Article Text

Abstract
OBJECTIVES To quantify the short term haemodynamic effects of biventricular pacing in patients with heart failure and left bundle branch block by using three dimensional echocardiography.
DESIGN Three dimensional echocardiography was performed in 15 consecutive heart failure patients (New York Heart Association functional class III or IV) with an implanted biventricular pacing system. Six minute walk tests were performed to investigate the effect of biventricular pacing on exercise capacity. Data were acquired at sinus rhythm and after short term (2–7 days) biventricular pacing.
RESULTS Compared with baseline values, biventricular pacing significantly reduced left ventricular end diastolic volume (EDV) by mean (SD) 4.0 (5.1)% (p < 0.01) and end systolic volume (ESV) by 5.6 (6.4)% (p < 0.02). Mitral regurgitant fraction was significantly reduced by 11 (12.1)% (p < 0.003) and forward stroke volume (FSV) increased by 13.9 (18.6)% (p < 0.02). Exercise capacity was significantly improved with biventricular pacing by 48.4 (43.3)% (p < 0.00001). Regression analyses showed that the percentage increase in FSV independently predicted percentage improvement in walking distance (r 2 = 0.73, p < 0.0002). Both basal QRS duration and QRS narrowing predicted pacing efficacy, showing a significant correlation with %ΔEDV, %ΔESV, and %ΔFSV.
CONCLUSIONS In five of 15 consecutive patients with heart failure and left bundle branch block, biventricular pacing induced a more than 15% increase in FSV, which predicted a more than 25% increase in walking distance and was accompanied by an immediate reduction in left ventricular chamber size and mitral regurgitation.
- heart failure
- left ventricular volume
- pacing
- three dimensional echocardiography
Statistics from Altmetric.com
Pacing as an adjunctive treatment in selected patients with severe heart failure and left bundle branch block is being investigated in clinical trials. Initial research was focused on dual chamber pacing with shortening of the atrioventricular interval to optimise ventricular filling and limit presystolic mitral regurgitation.1-3 More recently, simultaneous biventricular pacing to restore systolic contractile synchrony has been investigated. Thus, in heart failure patients both biventricular and single site left ventricular (LV) free wall pacing have been shown to enhance femoral systolic pressure acutely while lowering pulmonary wedge pressure and V wave amplitude.4 Similar results have been reported by other investigators showing significantly increased cardiac index and decreased pulmonary wedge pressure.5 In addition, pressure–volume analysis revealed that biventricular pacing acutely enhanced contractile function in heart failure patients with intraventricular conduction delay.6 Thus, improved contractile function, reduced mitral regurgitation, and optimised LV filling have all been proposed as beneficial effects of biventricular pacing. However, the relative importance of the proposed mechanisms is unclear and a direct correlation to the patient's clinical status is missing. Thus, a non-invasive protocol is needed to evaluate pacing related haemodynamic changes outside the catheterisation laboratory. Recent advances in three dimensional (3D) echocardiography using tissue harmonic imaging allow us to measure LV volumes with excellent reproducibility.7 In addition, a novel 3D colour Doppler technique has been shown to quantify volumetric flow in the large vessels accurately.8-11 No previous study has quantified the impact of biventricular pacing on forward stroke volume and mitral regurgitation or the possible changes in LV chamber size. Neither have pacing induced haemodynamic changes been correlated directly with exercise capacity. To address these issues, we performed a 3D echocardiographic study of short term biventricular pacing effects in patients with dilated cardiomyopathy. We investigated the following hypotheses: firstly, that biventricular pacing reduces functional systolic mitral regurgitation and increases cardiac output in patients with heart failure; secondly, that LV volumes are reduced because of electrical cardiac resynchronisation; and lastly, that a favourable haemodynamic response to biventricular pacing is reflected by improved exercise capacity in patients with dilated cardiomyopathy.
Methods
STUDY GROUP
Fifteen consecutive male patients in sinus rhythm with bundle branch block (QRS duration > 120 ms measured as the maximum width from a 12 lead surface ECG with a paper speed of 50 mm/s) and severe heart failure symptoms (New York Heart Association functional class III or IV) despite contemporary medical treatment were enrolled in the study. The study protocol included pacemaker implantation and 3D echocardiographic examination. Written informed consent was obtained from each patient in accordance with the regional ethical committee on human research. Patients were all in a stable haemodynamic condition at the time of their inclusion into the study. The anticongestive medication consisted of diuretics, angiotensin converting enzyme inhibitors, β blockers, digoxin, and aldosterone antagonist. Table 1provides baseline clinical characteristics.
Baseline clinical characteristics of patient group
PACING PROTOCOL
All patients had a permanent left sided biventricular pacemaker system implanted. Using either subclavian vein puncture or cephalic vein putdown, three transvenous pacing leads were implanted, one in the high right atrium, one in the septal region of the right ventricle, and one in the coronary sinus system (left ventricle). Active fixation leads (Sweet Picotip, CPI, St Paul, Minnesota, USA) were used for the right atrium and right ventricle. To pace the left ventricle, either a standard pacing lead (Slimtine, Vitatron, Dieren, The Netherlands) or a specially designed coronary sinus lead (2187 or 10512, Medtronic, Minneapolis, Minnesota, USA) was guided into the coronary sinus system. The tip electrode was then placed in a stable position in a side branch, preferably in the middle part of the lateral or posterolateral region.
For optimal LV resynchronisation during biventricular pacing, the right ventricular and LV pacing leads were placed so that the sensed local intracardiac activation during sinus rhythm was measured as early as possible for the right ventricular lead and as late as possible for the LV lead.5 Thereby the widest possible electrical and anatomical separation was obtained between the two ventricular pacing leads, ensuring maximal “normalisation” of QRS duration on surface ECG during biventricular pacing.
The pacing leads were connected to a dual chamber biventricular pacemaker (InSync, Medtronic) with simultaneous pacing of the two ventricular leads. The biventricular pacemaker was programmed in DDD mode and for each patient the atrioventricular interval was adjusted to maximise mitral inflow duration with the aid of pulsed Doppler recordings. Atrial rates were kept at identical values during the comparative 3D echocardiographic measurements with and without biventricular pacing.
ECHOCARDIOGRAPHIC PROTOCOL
Ten of the 15 subjects underwent measurement of LV volumes and volumetric flows by 3D echocardiography on the day before pacemaker implantation and 2–7 days (mean 2.9 days) afterwards. Five of the patients were investigated on the day after implantation with biventricular pacing on and off. These measurements were first taken with biventricular pacing on and then repeated after pacing had been off for approximately half an hour.
Transthoracic 3D echocardiography was performed with the subjects in the left lateral decubitus position (Vingmed SystemFive, GE Vingmed Ultrasound, Horten, Norway). LV volumes and volumetric flows through the LV outflow tract and mitral valve were acquired by coaxial (rotational) scanning from an apical position.12 The initial apical image of the LV long axis was selected arbitrarily to ensure absence of sampling bias, and six sections were acquired with a 30° interval by automated rotation of the transducer. LV volume recordings were made in tissue harmonic mode to improve endocardial border detection using a transducer frequency of 1.6 or 1.7 MHz, depending on the acoustic properties of the subjects.
Volumetric flows through the LV outflow tract and mitral valve were measured by 3D colour Doppler by rotational data acquisition similar to the LV volume measurements. The colour flow data were recorded at 2.5 MHZ and low velocity rejection was set to 12 cm/s. The aliasing velocity was 66–74 cm/s. In these settings the acquisition rate was 21–30 frames/s.
A hand held rotation device (GE Vingmed Ultrasound) that was triggered by the R wave of the ECG rotated the transducer. To exclude cardiac arrhythmia, only heart cycles with a cycle length within ±20% of the mean were accepted. The cardiac images were recorded during end expiratory apnoea within one breath hold, thereby abolishing the need for respiratory triggering. The six two dimensional images together with the ECG were stored in one cine-loop and then digitised and transferred on line to a computer (Apple, Cupertino, USA) for later data analysis. Total examination time including data storage was approximately 10–15 minutes depending on the acoustic window of the subject.
ECHOCARDIOGRAPHIC DATA ANALYSIS
One of the authors (WYK) performed the entire echocardiographic analysis to reduce observer variation. This observer was blinded to the results of the exercise test and was unaware of any changes in the patient's symptoms at the time of analysis.
LV VOLUME ANALYSIS
The LV endocardial contours were drawn manually. In defining the endocardium, the papillary muscles were included in the LV volume to standardise measurements. The image at the beginning of the QRS of the ECG was defined as end diastole while the smallest area just before mitral valve opening was defined as end systole. Total LV volume was calculated from all six sections according to a volume estimation algorithm based on calculation of reconstructed polyhedrons—a set of polygons (usually triangles) that describe the object.13The end diastolic (EDV) and end systolic (ESV) volumes were tabulated from the analysis and the ejection fraction (EF) was calculated as follows: EF = ((EDV − ESV)/EDV) × 100% [equation 1].
The average of the two repeated recordings of EDV, ESV, and EF were tabulated. The analysis time for each LV volume was 4–5 minutes.
VOLUMETRIC FLOW ANALYSIS
The digitised colour Doppler flow maps were analysed with a dedicated software program. Stroke volumes (SVs) through the mitral valve (total SV) and LV outflow tract (forward SV) were calculated by integrating spatial and temporal colour flow velocity data. By integration of velocity vectors across a spherical surface, which is normal to the point of scanning, volumetric flow can be measured independently of the angle between the ultrasonic beam and the blood flow. In addition, phasic variations in the cross sectional flow area are included by summation of each colour Doppler frame. A detailed description of the 3D colour Doppler technique is provided elsewhere.9 ,10 The mitral regurgitant fraction was calculated as follows: regurgitant fraction = ((total SV − forward SV)/total SV) × 100% [equation 2].
To characterise the mitral inflow waveform, the atrial systolic (A wave) contribution to mitral inflow was calculated as the ratio of the A wave time–velocity integral (ATVI) to the total diastolic time–velocity integral (TotalTVI). Thus, the atrial systolic contribution to mitral inflow was determined as ATVI/TotalTVI.
EXERCISE PROTOCOL
A six minute walk test was performed on the day before pacemaker implantation and 2–7 days after implantation to evaluate the effect of biventricular pacing on exercise capacity. Patients were instructed to walk down a corridor at their own pace, attempting to cover as much ground as possible in six minutes. The total walking distance was recorded.
STATISTICAL ANALYSIS
Paired Student's t test was used to compare haemodynamic parameters measured by 3D echocardiography at baseline and during biventricular pacing. The 3D echocardiographic determinants of exercise capacity were explored by univariate and stepwise multiple linear regression analysis with the changes relative to baseline entered into the equation. All data are presented as mean (SD).
Results
FEASIBILITY
All patients had successful pacemaker implantation. The LV lead was inserted in a lateral or posterolateral vein in all but six patients, in whom the electrode was placed in an anterior vein. 3D echocardiography was feasible in all patients, but in one patient colour Doppler measurements were not available because of an error in data storage.
VENTRICULAR RESPONSES TO BIVENTRICULAR PACING
Biventricular pacing showed a variable haemodynamic response in different subjects resulting in large SDs for the patient group. The percentage changes for the 3D echocardiographic parameters—EDV, ESV, EF, forward SV, total SV, atrial systolic contribution to inflow, and mitral regurgitant fraction—are shown in table 2. Results of the six minute walk test and changes in QRS duration are shown in table 2. Pacing data were acquired with an atrioventricular interval of 113 (10) ms, which was significantly shorter than the baseline values of 240 (38) ms (p < 0.01). There were no significant differences between patients who were investigated one day after pacemaker implantation and patients investigated at baseline and 2–7 days after implantation.
Summary of haemodynamic and exercise responses to biventricular pacing
PREDICTORS OF CHANGES IN EXERCISE TEST
Univariate 3D echocardiographic predictors of improved walking distance were the changes in forward SV, mitral regurgitant fraction, EDV, and ESV. Multiple linear regression analysis identified the percentage change in forward SV as the only independent factor determining absolute and percentage improvement in walking distance (r 2 = 0.45v r 2 = 0.73, p = 0.008v p = 0.0002). One of the patients was not included in the analysis because of severe shortness of breath even at rest. In fig 1 the increase in walking distance is plotted versus percentage changes in forward SV. In five of 15 patients, an increase in forward SV above 15% was seen with biventricular pacing and this was predictive of an improvement in walking distance of more than 90 m (25% above baseline).

Correlation between percentage changes in forward stroke volume and increase in walking distance by six minute walk test. Patients with the largest increase in forward stroke volume had the greatest improvement in walking distance.
INFLUENCE OF BASELINE QRS DURATION AND CHANGES IN QRS DURATION
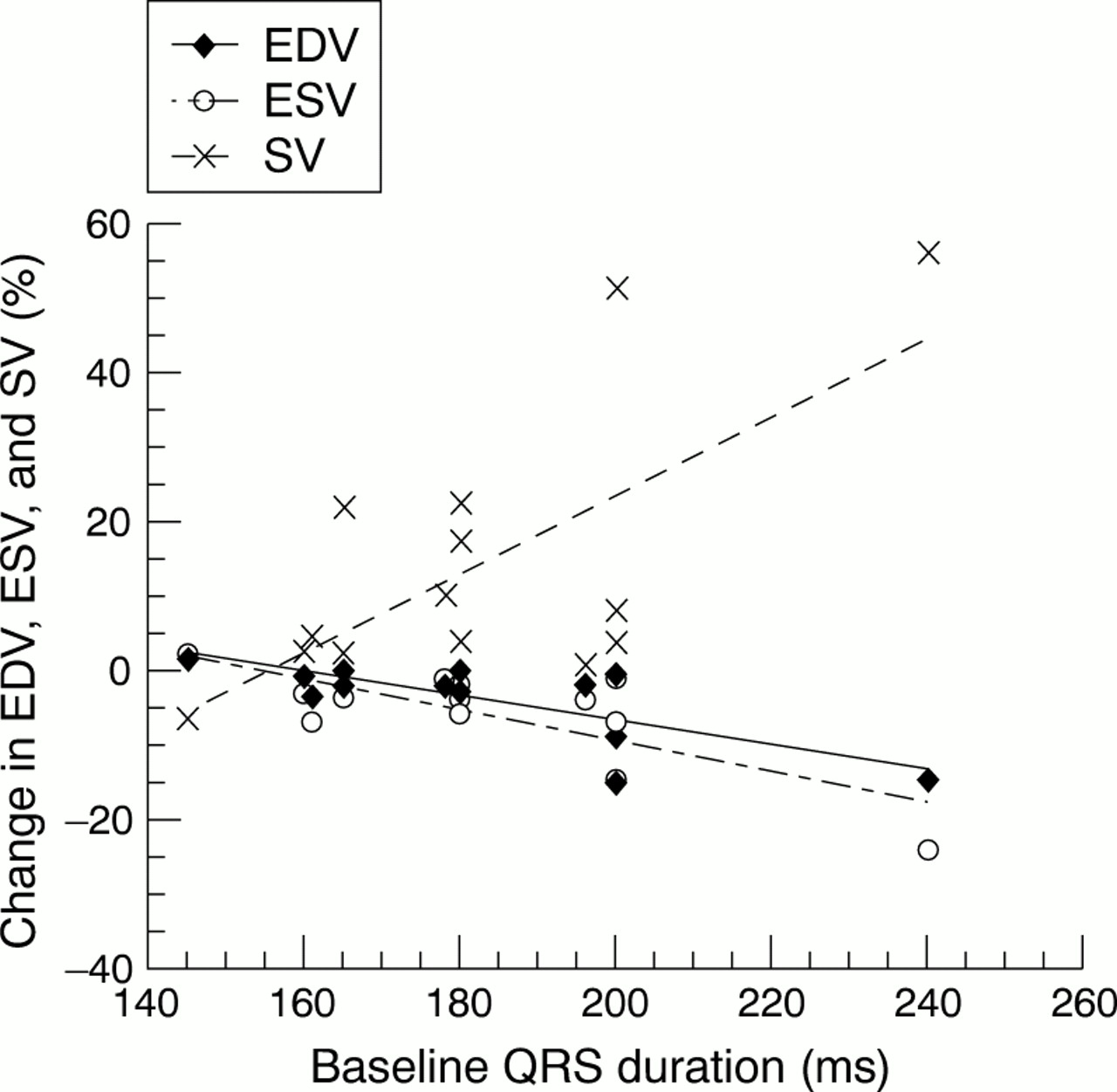
Univariate regression analysis showed that the basal QRS duration predicted an increase in forward SV and a reduction in EDV and ESV (fig2). Thus, patients with baseline QRS duration less than 165 ms did not show any substantial haemodynamic benefit.

Correlation between baseline QRS duration and pacing induced changes in end diastolic volume (EDV), end systolic volume (ESV), and forward stroke volume (SV). Patients with the longest baseline QRS duration showed the greatest benefit in terms of reduced left ventricular chamber size and increased forward stroke volume.
In addition, the reduction in QRS duration induced with biventricular pacing showed a modest but significant correlation with the increase in forward SV and the reduction in EDV and ESV (fig 3). Thus, patients with a reduction in QRS duration less than 20 ms did not show any substantial haemodynamic benefit. Stepwise multiple regression analysis revealed that baseline QRS duration was the only independent predictor of haemodynamic improvement in terms of increased forward SV and reduced EDV and ESV (r 2 = 0.46–0.59, p < 0.008 to 0.001).

{kind=link}
{kind=link}
{kind=link}
Correlation between pacing induced reduction in QRS duration and changes in end diastolic volume (EDV), end systolic volume (ESV), and forward stroke volume (SV). Patients with the largest reduction in QRS duration showed the greatest haemodynamic benefit.
Discussion
The present study supports recent acute invasive haemodynamic data showing that biventricular pacing in patients with heart failure and ventricular conduction delay increases systolic pressure4 and cardiac index,5 and enhances LV contractility.6 Thus, with 3D echocardiography we showed that forward SV was significantly augmented with an immediate reduction in LV chamber size and mitral regurgitant fraction. The increase in forward SV was predictive of improved exercise capacity in the study group. This study therefore shows the potential of 3D echocardiography for evaluating the haemodynamic effects induced by biventricular pacing in patients with heart failure.
MECHANISMS OF HAEMODYNAMIC EFFECTS OF BIVENTRICULAR PACING
The only independent predictor of the short term improvement of exercise capacity was the increase in forward SV. This can be ascribed to the low output heart failure in these patients with predominantly systolic dysfunction. Ventricular SV is a function of preload, afterload, and contractility.14 Accordingly, SV increases when there is an increase in preload, a decrease in afterload, or augmented contractility. With respect to biventricular pacing, it is important to emphasise that the observed rise in forward SV seems to result from cardiac resynchronisation leading to increased LV contraction synchrony and reduced mitral regurgitation. Obviously, both mechanisms promote antegrade SV. The improved LV systolic function is shown in the reduced ESV, which depends on afterload and contractility but not on preload.14 It has been hypothesised that by specifically pacing the LV region with delayed electrical activation, contractile synchrony and thereby systolic function is partly restored leading to a reduction in ESV. This electromechanical hypothesis is strongly supported by our data, which showed that patients with the widest baseline QRS duration and the greatest pacing induced QRS narrowing had the greatest haemodynamic benefit. This seems logical in that the greater the magnitude of conduction delay (QRS duration), and thereby LV dyssynchrony, the more benefit resulted from resynchronisation.
Altered geometry of mitral leaflet attachments associated with LV dilatation is supposed to increase the tethering forces on the mitral valve apparatus restraining the leaflets from closing. In experimental models, functional mitral regurgitation has been shown to occur when papillary muscles are displaced in the posterior and mediolateral directions.15 Conversely, the reduction in ESV during biventricular pacing is likely to be responsible for the reduction in mitral regurgitant fraction because a reduced ESV decreased mitral valve tethering forces. Whether specific pacing sites such as the posterior or lateral LV walls are preferable to reduce mitral regurgitation has to be investigated in future studies. With reduced mitral regurgitation volume, volume unloading leads to reduced EDV, which explains why EF did not change despite a significant increase in SV.
Biventricular pacing changed the diastolic inflow pattern from one characterised primarily by an early filling wave to one with more physiologically balanced early and atrial filling components. However, we were not able to show a direct effect of this altered diastolic filling pattern on exercise capacity. In addition, there was no correlation to the changes in forward SV or LV chamber sizes. It is therefore not clear to what extent changes in mitral inflow pattern affect clinical outcome.
METHODOLOGICAL CONSIDERATIONS OF 3D ECHOCARDIOGRAPHY
Because 3D echocardiography was used to obtain all haemodynamic parameters including LV volumes and volumetric flow rates, the validity of these measurements deserves comment. The recent introduction of tissue harmonic imaging has drastically improved ultrasound image quality and especially the definition of endocardial borders, which is pertinent for LV volume measurements. Thus, 3D echocardiography with tissue harmonic imaging closely agreed with magnetic resonance imaging for assessment of LV volumes in both healthy subjects and patients with dilated cardiomyopathy.16 In addition, 3D echocardiography in comparison with two dimensional echocardiography showed excellent day to day reproducibility for LV volume measurements in healthy subjects.7 Thus, the reproducibility of two dimensional compared with 3D echocardiography with harmonic imaging, expressed as the 95% range for change, was 22%v 10%, 34% v19%, and 9% v 5% for measurement of EDV, ESV, and EF, respectively. The reproducibility for the present study population should be similar since intraobserver variation (3–6%), which had the greatest impact on total variance7, was similar in healthy subjects and in patients with severe LV dysfunction and dilated hearts.16 It has recently been shown that the choice of imaging method (two dimensional or 3D) has a greater impact on the results than does the choice of imaging modality (echocardiography or magnetic resonance imaging) when measuring LV volume and systolic function.17
The 3D colour Doppler method has previously been evaluated for quantification of volumetric flow in patients.11 Thus, since pacemakers are contraindicated for magnetic resonance imaging, 3D echocardiography is in our opinion the most reproducible non-invasive tool for quantitative haemodynamic evaluation of the effects of biventricular pacing. The advantage of 3D echocardiography over invasive protocols is the possibility for serial as well as long term studies to explore the more chronic effects of pacing.
LIMITATIONS OF THE STUDY
The changes in exercise capacity were evaluated by a six minute walking test, which in every case was performed at first during baseline condition and secondly after pacemaker implantation. It has been shown that familiarisation results in a small increase of 6% in walking distance between two successive tests performed one day apart.18 In addition, a placebo effect of the pacemaker implantation may be expected. The ideal situation would be to perform the exercise test in random order and blinded to both the patient and the observer. Thus, if we look conservatively at the improvement in walking distance and use a cutoff value, we may speculate that the 12 of 15 patients who showed a substantial improvement above 20% showed a genuine short term improvement in exercise capacity. A regular exercise test of maximal exercise capacity on a treadmill or bicycle would have been difficult to accomplish in the majority of the patients in this study population because of the severity of heart failure symptoms. Thus, the average walking distance during six minutes in the study population at baseline was only 261 (105) m (range 0–390 m).
The 3D echocardiographic analysis and, in particular, the manual tracing of LV volumes are subjective and depend on image quality. Thus, a totally blinded data analysis would be preferable; however, neither the visible leads in the right ventricle nor the pace spikes occurring in the ECG tracings permit this. Instead the observer was blinded to the results of the exercise tests, the clinical status of the patient, and all pacing related parameters. In addition, when the paired data for each subject were analysed, the results were not compared directly during the analyses. For volumetric flow analysis, subjectivity is much less of a problem because the colour Doppler flow maps explicitly define both the area and the velocity for each pixel, which are summarised to calculate flow.
In five of the patients, 3D echocardiography was not performed at baseline but one day after pacemaker implantation with biventricular pacing on or off. However, there were no significant differences in the haemodynamic response compared with the patients who were investigated at baseline and 2–7 days after implantation, indicating that the effect of pacing is rather acute.
PRACTICAL IMPLICATIONS
The variable haemodynamic response to biventricular pacing in consecutive patients with heart failure indicates that each patient's baseline haemodynamic values should be screened before pacemaker implantation to ensure a rational treatment strategy. Our data showed a significant reduction in mitral regurgitation in all patients with more than trivial regurgitation. Thus, the present study suggests that patients with intraventricular conduction delay and moderate to severe functional mitral regurgitation would benefit from biventricular pacing. We confirmed invasive haemodynamic observations that a wider baseline QRS is associated with greater mechanical improvement.6 ,19 ,20 Our data also suggest that pacing induced changes in QRS width are predictive of the efficacy of biventricular pacing, even though the association was not very strong. In a six month follow up study, QRS duration during biventricular pacing was shown to be significantly shorter in patients who responded positively to pacing in terms of an increase in peak oxygen consumption rate.21 Other invasive studies did not show any predictive value of QRS narrowing but this could have been caused by differences in the pacing protocol, which in these studies was single site ventricular pacing6 ,20 compared with our simultaneous biventricular pacing protocol. LV single site pacing increased the width of the QRS complex. Therefore, at present baseline QRS duration remains an important parameter in both selection and evaluation of patients eligible for biventricular pacing. Tissue Doppler imaging may further improve patient selection by assessing the proportion of myocardium with asynchronous contraction.22
CONCLUSIONS
3D echocardiography documented a significant short term haemodynamic improvement by biventricular pacing in patients with heart failure and intraventricular conduction delay. In five of 15 consecutive patients with heart failure, biventricular pacing induced a more than 15% increase in forward SV, which predicted a more than 25% increase in walking distance. A baseline QRS duration ⩾ 165 ms with a reduction in QRS duration greater than 20 ms identified these patients. We believe that these results are very encouraging because they show that, in selected patients with medically refractory heart failure symptoms, biventricular pacing has the potential to provide a substantial and immediate improvement in haemodynamic profile and exercise capacity. Future studies should investigate the more chronic effects of biventricular pacing and try to establish even more precise criteria for patients who are candidates for pacing.
Acknowledgments
This work has been supported by grants from the Danish Heart Foundation, Copenhagen, Denmark.