Article Text

Abstract
OBJECTIVE To identify any potential relations between the size of an emptied plaque cavity and the remodelling pattern, plaque or vessel dimensions, lumen narrowing, and other ultrasonic lesion characteristics.
DESIGN Intravascular ultrasound was used to examine prospectively 51 ruptured ulcerated coronary plaques. Cross sectional area measurements comprised lumen, vessel, plaque, and emptied plaque cavity. Lumen narrowing was calculated as 1 − (lesion lumen area/reference lumen area) × 100%. A remodelling index was calculated as lesion vessel area/reference vessel area, and plaques were divided into those with values > 1.05 (group A) and ⩽ 1.05 (group B).
RESULTS Of the total of 51 plaques, 36 (71%) were assigned to group A and 15 (29%) to group B. In neither group was there a significant difference in reference dimensions and lumen narrowing. However, lesion vessel (mean (SD): 22.6 (8.1) mm2 v 17.5 (4.3) mm2; p = 0.006) and plaque areas (15.8 (6.2) mm2 v 12.8 (3.2) mm2; p = 0.03) were greater in group A than in group B. The cavity inside the plaque was larger in group A than in group B (2.8 (1.6) mm2 v 1.8 (0.9) mm2; p = 0.007) and showed a positive linear relation with lesion and reference vessel size (r = 0.58 and 0.56, respectively; p < 0.001), but not with lumen narrowing.
CONCLUSIONS The size of the emptied cavity inside ruptured plaques is on average larger in lesions with adaptive vascular remodelling, and shows a linear relation with lesion plaque and vessel size and with the reference dimensions, but not with the degree of lumen narrowing.
- intravascular ultrasound
- ultrasonic scanning
- plaque rupture
- remodelling
Statistics from Altmetric.com
Much information about fissuring and disruption of atherosclerotic coronary plaques, the trigger of acute coronary syndromes, has been obtained from necrospy data,1-8 and it has been shown that plaque rupture results in thrombus formation and often in emptying of the atheromatous core. Angiographic techniques provide data on the size and shape of the luminal silhouette in vivo.9 ,10 However, the value of angiography for the assessment of atherosclerosis is limited, as compensatory vascular enlargement may accompany plaque accumulation and partly accommodate the increasing plaque burden,11-13thereby preserving lumen dimensions and causing angiographic underestimation of the underlying atherosclerosis.
Intravascular ultrasound allows transmural visualisation of coronary vessels and has been most useful in confirming the concept of compensatory vascular enlargement in vivo.14-19 Along with its use in assessing vascular remodelling,20-27intravascular ultrasound can also be employed to confirm the presence of plaque rupture in vivo and to measure the size of the emptied plaque cavity (fig 1).28-34 In patients with unstable angina and also in those with plaque rupture documented by intravascular ultrasound, a greater degree of vascular remodelling has been described; this is associated with larger plaque and vessel cross sectional areas.27 ,33 In this study we analysed ruptured plaques using intravascular ultrasound in order to evaluate whether the remodelling pattern, plaque or vessel size, or other ultrasonic lesion characteristics might be related to the size of the cavity inside the ruptured plaque.

Intravascular ultrasound planimetry in ruptured right coronary plaque of a patient in group A (remodelling index > 1.05). Lumen (LU), plaque (PL), plaque cavity (CY), and vessel area (within external contour) were measured in the proximal (A) and distal reference segment (C), and at the lesion site (B). Lesion and mean reference vessel cross sectional area measured 24.4 mm2 and 22.25 mm2, respectively; the remodelling index was 1.09. Plaque cavity cross sectional area measured 4.6 mm2. Lumen area narrowing was 37%.
Methods
PATIENT POPULATION
The study population consisted of 51 patients with ulcerated ruptured plaques confirmed on intravascular ultrasound (lesion type VI-a according to a recently suggested intravascular ultrasound lesion classification19). The lesions were all in previously untreated coronary arteries. This consecutive series of ruptured plaques was identified prospectively from among our patients with unstable angina or with an angiographic picture suspicious of plaque rupture. All plaques included in this study met the following intravascular ultrasound criteria:
high quality images of the lesion as well as of the proximal and distal reference segments;
non-ostial lesion location;
calcification did not limit quantitative assessment of the vessel area;
absence of side branches between the lesion and the proximal and distal reference segments;
absence of very angulated segments on angiography.
The study was approved by the local Council on Human Research, and all patients signed a written informed consent form, approved by the local medical ethics committee.
INTRAVASCULAR ULTRASOUND IMAGING AND INTERVENTIONAL PROCEDURE
All patients were being treated with aspirin and received heparin intravenously before the study. Procedures were performed by the femoral approach, using adequately sized standard 8 F guiding catheters and 0.014 inch (0.36 mm) standard or extra support coronary guide wires.
Intravascular ultrasound imaging was performed before any intervention and after an intracoronary bolus injection of 200 μg of glyceryl trinitrate.
The intravascular ultrasound studies were performed with two commercially available systems. The first system was a mechanical sector scanner (UltraViewTM, Boston Scientific Corporation, San Jose, California, USA) which incorporated 30 MHz single element bevelled transducers. The second system was a solid state device (InVisionTM, Endosonics, Rancho Cordova, California, USA) which used 3.0 F electronic monorail catheters. With both systems, the transducer was withdrawn by use of motorised pullback devices to perform the imaging sequence.34 All transducer pullbacks were started as distal as possible, and the entire artery was imaged to the aorto-ostial junction. In addition, the site of the plaque rupture was examined using manual interrogation. We performed bolus injections of dye and saline to confirm (or exclude) the presence of plaque rupture, as previously described.34 All intravascular ultrasound examinations were recorded on 0.5 inch (1.27 cm) high resolution super VHS tape for off-line analysis. There was no procedural or postprocedural in-hospital complication that could possibly have been related to intravascular ultrasound or to the interventional procedure.
INTRAVASCULAR ULTRASOUND IMAGE ANALYSIS
All intravascular ultrasound runs were analysed by an experienced analyst and overread by two experienced cardiologists. Validation of plaque composition and planimetric measurements of lumen, vessel, and plaque plus media area by intravascular ultrasound have been reported.18 The vessel arearepresents the cross sectional area within the border between the hypoechoic media and the echoreflective adventitia; it was measured by tracing the leading edge of the adventitia—a reproducible measure of the total vessel area. As in many previous intravascular ultrasound studies, plaque plus media area was used as a measure of atherosclerotic plaque, because intravascular ultrasound cannot measure media thickness accurately.15 ,18 ,22 ,23In our laboratory, the intraclass correlation coefficient is 0.99 for repeated measurements of vessel, 0.96 for lumen, 0.95 for plaque cavity, and 0.99 for plaque plus media area.
The area of the cavity inside the plaque (plaque cavity area) was measured as previously described,34 and was added to the plaque plus media area. Accordingly, lesion plaque plus media arearepresents an estimate of plaque area before plaque rupture. The lesion image slice that was analysed had the smallest lumen area.15 ,22 If there were several image slices with an equal lumen area, the one with the largest plaque cavity was analysed. In general, the largest plaque cavity area was observed at (or close to) the slice of the smallest lumen area.
Lesion plaque composition was assessed visually as previously described.18 The total arc of calcium was measured with a protractor centred on the lumen. Thrombus formation was a heterogeneously reflecting plaque with layering,32oscillating or undulating fine speckles within the plaque,18 and a rough intimal surface or a negative imprint of the intravascular ultrasound catheter.29
Reference segments were analysed in a similar way to the lesion. The proximal and distal reference segments were the most normal looking cross sections (smallest plaque plus media) ⩽ 10 mm distal and proximal to the lesion. This method of reference segment selection has been published previously.22 The use of motorised pullbacks helped to limit the axial distance between the lesion and the reference segments. The reference lumen, vessel, and plaque plus media areas reported were the average of the proximal and distal reference.
Lesion lumen area at the minimum lumen site was compared with the reference lumen area; lumen area narrowing was calculated as (1 − (lesion lumen area/reference lumen area)) × 100%. Reduction in the lesion lumen area could theoretically result from plaque plus media increase or vessel area decrease. To study vascular remodelling, we compared the lesion vessel area with the reference vessel area to produce a remodelling index, defined as lesion vessel area/reference vessel area. Based on the value of this index, we divided the plaques into two groups: group A, with values > 1.05, and group B, with values ⩽ 1.05.
STATISTICAL ANALYSIS
Quantitative data are given as mean values (SD). Dichotomous variables are expressed as frequencies; categorical data are compared using χ2 statistics. Continuous variables are compared using the two tailed Student t test and linear regression analysis. Probability values of p < 0.05 are considered significant.
Results
REMODELLING STATE
A remodelling index of > 1.05 was found to be present in 36 (71%) of 51 lesions, which were assigned to group A. The other 15 lesions (29%) had a remodelling index of ⩽ 1.05 (group B).
CLINICAL DATA AND LESION CHARACTERISTICS
Lesions were located in the left anterior descending (n = 23 (45%)), right (n = 24 (47%)), left circumflex (n = 3 (6%)), and left main coronary arteries (n = 1 (2%)), in the proximal (n = 18 (35%)), mid (n = 24 (47%)), and distal segments (n = 9 (18%)). There was a non-significant trend for group A patients to have suffered more often from previous myocardial infarction and to be more likely to have unstable angina (table 1). In groups A and B, lesions were located in the left anterior descending (15/36 (42%) v 8/15 (53%)), right (18/36 (50%) v 6/15 (40%)), left circumflex (2/36 (6%) v 1/15 (7%)), and left main coronary arteries (1/36 (3%) v 0/15 (0%)), in the proximal (13/36 (36%) v 5/15 (33%)), mid (19/36 (53%) v 5/15 (33%)), and distal segments (4/36 (11%) v 5/15 (33%)).
Clinical characteristics of the whole study population and of groups A and B
Predominantly soft plaque composition was found in 33% of all lesions (17 of 51; groups A v B 12/36v 5/15). Some calcium was found in 26 lesions (51%), and the total arc of calcium at lesion site (mean (SD)) was 43 (55)°. Thrombus formation was observed in 15 lesions (29%). There was a trend towards a larger total arc of lesion site calcium in group A than in group B (50 (60)° v 26 (38)°; p = 0.09).
QUANTITATIVE INTRAVASCULAR ULTRASOUND DATA
In group A, the lesion vessel area was larger than the reference vessel area (22.6 (8.1) v 19.3 (6.4) mm2, p < 0.001), while in group B the vessel area at lesion site did not differ significantly from the reference (17.5 (4.3)v 17.9 (4.5) mm2, NS)(table 2).
Quantitative intravascular ultrasound data
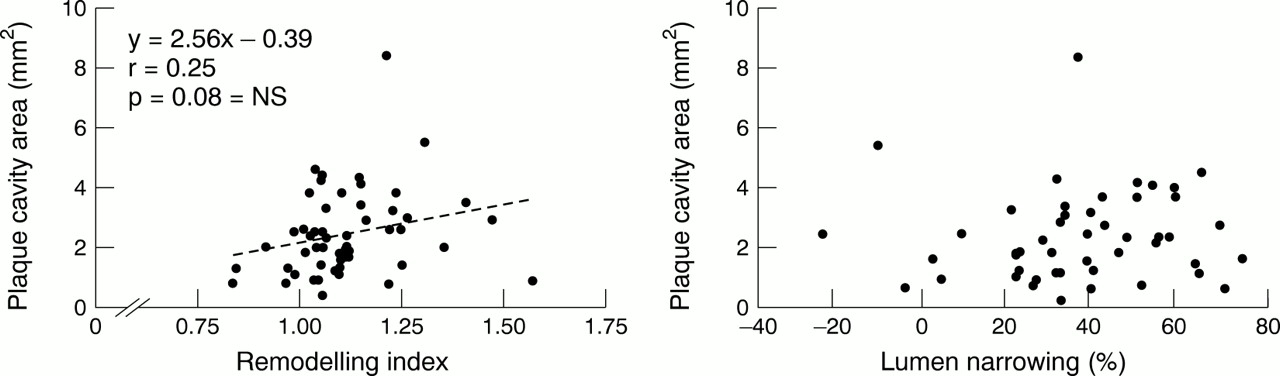
The cavity inside the plaque was larger in group A than in group B (2.8 (1.6) v 1.8 (0.9) mm2; p = 0.007). Examples are given in figs 1 and 2. There were positive linear relations between plaque cavity area and lesion vessel and plaque areas, and between plaque cavity area and reference vessel and lumen areas (fig 3) (r = 0.52–0.58; p < 0.001). There was no significant relation between plaque cavity area and either per cent lumen narrowing or remodelling index (fig 4).

Example of ruptured right coronary plaque from a patient in group B (remodelling index ⩽ 1.05). Lumen (LU), plaque (PL), plaque cavity (CY), and vessel area (within external contour) were measured in the proximal (A) and distal reference segment (C), and at lesion site (B). Remodelling index was 0.97. Lesion and mean reference vessel area measured 15.2 mm2 and 15.7 mm2, respectively. Plaque cavity area was 2.6 mm2 and lumen area narrowing measured 40%. Despite comparable lumen area narrowing in the two examples in figs 1 and 2, plaque cavity area was significantly smaller in the present example, which showed smaller vascular dimensions than the vessel segment of fig1 (note the difference in the 1 mm calibration grid in figs 1 and 2).

Linear regression analyses comparing vascular dimensions with plaque cavity size. The emptied cavity inside the ruptured plaque showed a significant linear relation with lesion plaque and vessel size (upper panels), and with the reference dimensions (lower panels).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison of remodelling index and lumen narrowing with plaque cavity size. The emptied cavity inside the ruptured plaque showed a significant linear relation with lesion plaque and vessel size, and with reference dimensions. There was no significant relation between plaque cavity size and remodelling index (left panel) or the per cent lumen area narrowing (right panel, note scattered distribution of data points).
Discussion
Various studies have shown that ruptured plaques can be detected satisfactorily by intravascular ultrasound.28 ,31 ,33 ,34In the present study, we also evaluated compensatory vascular enlargement (that is, adaptive vascular remodelling), which is the increase in vessel area that occurs to compensate for the increasing plaque burden during the early phase of plaque accumulation. In addition, we measured the size of the cavity inside ruptured ulcerated plaques by intravascular ultrasound and found good agreement with data reported in previous studies.33 ,34
The current in vivo study shows that the size of the emptied plaque cavity following plaque rupture is linearly related to the absolute lesion plaque and vessel dimensions, and to the reference dimensions. In addition, plaque cavity size was larger in the lesions in group A (with a remodelling index > 1.05), which were present in 71% of the patients. However, neither lumen narrowing nor remodelling index showed a direct relation with plaque cavity size; thus these variables do not allow one to identify plaques at increased risk ofmassive atheroma embolisation in the case of plaque rupture with ulceration.
The larger mean plaque cavity size in group A lesions can easily be explained by the relatively larger lesion plaque and vessel dimensions in cases of greater adaptive remodelling. However, a linear relation between plaque cavity size and remodelling index was not found and should not be expected. Adaptive remodelling with higher compensatory vascular enlargement is associated withrelatively larger plaque and vessel dimensions at the lesion site, but this remodelling pattern can be found in vascular segments of any (reference) size, which renders a linear relation with plaque cavity size improbable.
INSIGHTS PROVIDED BY NECROPSY STUDIES
Previous necropsy studies have underlined the importance of plaque size in the development of a large atheromatous core and plaque rupture, suggesting that plaque rupture with thrombus formation is mostly associated with significant plaque burden.1 ,4 ,6Most pathoanatomical studies have suggested that the atheromatous core enlarges with plaque growth.33-37 However, comparison of plaque size and core size of mostly non-ruptured plaques showed no linear relation.8 Our observation in the present study that the cavity inside the plaque showed no relation to percentage lumen narrowing corroborates previous angiographic data and pathoanatomical findings.8 ,9
Rupture and ulceration of lesions with large vessel dimensions and a marked atheromatous core may be followed by embolisation ofmore atheromatous material, leading to microinfarction, exposure of more thrombogenic tissue,6and (most probably) a worse clinical outcome. This may partly explain the high representation of plaques with large plaque burden that was described in previous studies on patients withfatal plaque rupture.1 ,4 ,6Conversely, intravascular ultrasound studies in vivo imply the assessment of survivors of the event. Therefore, histological and intravascular ultrasound studies may be complementary in improving our understanding of coronary atherosclerosis, acute coronary syndromes, and plaque rupture.
PREVIOUS INTRAVASCULAR ULTRASOUND STUDIES
Adaptive remodelling with compensatory vascular enlargement was previously identified as the predominant remodelling pattern of unstable or ruptured plaques.26 ,27 ,33 Gyöngyösiet al reported adaptive remodelling in unstable patients in no more than 37% of all plaques,27while adaptive remodelling was found in 16 of 26 ruptured plaques (62%). Moriuchi et al observed compensatory vascular enlargement in 11 of 22 ruptured plaques (50%).33
LIMITATIONS AND POTENTIAL SOURCES OF ERROR
As with all histological and most intravascular ultrasound studies, our study provides only a snapshot view of coronary artery disease, and because ostial and extremely calcified plaques were not included, our findings may not be applicable to these lesions. Visual assessment of plaque composition is limited, and ultrasonic tissue classification does not necessarily correspond to histology. Remodelling of the reference segments may affect assessment of lesion site remodelling. We may also have missed some ruptured plaques in which the cavity was extremely small, filled by thrombus, or sealed by reattachment of the flap. In addition, angiographic suspicion of plaque rupture may have triggered intravascular ultrasound examination in several cases. Accordingly, we cannot exclude a certain selection bias towards larger plaque cavities in this population. Finally, plaque rupture may lead to haemorrhage and thrombus formation, which could alter plaque geometry and the remodelling pattern. However, observation of a predominance of greater compensatory vascular enlargement in ruptured plaques in vivo is supported by the in vitro data of Pasterkamp et al,38 who found an association between histopathological markers of plaque vulnerability and adaptive remodelling in plaques that had not undergone plaque rupture.
CONCLUSIONS
The size of the emptied cavity inside the ruptured plaque is on average larger in lesions with adaptive vascular remodelling, and shows a linear relation with lesion plaque and vessel size and with reference dimensions, but not with the degree of lumen narrowing.
Acknowledgments
This project was supported by a grant of the German Research Society, DFG, Bonn, Germany (DFG 155 4–1).