 60%, while the rate in our series is 82%. In the series of Tornos and colleagues18 the five year survival rate for NVE was 88% and for late PVE 80%,8 while in our series the rates were 96% and 82%, respectively. More recently Schultz and colleagues,6 in their series conducted between 1989 and 1993, report a one year survival rate for survivors to the active phase of 73% in NVE and 83% in late PVE, compared with rates of 98% and 94% in our series. When comparing the type of treatment received during the active phase (medical or combined medical–surgical), the overall, event free survival rate in the surgical group was slightly higher than in the medical group (no significant differences).
In conclusion, our results seem to indicate that a high elective surgery rate in the active phase of infective endocarditis improves long term survival rate without increasing early mortality. However, in cases of responsive infective endocarditis with absence of poor prognostic factors, medical treatment also offers favourable long term results.