Article Text

Abstract
OBJECTIVE To clarify whether assessment of the acoustic properties of the myocardium at rest can predict contractile reserve in patients with chronic left ventricular dysfunction.
METHODS 23 patients (mean (SD) age 63 (12) years) with chronic left ventricular dysfunction were studied. The magnitude of cardiac cycle dependent variation of integrated backscatter (CVIB) of the myocardium was measured at rest in the basal and mid segment of the septum and posterior wall of the left ventricle, using a real time two dimensional integrated backscatter imaging system. The results were compared with the percentage wall thickening and the wall motion at rest and during low dose dobutamine infusion. The wall motion was graded as normal, hypokinetic, or akinetic and contractile reserve was considered present when an akinetic or hypokinetic segment improved during dobutamine infusion.
RESULTS The CVIB at rest correlated with per cent wall thickening at rest and during dobutamine infusion (at rest, r = 0.61, p < 0.0001, during dobutamine, r = 0.76, p < 0.0001). Of the 76 segments examined, 27 showed contractile reserve. The mean CVIB at rest was significantly greater in segments with contractile reserve than in those without (p < 0.0001). CVIB above 3 dB at rest predicted segments with contractile reserve with a sensitivity and specificity of 81% and 60%, respectively (p < 0.0001).
CONCLUSIONS CVIB reflected not only myocardial contractility but also the functional capacity of the myocardium. It predicted segmental contractile reserve in patients with chronic left ventricular dysfunction.
- contractile reserve
- acoustic properties of myocardium
- cyclic variation of integrated backscatter
- left ventricular dysfunction
Statistics from Altmetric.com
- contractile reserve
- acoustic properties of myocardium
- cyclic variation of integrated backscatter
- left ventricular dysfunction
Contractile reserve is the potential of ventricular segments that contract abnormally in the basal state to show augmented contractility with pharmacological or mechanical interventions. The prediction of contractile reserve in dysfunctional myocardium has therapeutic and prognostic implications.1-5 Although dobutamine induced systolic wall thickening assessed by echocardiography has proved reliable for evaluating regional contractile reserve,6-8it is time consuming and relatively invasive. Ultrasonic tissue characterisation by integrated backscatter is a time saving and non-invasive approach for determining the static and dynamic properties of the myocardium. Normal myocardium shows cardiac cycle dependent variation of integrated backscatter (CVIB). CVIB reflects regional and intramural contractile performance, and its magnitude is decreased in both ischaemic9-15 and non-ischaemic16-20myocardial disease. Studies have shown that the magnitude of CVIB is preserved in segments with functional recovery after myocardial ischaemia,11 ,21-24 and that it predicts contractile reserve in ischaemic myocardial damage.10 ,11 We hypothesised that myocardial segments with preserved CVIB in patients with chronic left ventricular dysfunction might show contractile reserve. The purpose of this study was to determine whether assessment of the acoustic properties of the myocardium at rest can predict contractile reserve in patients with chronic left ventricular dysfunction.
Methods
STUDY POPULATION
Twenty six consecutive patients with chronic left ventricular dysfunction were considered for inclusion in the study, but three were excluded because of inadequate echocardiographic image quality, where the endocardial border was not identified clearly by the conventional echocardiograms. The study group thus included 23 patients (nine women and 14 men) with a mean (SD) age of 63 (12) years (range 37–85 years). The diagnosis of left ventricular dysfunction was based on dilatation of the left ventricle (end diastolic dimension over 60 mm) and a low ejection fraction (< 35%). We did not exclude patients with coronary artery disease, hypertension, or diabetes. Coronary angiography was performed in 20 patients. The depressed left ventricular function was attributed to coronary artery disease in 13 patients, to idiopathic cardiomyopathy in eight, and to hypertension in two (table 1). All patients gave written informed consent for participation in the study.
Patient characteristics
CONVENTIONAL ECHOCARDIOGRAPHY
Conventional cross sectional echocardiography was performed in the standard manner. The end diastolic and end systolic wall thicknesses were measured from the cross sectional images. The percentage wall thickening (%WT) was calculated as follows: %WT = [(end systolic thickness − end diastolic thickness)/end diastolic thickness] × 100 (%).
The volume of the left ventricle was calculated by the biplane modified Simpson's method, and the ejection fraction from the standard formula. Wall motion was scored as normal, hypokinetic, or akinetic for each segment, both at rest and during dobutamine infusion. Contractile reserve was considered present when an akinetic or hypokinetic segment improved by more than one grade from rest during dobutamine infusion. All tomograms were analysed on a segmental basis by two experienced observers who did not know the results of the integrated backscatter analysis. In case of disagreement over segmental grade, a third observer reviewed the study and the subsequent majority judgment was binding.
INTEGRATED BACKSCATTER IMAGES
Integrated backscatter images were obtained using a real time two dimensional ultrasonic backscatter imaging device (Sonos 5500, Hewlett-Packard Co, Andover, Massachusetts, USA) equipped with an acoustic densitometry measurement package for the analysis of backscatter signals. This system allows the operator to acquire and store a sequence of continuous two dimensional integrated backscatter images on an optical disk for subsequent analysis. Off-line analysis of the backscatter images was performed by retrieving the previously stored real time cine loop data from the system's built in optical disc drive. The integrated backscatter was measured from the cine loop of the parasternal long axis view of the left ventricle (fig 1). We attempted multiple segmental analysis. An elliptical region of interest, of 31 × 31 or 41 × 41 pixels, was placed in either the mid or the basal anterior septum or in those portions of the posterior wall of the left ventricle. Thus regions of interest were placed in a maximum of four segments for each patient. We chose the largest region of interest that covered the myocardium while avoiding the specular echoes from the endocardium or epicardium. After the initial adjustment, an acquisition test was made to guide the adjustments of the transmitting and gain controls to ensure that the radio frequency signal of the myocardium was neither saturated nor below noise level. All controls were held constant during the studies in each subject after the adjustment. The magnitude of CVIB was calculated as the difference between the minimum and maximum values in a cardiac cycle averaged for at least two consecutive beats.
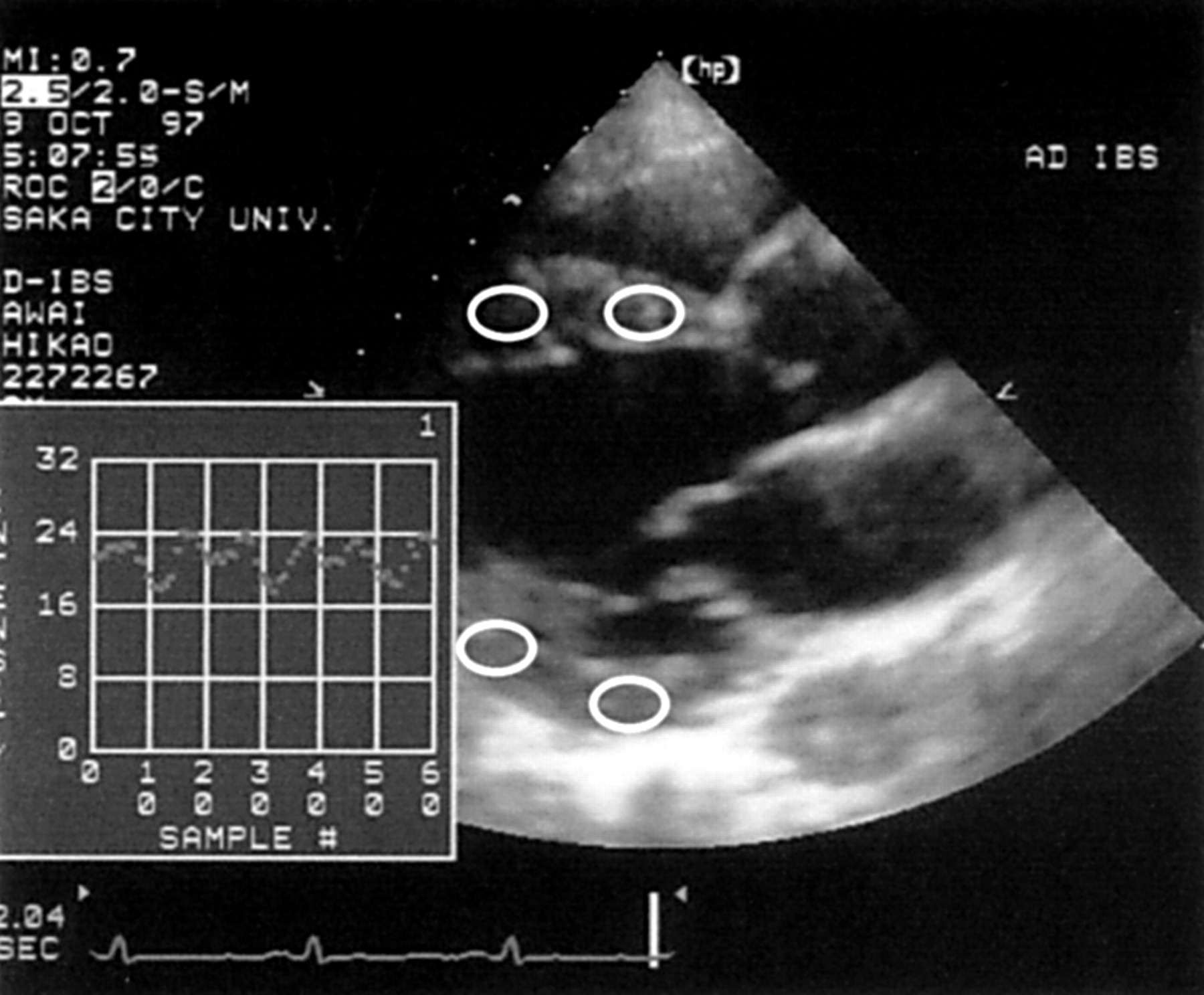
Two dimensional (cross sectional) integrated backscatter imaging interfaced with acoustic densitometry. Parasternal long axis integrated backscatter images were stored in digital format. An elliptical region of interest was placed in the mid myocardium of the mid or basal myocardial segment of the interventricular septum and posterior wall.
We also calculated the time delay of CVIB, which was defined as the interval between the onset of the R wave on the ECG to the nadir of the integrated backscatter curve divided by the QT interval. Both these intervals were measured from the same cine loop. Because each stored cine loop consisted of 60 frames from consecutive cardiac cycles (30 frames/s), the time delay of CVIB could be obtained from the same cardiac cycle by determining the ratio of frame numbers from the R wave to the nadir of the integrated backscatter curve, and that from the Q wave to end of the T wave of the ECG. If the end of the T wave could not be identified, the QT interval was measured from a 12 lead ECG. We used the phase corrected magnitude reported by Takiuchi and colleagues,12 which was an approximation of the phase weighted amplitude.13 ,21 In summary, if the time delay of CVIB was < 1.2 (mean + 2 SD of normal), the magnitude of CVIB was multiplied by 1.0, while if the time delay was > 1.2, the magnitude of CVIB was multiplied by −1.0.
DOBUTAMINE STRESS ECHOCARDIOGRAPHY
After conventional and integrated backscatter echocardiographic images were obtained, dobutamine was given intravenously at doses of 5 and 10 μg/min for five minutes each, with continuous lead II ECG monitoring. Digitised echocardiographic recordings were obtained at the end of each stage. A 12 lead ECG and blood pressure were monitored at every stage. Images were obtained digitally from parasternal long, short axis, and apical four and two chamber views and stored in cine loop format. The per cent wall thickening of each segment was determined at each stage of dobutamine infusion from the parasternal long axis images.
REPRODUCIBILITY OF DATA
Intraobserver and interobserver variability of the magnitude of CVIB was assessed by measuring the magnitude of CVIB in 10 randomly selected subjects twice by the same observer and also by two independent observers. The mean (SD) absolute differences in the magnitude of CVIB were 0.2 (0.3) dB (intraobserver) and 0.3 (0.4) dB (interobserver).
STATISTICAL ANALYSIS
All values are expressed as mean (SD). The per cent wall thickening values at rest were compared with those during dobutamine infusion in the same segment using a pairedt test. Variables for different groups were compared by means of the Wilcoxon non-parametric test. The relations between variables of two groups were studied by simple linear regression analysis. Analysis of categorical variables was performed using Fisher's exact test and the χ2 test. Sensitivity, specificity, and positive and negative predictive accuracies were calculated by the standard formulas. Significance was established at p < 0.05.
Results
CONVENTIONAL AND DOBUTAMINE STRESS ECHOCARDIOGRAPHY
The mean (SD) per cent wall thickening increased significantly during dobutamine infusion (19 (17)% at restv 32 (22)% during dobutamine, p < 0.0001). There was a significant correlation between per cent wall thickening at rest and during dobutamine infusion (r = 0.61, p = 0.0001). Of 92 segments (four in each patient), 16 were excluded from analysis because of inadequate image quality. Of the 76 segments analysed, 14 were scored at rest as akinetic, 56 as hypokinetic, and six as normal. Of the 70 akinetic or hypokinetic segments at rest, three akinetic segments changed to hypokinetic, and two akinetic and 22 hypokinetic segments changed to normal during dobutamine infusion. In all, 27 segments (38.6%) were judged to have contractile reserve. There was a weak but significant difference in per cent wall thickening at rest between segments with and without contractile reserve (p < 0.05, fig2).

Individual values of per cent wall thickening (%WT) (A) and magnitude of cardiac cycle dependent variation of integrated backscatter of the myocardium (CVIB) (B) for segments with contractile reserve (CR+) and those without (CR−). There was a weak but significant difference in %WT at rest between segments with and without contractile reserve. The magnitude of CVIB was significantly greater in segments with contractile reserve that in those without.
INTEGRATED BACKSCATTER IMAGES
We attempted multiple segmental analysis of integrated backscatter from one cine loop, and a reproducible integrated backscatter curve was obtained in 76 segments (83%).
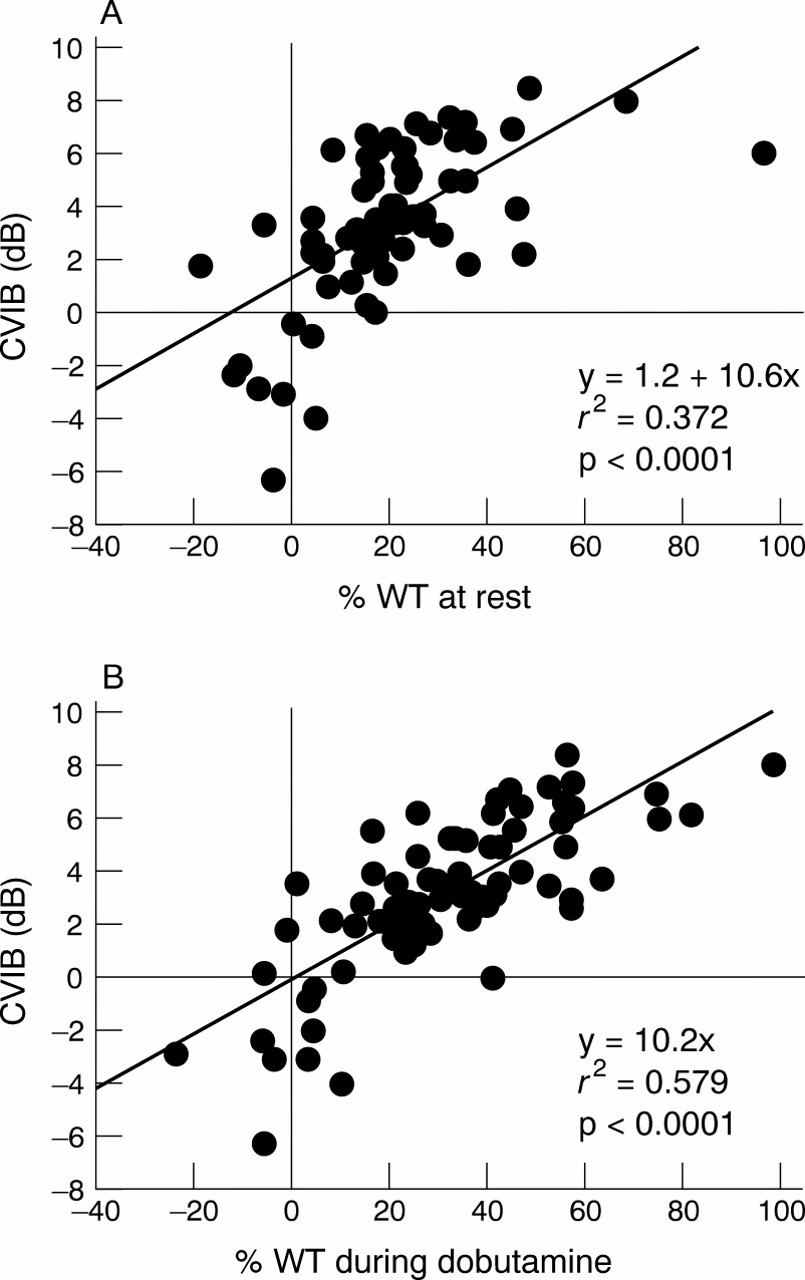
The magnitude of CVIB at rest correlated with per cent wall thickening at rest and during dobutamine infusion (at rest,r = 0.61, p < 0.0001; during dobutamine, r = 0.75, p < 0.0001, fig3). The magnitude of CVIB at rest was significantly greater in segments with contractile reserve than in those without (95% confidence interval (CI) 4.01 to 5.59 dB in segments with contractile reservev 0.97 to 2.72 dB in segments without contractile reserve, p < 0.0001 (fig 2B)). Figure 4 shows representative backscatter curves for a segment with contractile reserve and a segment without contractile reserve. The potential of CVIB magnitude for predicting contractile reserve in akinetic or hypokinetic segments was assessed, and CVIB of 3 dB was considered the optimum cut off point for predicting contractile reserve. A CVIB of 3 dB at rest predicted contractile reserve with a sensitivity of 81%, a specificity of 61%, and positive and negative predictive accuracies of 56% and 84%, respectively (p < 0.001).

Scatterplot showing the correlation between the magnitude of cardiac cycle dependent variation of integrated backscatter at rest and systolic wall thickening at rest (A) and that during dobutamine infusion (B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Representative curves of cyclic variation of integrated backscatter in a segment with contractile reserve (A) and a segment without contractile reserve (B). Cyclic variation shows a synchronous pattern in the segment with contractile reserve, but an asynchronous pattern in the segment without.
Discussion
The results of this study showed first, that the magnitude of CVIB at rest correlated with myocardial contractile potential as well as with myocardial contractility, and second, that the magnitude of CVIB at rest predicted segments with contractile reserve in patients with chronic left ventricular dysfunction.
CARDIAC CYCLIC DEPENDENT VARIATION OF INTEGRATED BACKSCATTER AND WALL THICKENING
Previous studies have shown that CVIB reflects the physical properties of the myocardium. The dependence of CVIB on myocardial contractile performance has been documented in both animals and humans.16 ,25-29 Many studies have shown that the magnitude of CVIB depends on segmental contractility and is decreased in hypokinetic regions in both ischaemic30 and non-ischaemic myocardial diseases.17 ,20 However, it has also been shown that CVIB does not depend entirely on segmental contractility in either ischaemic or non-ischaemic myocardial dysfunction.9 ,24-27 ,29 ,31 ,32 In ischaemic heart disease, regions of severe hypokinetic or akinetic segments in acute myocardial infarction may show recovery of CVIB after coronary recanalisation.9 ,12 ,16 ,24-26 ,28 ,32 In non-ischaemic heart disease, a transient reduction in CVIB accompanies rejection of cardiac allografts and recovers following intensive antirejection treatment.18 These observations indicate that CVIB reflects the functional potential as well as the contractility of the myocardium.
In this study, the magnitude of CVIB was correlated with per cent wall thickening both at rest and during dobutamine infusion. Our results indicate that CVIB provides information not only about contractility at rest but also about the functional capacity of the myocardium—that is, contractile reserve. Several mechanisms might explain why CVIB predicts the contractile reserve of the chronically dysfunctional myocardium. First, the functional muscle is mixed with fibrosis or non-viable muscle in this situation. Contraction of the functional muscle is therefore not strong enough to obtain observable segmental contraction. Second, some dysfunctional segments contract isometrically or asymmetrically against an excessive afterload. In such conditions, the myocardium fails to contract transmurally. However, the myocardium in these conditions can show CVIB. Dobutamine makes the segmental myocardial contraction stronger, a change detectable by conventional echocardiography regardless of the cause of dysfunction.
CONTRACTILE RESERVE AND DYSFUNCTIONAL MYOCARDIUM
Contractile reserve has important clinical implications regarding chronic left ventricular dysfunction in patients with both ischaemic and non-ischaemic myocardial damage. In patients with impaired left ventricular function, reliable distinction of potentially salvageable myocardium from irreversibly damaged scar tissue is of major clinical importance. The presence of contractile reserve indicates preserved myocardial perfusion and functional recovery after revascularisation in chronic ischaemic left ventricular dysfunction,1 ,6 ,8 ,33and is also associated with a good prognosis in non-ischaemic left ventricular dysfunction.4 ,5 Many hypokinetic and even akinetic areas of ventricular wall contain ischaemic though viable muscle, non-ischaemic viable muscle, and fibrous scar. The viable muscle is capable of responding to inotropic stimulation, while necrotic tissue obviously cannot be stimulated to contract by any pharmacological or haemodynamic intervention.
Methods for assessing the contractile reserve of the potentially viable myocardium include the use of postextrasystolic potentiation during left ventricular angiography,34 the response of left ventricular contraction to an inotropic stimulus such as dobutamine,1 ,6-8 ,14 evidence of uptake of thallium-201 in a dysfunctional region of myocardium,3 ,8 and positron emission tomography, which demonstrates glucose utilisation by the myocardium.3 ,7 We employed low dose dobutamine infusion to evaluate contractile reserve because it is clinically well tolerated.
REAL TIME TWO DIMENSIONAL INTEGRATED BACKSCATTER IMAGE
Conventionally, integrated backscatter analysis of the myocardium is performed by the M mode integrated backscatter technique, which yields segmental ultrasonic characteristics of the myocardium. The real time two dimensional integrated backscatter device enables us to analyse multiple segments simultaneously. Although this technique has been validated29 and many studies using it have been reported, there are few reports in which multiple segmental integrated backscatter analysis was attempted.35 Real time, two dimensional integrated backscatter images also have an advantage over M mode images because the M mode technique does not permit perfect geometric localisation of structures, and the two dimensional approach provides for spatial averaging during examination. In this study, we could obtain a reproducible integrated backscatter curve for more than 80% of segments. This approach is promising for assessing myocardial tissue in various clinical settings.
LIMITATIONS OF THE STUDY
There was considerable overlap in CVIB at rest between segments with contractile reserve and those without. This overlap made it difficult to predict contractile reserve within individual patients. There are several possible explanations for the low specificity observed in this study. One is downregulation of β receptors in chronic myocardial dysfunction. In the failing myocardium, there is a blunted myocardial response which is increasingly reduced as heart failure progresses.36 ,37 Therefore the use of a larger dose of dobutamine could have improved the specificity of our study. Another possibility is heterogeneity of myocardial contraction. In normal myocardium, subendocardial thickening is greater than subepicardial thickening and CVIB is greater in the subendocardial layer than in the subepicardial layer. In acute myocardial ischaemia, CVIB decreases in the subendocardial layer but not in the subepicardial layer, even when transmural wall thickening decreases.14Therefore, if there is much more damage in the subendocardial layer than in the subepicardial layer in the chronically injured myocardium, a discrepancy may occur between preserved CVIB and decreased wall thickening. In this study, we did not measure an intramural gradient of CVIB because this requires a high image quality such as can be obtained with a transoesophageal approach or by using a zoom function. These explanations could mean that preserved CVIB represents myocardial viability rather than contractile reserve. This is crucial not only for the assessment of myocardial viability and contractile reserve but also for therapeutic intervention for patients with chronic left ventricular function.
CVIB could be obtained only from the anterior septum and posterior wall, because it is strongly dependent on fibre orientation and anisotropism of the myocardium.38 ,39 Though the real time two dimensional integrated backscatter imaging technique cannot overcome this limitation, it allows placement of multiple regions of interest to the extent that fibre orientation is adequate, and this yields much more information than the M mode technique. In this study, we attempted multiple segmental integrated backscatter analysis by using the real time two dimensional integrated backscatter imaging device, and over 80% of segments could be analysed and compared with segmental wall thickening.
The number of patients was small so that the statistical power was low in distinguishing those segments with contractile reserve from those without, and also there was insufficient statistical power to predict prognosis. Further studies are needed.
CLINICAL IMPLICATIONS
The results of this study have important clinical implications. Dobutamine stimulation or other semi-invasive techniques have hitherto been required to evaluate contractile reserve. Integrated backscatter images can be obtained completely non-invasively, and analysis of CVIB can add quantitative and qualitative information on myocardial contractile reserve. This method will be helpful in performing medical or surgical interventions, such as revascularisation or transplantation, for chronic myocardial dysfunction. It will also be convenient for the clinical follow up of patients with chronic left ventricular dysfunction.
CONCLUSIONS
The magnitude of CVIB at rest correlated not only with percentage wall thickening at rest but also with that during low dose dobutamine infusion, and it predicted contractile reserve in patients with chronic left ventricular dysfunction. These findings suggest that tissue characterisation with integrated backscatter is useful for detecting functional myocardium in these patients.