Article Text

Abstract
OBJECTIVE To evaluate the significance of commissural calcification, identified by transthoracic echocardiography, on the haemodynamic and symptomatic outcome of mitral balloon valvotomy.
METHODS Commissural calcification was graded from 0–4 using parasternal short axis transthoracic views. The morphology of the mitral valve was also assessed using the Massachusetts General Hospital echo score.
SETTING A tertiary cardiac centre in Scotland.
PATIENTS 300 patients were studied, 85 retrospectively and 215 prospectively. Mean (SD) age was 59.8 (12.7) years, range 13 to 87; 30% had been judged unsuitable for surgery. Median echo score was 6.8 (3.0), range 2–16.
MAIN OUTCOME MEASURES Immediate increase in mitral valve area and in New York Heart Association functional class 1–3 months after balloon valvotomy.
RESULTS On univariate and multivariate analysis, commissural calcification grade was a significant predictor of achieving a mitral valve area of > 1.50 cm2 without severe mitral reflux. Its influence was greatest in patients with an echo score ⩽ 8: those with commissural calcification grade 0/1 had significantly greater improvement in valve area and symptom status than those with grade 2/3; the proportions of patients achieving a final valve area of > 1.50 cm2 were 67% and 46%, respectively (p < 0.05). In patients with an echo score of > 8, the influence of commissural calcification was smaller and not significant.
CONCLUSIONS Commissural calcification as assessed by transthoracic echocardiography is a useful predictor of outcome in patients with otherwise “good” valves (echo score ⩽ 8). Calcification of one commissure or more predicts a less than 50% probability of achieving a valve area above 1.50 cm2and is an indication for valve replacement in those who are suitable for surgery.
- mitral balloon valvotomy
- commissure calcification
Statistics from Altmetric.com
The introduction of percutaneous transseptal mitral balloon valvotomy by Inoue and colleagues in 19841 was an important new option for the treatment of patients with mitral stenosis. In patients judged to have a mitral valve anatomically suitable for a commissurotomy, randomised trials2-5 have shown that balloon dilatation gives haemodynamic, echocardiographic, and symptomatic results equivalent to open and closed surgical valvotomy. In addition, in older patients with pronounced mitral valve degenerative change who are very high risk candidates for surgery, percutaneous balloon valvotomy can be undertaken safely and may provide palliative symptomatic improvement.6 ,7
When closed surgical valvotomy began in the 1950s, only physical signs and fluoroscopy were available to predict valve anatomy.8The early surgical experience9-11 and necropsy data12 showed leaflet rigidity, subvalvar change, and commissural fusion to be the three components that could contribute to obstruction in rheumatic mitral stenosis. The surgeons recognised that some commissures were sclerosed by fibrosis or calcification and resisted separation. The introduction of balloon valvotomy came at a time when echocardiography was available to examine mitral valve anatomy in more detail. To help predict the result of mitral balloon valvotomy, a transthoracic echo score was devised at the Massachusetts General Hospital13 ,14 to make a semiquantitative assessment of some of the degenerative changes found with stenosed mitral valves. This echo score assesses four valve characteristics: leaflet thickening, subvalvar change, leaflet mobility, and valve calcification. It does not, however, include assessment of commissural morphology. We have examined the effect of commissural calcification on the haemodynamic outcome after percutaneous mitral balloon valvotomy in a group of patients, many of whom were elderly, as is now typical in western countries.
Methods
PATIENTS
In 311 consecutive patients in whom mitral balloon valvotomy was attempted between 1986 and 1996, dilatation of the mitral valve was achieved in 300 (97%). Of these 300 patients, 235 (78%) were women and 65 (22%) were men. Mean (SD) age was 59.8 (12.7) years, range 13–87. A previous surgical valvotomy had been carried out in 23%. Twenty four per cent were in New York Heart Association (NYHA) functional class II, 50% in class III, and 26% in class IV. Atrial fibrillation was present in 215 (72%), while 82 (27%) were in sinus rhythm, and three (1%) in atrial flutter or nodal rhythm. The median echo score was 6.8 (3.0), range 2–16.
Patients were selected for percutaneous mitral balloon valvotomy if their mitral valves appeared anatomically suitable for improvement by a commissurotomy or if, regardless of valve morphology, they had unacceptably severe symptoms on medical treatment but were high risk candidates for cardiac surgery. Of the 300 patients, 89 (30%) had been judged unsuitable for surgical treatment. There was thus a wide spectrum of degenerative mitral valve change. Patients had been referred for mitral balloon valvotomy from hospitals throughout Scotland, and 97% were born in the UK.
ECHOCARDIOGRAPHIC ASSESSMENT
Before balloon valvotomy, all patients underwent full transthoracic cross sectional echocardiography using an ATL Ultramark 9 (Bothell, Washington, USA), Hewlett-Packard Sonos 2000 (Andover, Massachusetts, USA), or Acuson 128 XP/10 ultrasound scanner (Mountain View, California, USA). The final 196 patients also had a transoesophageal study immediately before the procedure to identify left atrial thrombus.
The mitral valve was scored on the transthoracic images as described by Wilkins and colleagues and Abascal and associates.13 ,14This involves semiquantitative assessment of leaflet mobility and thickening, subvalvar change, and valve calcification; each abnormality has a possible score of 0 or 1 to 4, corresponding to zero/mild to severe abnormality and giving a possible total echo score of between 2–16.
For assessment of the commissures the mitral valve was examined in the short axis parasternal view. The echo beam was scanned repeatedly through the mitral apparatus to assess commissure anatomy and to determine if any bright echoes were present across either commissure. High intensity bright echoes extending across the commissure were taken to be areas of commissural calcification. Although by strict terminology the mitral valve has only one commissure between its two leaflets,12 we have followed the common convention of considering that the mitral valve has two commissures: posteromedial and anterolateral. The extent of commissural calcification was quantified by giving each half commissure with such echoes a score of 1. Commissural calcification could therefore range from grade 0 to grade 4 (figs 1 and 2). A grade of 2 could correspond to calcification of one commissure or to calcification of half of both commissures; in 96% of such cases the calcification was localised to one commissure.

Grading system for commissural calcification.

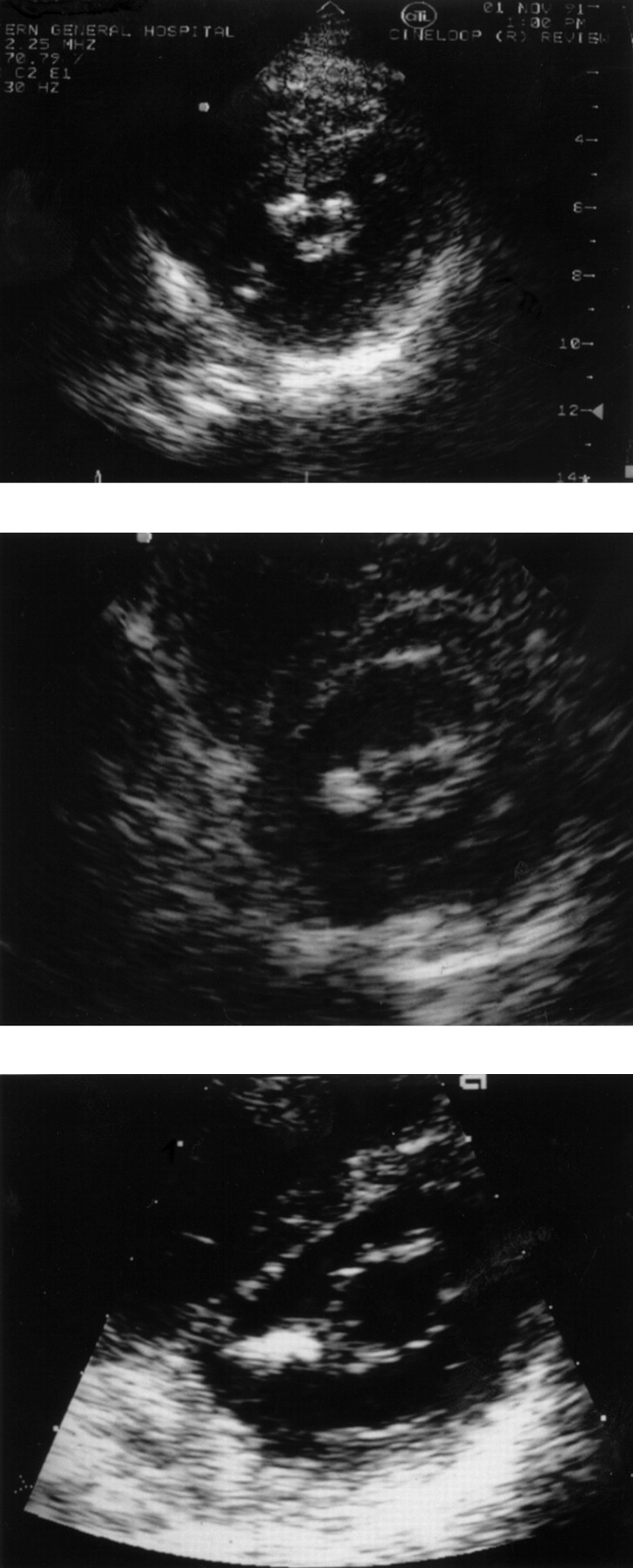
Illustrative examples of commissural calcification. Upper panel: thickening and brightness at leaflet tips but no bright echoes extending across either commissure; grade 0000 = 0. Middle panel: bright echoes extend across half of posteromedial commissure; grade 1000 = 1. Lower panel: postdilatation the anteromedial commissure has opened well but the posteromedial commissure had bright echoes throughout its length and had resisted splitting; grade 1100 = 2.
During the 10 year period, echocardiographic assessment was by consensus of two observers who each performed a transthoracic echocardiogram before the procedure in the final 215 patients and retrospectively from blinded video recordings in the first 85.
TECHNIQUE OF BALLOON VALVOTOMY
The first 70 patients were treated by single or double cylindrical balloons based on the methods described by Lock and colleagues and Al Zaibag and colleagues,15-17 and in the subsequent 230 cases the Inoue balloon was used.18 We found that each technique gave the same increase in valve area.19
Measurement of mitral gradient was by planimetry. Cardiac output was calculated by the Fick principle using assumed oxygen uptake.20 Valve area before and after dilatation was calculated by the Gorlin equation.21 Calculation of valve area after dilatation used oxygen saturations from the venae cavae to avoid any influence of left to right shunting at the atrial puncture site. Mitral reflux was assessed at left ventricular angiography and graded as absent, mild, moderate, or severe.
Inoue balloon size was chosen on the basis of the patient's height.22 The mean effective balloon dilatation area/m2 body surface area23 was 3.41 (0.52).
We used the increase in Gorlin mitral valve area as the measure of haemodynamic improvement because echocardiographic assessment of mitral orifice by planimetry is inaccurate when there is pronounced degenerative change—as was common in our more elderly patients—and Doppler pressure half time is also inaccurate immediately after balloon valvotomy.24 A successful immediate haemodynamic outcome was defined as a final mitral valve area greater than 1.50 cm2 without severe mitral reflux. As patients were referred from a wide geographical area, longer term follow up echocardiograms could not be obtained in all patients; follow up symptom status was obtained by clinic visit or telephone contact.
STATISTICS
Results are expressed as mean (SD). Statistical analysis between groups was by unpaired Student's t test, the χ2 test, and analysis of variance. To identify predictors of a successful haemodynamic outcome, discrete data were compared by χ2 test and continuous data by Student's two tailed t test. A stepwise logistic regression model was used to identify independent predictors of this outcome. A value of p < 0.05 was considered significant.
Results
HAEMODYNAMIC CHANGE
Before balloon dilatation in these 300 patients, the mean (SD) gradient across the mitral valve was 12.8 (5.2) mm Hg, mean cardiac output was 3.65 (1.01) l/min, and mean valve area was 0.91 (0.30) cm2. After final balloon dilatation, the gradient was 5.8 (2.9) mm Hg, cardiac output 4.4 (1.60) l/min, and valve area was 1.74 (0.73) cm2 (all p < 0.001). The mean increase in valve area after balloon dilatation was 0.83 (0.60) cm2. A final valve area above 1.50 cm2without severe mitral reflux was obtained in 173 patients (58%).
ECHO SCORE, COMMISSURAL CALCIFICATION, AND VALVE AREA
The echo score was significantly related to severity of mitral stenosis before dilatation (table 1) but also to the increase in valve area produced by balloon dilatation. The commissure calcification grade was also significantly related to valve area before and after dilatation, but the increase in valve area did not reach significance (table 2).
Relation between the mitral valve area before and after balloon dilatation and the echo score
Relation between the mitral valve area before and after balloon dilatation and the commissure calcification grade
The different types of degenerative mitral valve change tended to develop together. Increasing echo score, reflecting leaflet and subvalvar changes, was significantly associated with increasing commissural calcification (table 3).
Commissural calcification grade in each of four ranges of echo score 3-150
In patients with an echo score of ⩽ 8, a smaller increase in valve area was achieved in those with commissure calcification grade 2/3 than in those with grade 0/1 (table 4). No significant difference was found in patients with an echo score of > 8.
Effect of commissural calcification on increase in mitral valve area in patients with echo score of ⩽ 8 and > 8
The proportions of patients who had a final valve area > 1.50 cm2 are included in table 4. In patients with an echo score of ⩽ 8, 67% of those with commissure calcification grade 0/1 achieved this valve area, compared with only 46% of those with commissure calcification grade 2/3 (p < 0.05).
Echo score had a significant but weak correlation with increase in valve area (fig 3).

{kind=link}
{kind=link}
{kind=link}
Correlation between increase in mitral valve area after balloon dilatation and echo score.
PREDICTORS OF OUTCOME
By univariate analysis, the following patient characteristics were predictive of a final valve area > 1.50 cm2 without severe mitral reflux: younger age, lower commissural calcification grade, lower echo score, less fluoroscopic calcification, lower Parsonnet score (all p < 0.001), sinus rhythm, male sex, and absence of mitral reflux (all p < 0.01). Previous valvotomy, effective balloon dilation area/m2 body surface area, type of balloon, left ventricular impairment, and coronary disease were not significantly related to this outcome.
On multivariate analysis, less fluoroscopic calcification, male sex, sinus rhythm, and lower commissure calcification grade (p < 0.01) were independent predictors of this outcome.
MITRAL REFLUX AFTER FINAL DILATATION
An increase in mitral reflux by two or more grades occurred in 4.1% of patients with commissure calcification grade 2/3 and in 2.8% of those with grade 0/1(NS).
ECHO SCORE, COMMISSURAL CALCIFICATION, AND SYMPTOMATIC IMPROVEMENT
Table 5 shows the NYHA symptom class scores before mitral balloon valvotomy and at follow up 1–3 months later. In patients with an echo score of ⩽ 8, those with commissure calcification grade 0/1 had a significantly greater improvement in symptoms than those with grade 2/3. No difference was seen in those with an echo score of > 8.
Symptom class before mitral balloon valvotomy and alive at 1–3 months follow up in patients with echo score ⩽ 8 and > 8
Discussion
Percutaneous mitral balloon valvotomy has two roles: as an alternative to open or closed surgical valvotomy in patients with a mitral valve judged suitable for commissurotomy, and as a palliative procedure in patients requiring valve replacement but considered to be very high risk surgical candidates. Our series contained many elderly patients and 30% had been judged unsuitable for surgery, so there was a wide spectrum of degenerative mitral valve change. We confirmed the relation between the Massachussets General Hospital echo score and haemodynamic and symptomatic status before and after mitral balloon valvotomy, but the echo score was a weak predictor of increase in valve area in individual cases. In those patients with an echo score of 8 or less, who are generally held to be suitable for balloon valvotomy, we found that commissural calcification had a significant influence on both the increase in mitral valve area and the degree of symptomatic improvement. Assuming that valve replacement is necessary if there is less than a 50% probability of achieving a valve area of more than 1.50 cm2 by balloon dilatation, then commissural calcification occupying the equivalent of one of the two mitral commissures would be an indication for valve replacement rather than for balloon valvotomy. In patients with a low echo score (⩽ 8) and little or no commissural calcification, percutaneous balloon dilatation would be the preferred option when cardiac catheterisation facilities and transseptal puncture skills are available, in view of reduced patient discomfort, short convalescence, and equivalent outcome.2-5
Fatkin and colleagues also found that commissural echo calcification predicted commissural splitting in their group of 30 patients.25 Cannan and colleagues showed that commissural calcium was the only factor significantly affecting clinical outcome after mitral balloon valvotomy in 149 patients.26 In these smaller studies, the extent of commissure calcification was not quantified. Hernandez and colleagues noted that commissural calcium, identified by echocardiography, had been present in patients who developed severe mitral reflux at Inoue mitral balloon valvotomy.27 This could occur if resistance to commissural splitting led to leaflet tear. We found that a pronounced increase in mitral reflux was uncommon, although slightly more frequent in those with pronounced commissural calcification (4.1%v 2.8%). It has been suggested27 that if balloon dilatation is undertaken in a patient with commissural calcification then smaller initial balloon size and a cautious progressive increase in balloon diameter should be used.
In patients with an echo score of > 8, we were not able to show a separate significant effect of commissural calcification on increase in valve area, although the same trend was present. Although such mitral valves are not ideal for a commissurotomy, percutaneous balloon dilatation may be justified if the patient is unsuitable for surgery because of comorbidity. Even limited haemodynamic improvement may give sufficient symptomatic relief to maintain independence.6 ,7
Mitral valve calcification seen at fluoroscopy was also a predictor of outcome. However, fluoroscopy cannot accurately localise the calcific change, and calcification can affect outcome either through leaflet rigidity or commissural resistance. Echocardiography is preferred to localise any mitral calcification to the annulus, the body of the leaflets, or the commissures. This is helpful when there is slight calcification localised at the commissure or, with generalised calcification, when splitting of commissures may give a useful palliative result.
LIMITATIONS OF STUDY
We used transthoracic echocardiography of the mitral valve but in some elderly patients transthoracic imaging is difficult and localisation of calcification may have been imprecise. Very bright echoes may not always correspond to calcification but may reflect dense fibrosis. The consensus grading of commissural calcification involved a variety of observers over a 10 year period.
It would be desirable to improve the echocardiographic predictability of outcome of mitral balloon valvotomy. The echo score is semiquantitative and subjective. In a multicentre registry study, the echo score did not show a significant link with outcome,28but Post and colleagues found that on review of 87 patients initially judged to have an echo score of ⩾ 10, 18 were reclassified as having lower scores when judged by single centre observers.29
CONCLUSIONS
When commissural calcification grade was assessed at transthoracic echocardiography, it was found that calcification equivalent to one commissure was associated with less than a 50% probability of achieving a good haemodynamic outcome. Transoesophageal examination of both commissural calcification and fusion may lead to further improved prediction of outcome by balloon commissurotomy,30particularly in patients who are difficult to scan transthoracically.
Acknowledgments
This study was supported by a grant from the Clinical Resource and Audit Group (CRAG) of the Scottish Office Department of Health. The views expressed are those of the authors and do not necessarily reflect those of either CRAG or the Scottish Office Department of Health.