Article Text

Abstract
OBJECTIVE To determine if appropriate advice had been given to adults with congenital heart disease regarding safe and effective exercise, and to assess pre-existing misconceptions of the potential benefits and dangers of exercise.
DESIGN An anonymous self assessment questionnaire.
SETTING A tertiary referral clinic.
PATIENTS 99 adults (57 men, 42 women) with congenital heart disease, mean age 25.6 years.
MAIN OUTCOME MEASURES The extent and nature of exercise advice given over previous years; a measure of current activity level compared with the American Heart Association recommendations; and an assessment of exercise limiting symptoms and a description of barriers to further exercise.
RESULTS 44% of the cohort assumed all exercise was safe despite their cardiac disease. A health care professional had only raised the issue of specific exercise advice in 28 cases. Of those given instruction it was more common to receive prohibitive advice (30%) than to be encouraged to take more exercise (19%). Despite this 61% were involved in some form of at least light exercise. The most prevalent barriers to exercise were current symptoms (32.3%), lack of interest in exercise (24.2%), and health fears (16.1%).
CONCLUSIONS The education of adults with congenital heart disease regarding exercise and its potential benefits and limitations is suboptimal even in a specialist clinic.
- congenital heart defects
- exercise prescription
Statistics from Altmetric.com
The social, medical, and psychological benefits of exercise and participation in sporting activities are well established. Even in individuals with significant cardiac morbidity, such as those with cardiac failure, exercise may have a positive effect.1Despite this physicians have been reluctant to encourage patients with heart conditions to take regular exercise and have neglected to give specific recommendations.2 This is particularly true in the area of congenital heart disorders which requires specialist knowledge and understanding of the anatomical and physiological implications of the patient's condition.
In this young patient group the ability to exercise and participate in sport is especially important, and conflicting agendas may arise when advising these patients. The physician may be left to balance the enthusiastic youngster who underplays a physical limitation and the anxious overprotective parent. Under these circumstances there is a tendency to discourage patients from exercise “to be on the safe side”, to give woolly advice, or to ignore these issues altogether.3
In response to this dilemma the American Heart Association (AHA) committee on congenital cardiac defects of the council on cardiovascular disease in the young published recommendations for both the recreational and occupational activities of young patients with heart disease.4 These are diagnosis specific guidelines which grade the exercise recommendations for patients on a scale of 1 (no restriction) to 5 (extreme limitation) (table1).
AHA activity guidelines for patients with congenital heart disease
One of the roles of regional adult congenital units has been to convey specialist advice, such as the AHA recommendations, to both patients and other health care providers such as the family practitioner. By having a supraspecialist unit, lifestyle issues and patient education can be addressed in an informative manner.
The aim of this study was to determine, in a group of adults with congenital heart disease attending a tertiary referral centre, if appropriate advice had been given regarding safe exercise or if patients had persisting misconceptions regarding the potential benefits and/or dangers of exercise and sport.
Methods
Subjects from an adult congenital outpatient clinic database at the Western Infirmary, Glasgow, were asked to complete a self assessment questionnaire either posted to them or given to them at the clinic. The only exclusion criteria to the study was a significant learning difficulty. Questions focused on current activity level, exercise prescription, and perceived barriers to exercise.
Subjects were asked if a doctor had ever mentioned, without being prompted, how much exercise it was safe to perform. Patients were asked to describe the amount of exercise the doctor said they could safely do using the AHA categories below. This classification scale was also used to describe the subjects' current exercise level and an assessment of how much activity they believed was safe or they were happy to do. In addition subjects were asked about five symptoms: breathlessness, chest pain, tiredness, palpitation, and muscle fatigue. They were instructed to grade these specific symptoms on a scale of 0 (no symptoms) to 10 (severe limiting symptoms). “Total symptom scores” were also calculated with a maximum of 50 points—that is, a score of 10 for each of the five symptoms. There was also an opportunity to volunteer alternative limiting non-cardiac symptoms.
Results are described as numbers and percentages of subjects responding to that question. When comparing two groupst tests were used.
Results
Ninety nine patients (57 men, 42 women) were analysed. Mean age of the subjects was 25.6 years (range 11–51 years; only two patients were under 16 years old). The mean time attending the clinic was 4.7 years (range from first visit to 17 years). Fifty six of 86 (65%) of the cohort had been initially referred from the regional paediatric cardiac unit, 27% from their family practitioner, and 8% from other hospital specialities (including general cardiology).
DIAGNOSIS
The patient group had a heterogeneous selection of diagnoses. This included aortic valve pathology (23.5%), ventricular septal defects (14.8%), tetralogy of Fallot's and pulmonary valve pathology (11.3%), coarctation of the aorta (5.2%), Marfan's syndrome (4.4%), transposition of the great arteries (2.6%), congenitally corrected transposition (1.7%), palpitations and conduction defects (10.4%), mitral valve pathology (4.3%), left to right intracardiac shunts (6.1%), complex non-cyanotic lesions (5.2%), Eisenmenger's (3.4%), familial hypertrophic cardiomyopathy (1.7%), and a few with structurally normal hearts or left ventricular hypertrophy (7%). Thirty eight (38.4%) of the cohort had had previous cardiac surgery, either palliative or curative.
SYMPTOMS
Only 10 (10.3%) patients were asymptomatic, and 26 (26.8%) had at least one symptom that was relatively disabling (severity of 8 or more). The most common “high scoring” symptoms were breathlessness and palpitation rather than chest pain. Table 2 depicts the “total symptom scores” for the group. Ten subjects reported other symptoms which included dizziness, cyanosis, and depression.
Total symptom scores (scale of 0–50)
SEEKING EXERCISE ADVISE
Only one third (37.3%) of the cohort had ever asked a doctor about how much exercise they could do safely. Of this group it was most common to consult either the general practitioner or the cardiologist; two individuals stated that they had sought the advice of the paediatrician before their transfer to the adult services. The most common reason for not seeking advice was the assumption that all exercise was safe (table 3).
Reasons for not consulting medical advice
EXERCISE PRESCRIPTION
In 71% of individuals the topic of exercise had never spontaneously been raised by either their paediatrician, general practitioner, or the cardiologist at the adult clinic. Only 19% had been encouraged to take more exercise. Eleven (11%) patients were specifically told that they had no exercise limitation from a cardiac point of view. It was more common, however, to be given advice about which forms of exercise were prohibited (30%), with isometric weight training being mentioned to eight individuals.
Those with “high risk” lesions (groups 3 and 4) were compared to those with “low risk” (groups 1 and 2) defects. Only seven of 21 patients in the high risk group were given specific advice. In particular only two of seven patients with Eisenmenger's or severe pulmonary hypertension were advised to avoid strenuous activity. Three patients in this high risk group were given inappropriately reassuring advice—that is, encouraged to exercise to a greater level than that suggested by the AHA classification. Of the 55 patients with less haemodynamically significant lesions, eight were given inappropriately inhibitory advice. The consequences of inappropriate advice in the first group is obviously more clinically significant.
CURRENT ACTIVITY LEVEL
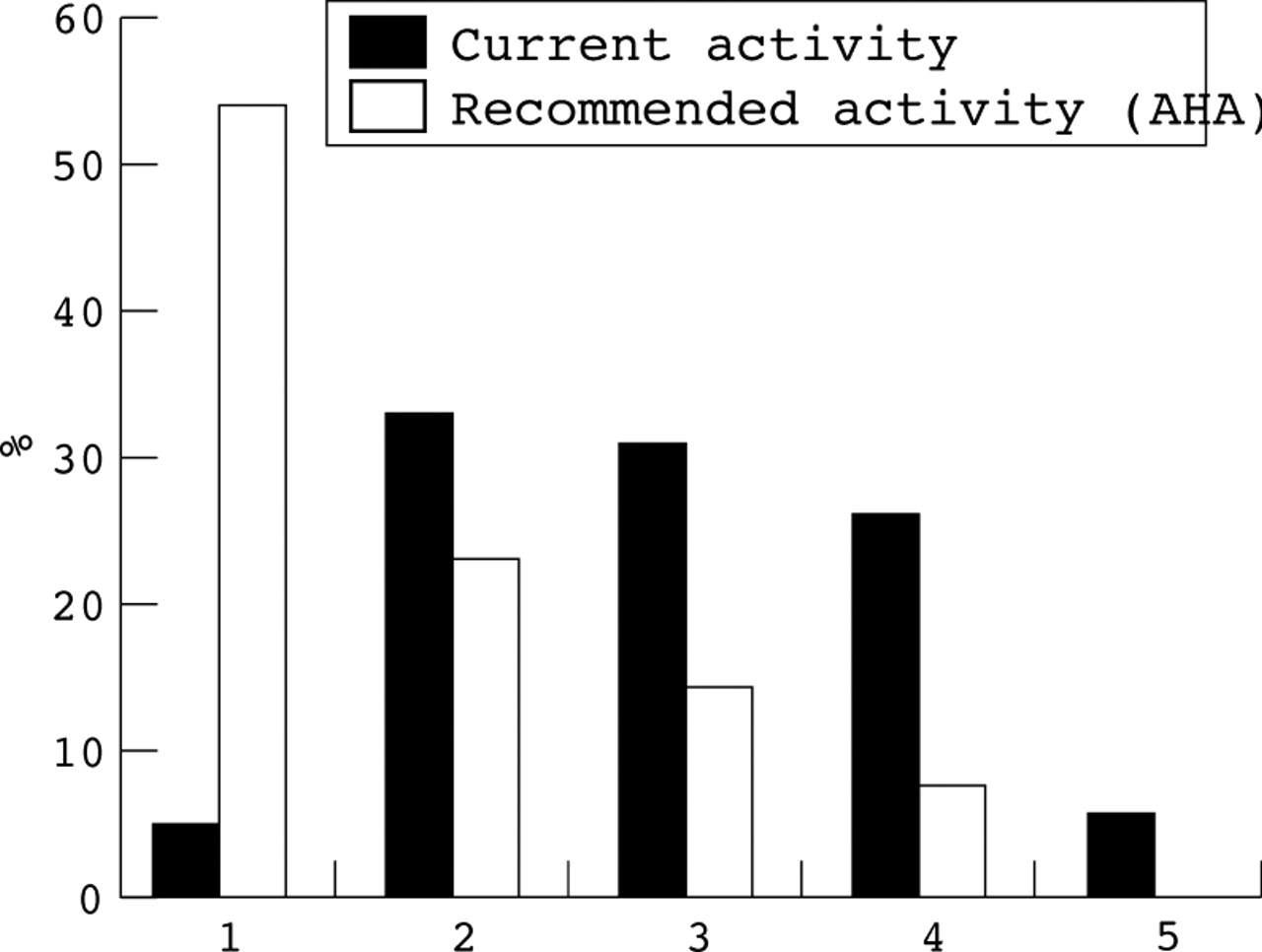
Five patients were very active (no limitation), 33% stated they were involved in regular moderate exercise, 31% were involved in light exercise, 25% did not perform any regular physical exercise, and five patients were severely limited (housebound/wheelchair bound). Figure 1shows the discrepancy between patient's actual activity levels and the AHA recommendations for optimum or maximal activity.

{kind=link}
Current activity level (scale 1–5) of study subjects compared to AHA recommended activity level.
Patients were asked about the amount of activity they would be happy to perform. Ten (10%) patients felt they could happily perform any exercise including endurance training and contact sports. More commonly the response (27%) was to undertake light exercise (swimming, cycling, and golf). There was no significant difference between those who had and had not been given specific advice regarding the amount of activity they were happy to perform.
BARRIERS TO EXERCISE
Symptoms prevented one third of patients exercising more frequently (table 4). Few patients (5%) stated that they were happy with their current level of activity. Health fears inhibited one in six subjects. The questionnaire specifically asked about parental concerns regarding participation in sport and exercise. Only three (3.3%) felt their parents had inappropriate concern with 43% expressing appropriate concern.
Barriers to exercise
Discussion
In this study the majority of patients with congenital heart disease were symptomatic, with one third being limited by cardiac symptoms. Symptoms often occurred in the presence of non-haemodynamically significant lesions. Physicians may be underestimating the degree of morbidity associated with a “cardiac diagnosis” in this patient group, and subsequently underestimating their need for detailed counselling regarding daily activities such as employment and leisure pursuits. Alternatively there may be misunderstanding within this patient group of the difference between significant “pathological” symptoms and “normal” symptoms indicative of a lack of physical fitness. In addition anxiety or preoccupation with one's health may contribute. If this is the case regular cardiac follow up may have a detrimental effect on a teenager's perception of his or her medical problems, equating a cardiac lesion with disability and functional limitation, unless these issues are handled sensitively.
Unfortunately an adequate discussion of the importance of fitness and a patient centred exercise prescription was rare. Few patients were encouraged to exercise more and advice was more often prohibitive, even though the majority of patients (78%) had lesions in AHA classes 1 and 2. This negative advice may have had some bearing on the discrepancy seen between the current level of activity and the AHA classes shown in fig 1. Without appropriate reassurance and encouragement many in this group may be unaware of the potential reversibility of some of their limitations.
The patient and physician misunderstandings regarding what was “safe” exercise were not all in the direction of being overprotective. Rather concerning was the fact that, of those patients who believed all exercise was safe, three were in either class 3 or 4—that is, patients who should have been given instructions to limit activity to light or no exercise.
In conclusion, there is room for a significant improvement in the understanding of safe and effective exercise, even in patients who attend paediatric and adult specialist services. In patients with lesions classified as AHA grades 1–3, focused advice can empower them to choose activities that will not only improve their health but increase their quality of life by helping to remove or modify many of the perceived barriers to exercise. Specialist adult congenital clinics with clinicians aware of these issues may go some way to redressing these problems, but improved methods of communication are needed. It is well recognised that written instruction has added weight over verbal communication alone.5 One such vehicle could be a “patient passport”, a small card or booklet given to the patient to document diagnosis and provide advice on issues such as endocarditis prophylaxis, exercise, general anaesthesia, and contraception. In a “high tech” world a “low tech” solution may improve the patients' understanding of their health problem and communication between health care professionals.