Article Text

Abstract
OBJECTIVE To assess acute and chronic effects of surgical thromboendarterectomy on exercise capacity and ventilatory efficiency in patients with chronic thromboembolic pulmonary hypertension (CTEPH).
DESIGN Cardiopulmonary exercise testing was performed in 20 patients with CTEPH before thromboendarterectomy (baseline), one month after (early phase), and four months after (late phase). Peak oxygen uptake (peakV˙o 2) and the ventilatory response to carbon dioxide production (V˙e-V˙co 2 slope) were measured for assessment of exercise capacity and ventilatory efficiency. Right heart catheterisation was performed in all patients before and one month after surgery.
RESULTS Baseline peakV˙o 2 decreased andV˙e-V˙co 2 slope increased along with the increase in pulmonary vascular resistance in patients with CTEPH. After thromboendarterectomy, theV˙e-V˙co 2 slope decreased greatly from baseline to the early phase (mean (SD), 50 (9) to 37 (7), p < 0.05) and reached a steady level thereafter. In contrast, a continued increase in peak V˙o 2 was noted from the early to the late phase (16.9 (4.1) to 21.1 (5.0) ml/kg/min, p < 0.05). The decrease in theV˙e-V˙co 2 slope from baseline to the early phase, but not the increase in peakV˙o 2, correlated strongly with the decrease in pulmonary vascular resistance after surgery (r = 0.75, p < 0.01).
CONCLUSIONS Thromboendarterectomy may cause an immediate improvement in ventilatory efficiency, possibly through its beneficial haemodynamic effects. In contrast, exercise capacity may continue to improve towards the late phase, reflecting peripheral adaptation to exercise.
- thromboendarterectomy
- exercise capacity
- pulmonary thromboembolism
- pulmonary hypertension
Statistics from Altmetric.com
Chronic thromboembolic pulmonary hypertension (CTEPH) is the result of obstruction of the pulmonary arteries by thrombus.1 Most patients with CTEPH have severe exercise limitation because of the cardiopulmonary effects of the condition.2 For example, Janicki and colleagues have shown a decrease in peak exercise oxygen consumption (peak V˙o 2) and an increase in the regression slope relating minute ventilation to carbon dioxide output (V˙e-V˙co 2 slope) in patients with CTEPH, using cardiopulmonary exercise testing.3 Fortunately, pulmonary thromboendarterectomy has been shown to ameliorate pulmonary hypertension in patients with CTEPH.4 ,5 However, little information is available about the effects of thromboendarterectomy on exercise capacity and ventilatory efficiency. Peak V˙o 2 is determined not only by the maximum cardiac output during exercise but also by the potential for oxygen extraction in exercising muscle.6 On the other hand, the increase in theV˙e-V˙co 2 slope is associated with increased physiological dead space resulting from an impaired increase in pulmonary perfusion during exercise.7 ,8 Thus we hypothesised that peakV˙o 2 and theV˙e-V˙co 2 slope may represent differing aspects of cardiopulmonary and peripheral responses after thromboendarterectomy.
To assess the acute and chronic effects of thromboendarterectomy on exercise capacity and ventilatory efficiency, we examined serial changes in peak V˙o 2 and theV˙e-V˙co 2 slope after thromboendarterectomy, and the relations between changes in peakV˙o 2 andV˙e-V˙co 2 slope and those of haemodynamic variables after thromboendarterectomy.
Methods
STUDY SUBJECTS
Pulmonary thromboendarterectomy was performed in 21 patients with CTEPH between January 1996 and December 1999. One patient died from the surgical procedure. The remaining 20 consecutive patients with CTEPH (11 men and nine women, mean age 43 years, range 22–65 years) were enrolled in the study (table 1). All patients complained of dyspnoea on effort, and the mean duration of symptoms before surgery was 57 months (range six months to 11 years).
Baseline characteristics in 20 patients with chronic thromboembolic pulmonary hypertension
Anticoagulation was initiated in all the patients when we made the diagnosis of CTEPH and this was continued during the follow up period after surgery. Vasodilators such as calcium antagonists and beraprost sodium, an oral prostacyclin analogue, were used in 13 patients. Use of drugs was unchanged before and after surgery, except in three patients in whom vasodilators were discontinued because of significant improvements in pulmonary hypertension.
The diagnosis of CTEPH was made as follows.2 In brief, patients with clinical symptoms suggesting CTEPH initially underwent electrocardiography, chest radiography, echocardiography, and lung scanning. When pulmonary hypertension and right ventricular enlargement were identified by echocardiography, and perfusion defects were found on ventilation/perfusion lung scanning, we suspected the presence of CTEPH rather than primary pulmonary hypertension. The diagnosis was confirmed by pulmonary angiography. The characteristic angiographic findings of CTEPH—such as “pouching”, pulmonary arterial webs or bands, intimal irregularity, abrupt narrowing of major pulmonary vessels, and obstruction of lobar vessels—were found in all patients.9
Cardiac catheterisation was performed to confirm precapillary pulmonary hypertension (mean pulmonary arterial pressure > 25 mm Hg with pulmonary capillary wedge pressure < 12 mm Hg) and to rule out other causes of pulmonary hypertension, such as congenital heart disease, valvar heart disease, ischaemic heart disease, and cardiomyopathy.
The criteria for pulmonary thromboendarterectomy used in our institute were as defined by Moser and colleagues4: calculated pulmonary vascular resistance at rest greater than 300 dynes.s.cm–5 in a symptomatic patient; thrombus location in the main, lobar, or segmental arteries; absence of severe associated disease; and the willingness of the patient to accept the surgical risks. All subjects provided written informed consent.
To compare baseline exercise capacity and ventilatory efficiency in patients with CTEPH with the normal value for each variable, we also studied 24 healthy volunteers matched for age and sex (12 men and 12 women; mean age 46 years, range 21–75 years; mean height 1.64 m, range 1.47–1.80 m; mean weight 62 kg, range 41–87 kg). None was taking any drugs.
CARDIOPULMONARY EXERCISE TESTING
Cardiopulmonary exercise testing was performed in 20 patients with CTEPH before thromboendarterectomy (baseline), one month after (early phase), and four months after (late phase). The exercise test was performed on an upright bicycle ergometer. After a one minute warm up at 0 W, exercise work load was increased in a ramp pattern at 15 W/min to the symptom limited maximum. Heart rate was monitored with standard ECG leads, and blood pressure was measured at the brachial artery with a sphygmomanometer. Breath by breath gas analysis was performed using a respiromonitor (AE280, Minato Medical Science, Osaka, Japan) connected to a personal computer running analysing software.10 Exercise capacity was evaluated by peakV˙o 2, which was defined as the value of averaged data during the final 15 seconds of exercise. Ventilatory efficiency on exercise was represented by theV˙e-V˙co 2 slope, which was determined as the linear regression slope of V˙eand V˙co 2 from the start of exercise until the RC point (the time up until which ventilation is stimulated by CO2 output and end tidal CO2 tension begins to decrease).11 ,12
HAEMODYNAMIC STUDIES
Right heart catheterisation was performed in all patients before and one month after surgery. Haemodynamic variables including mean pulmonary artery pressure, mean right atrial pressure, and mean pulmonary wedge pressure were measured. Cardiac output was determined by the Fick method.13 Pulmonary vascular resistance was calculated according to the standard formula.
PULMONARY THROMBOENDARTERECTOMY
Pulmonary thromboendarterectomy was performed by a previously described method.14 ,15 After a median sternotomy, cardiopulmonary bypass was initiated. Pulmonary thromboendarterectomy was initially performed on the right pulmonary artery under intermittent circulatory arrest using deep hypothermia. Any loose thrombi in the lobar artery were removed, and pulmonary thromboendarterectomy was then carried out from lobar artery to the segmental arteries. After this the left pulmonary artery was incised and pulmonary thromboendarterectomy performed in a same way. The pulmonary arteries were then sutured and the patients weaned from cardiopulmonary bypass after restoration of body temperature to normal levels.
STATISTICAL ANALYSIS
All data are expressed as mean (SD). Comparisons of variables between the two groups were made by the unpaired Studentt test. Correlation coefficients between haemodynamic variables and cardiopulmonary exercise test results were determined by linear regression analysis. Changes in haemodynamics and exercise capacity after thromboendarterectomy were compared by the paired Student t test. Comparisons of the time course of peak V˙o 2 or theV˙e-V˙co 2 slope were made by one way analysis of variance (ANOVA) for repeated measures, followed by Scheffé's multiple comparison test. A probability value of p < 0.05 was considered significant.
Results
BASELINE EXERCISE CAPACITY
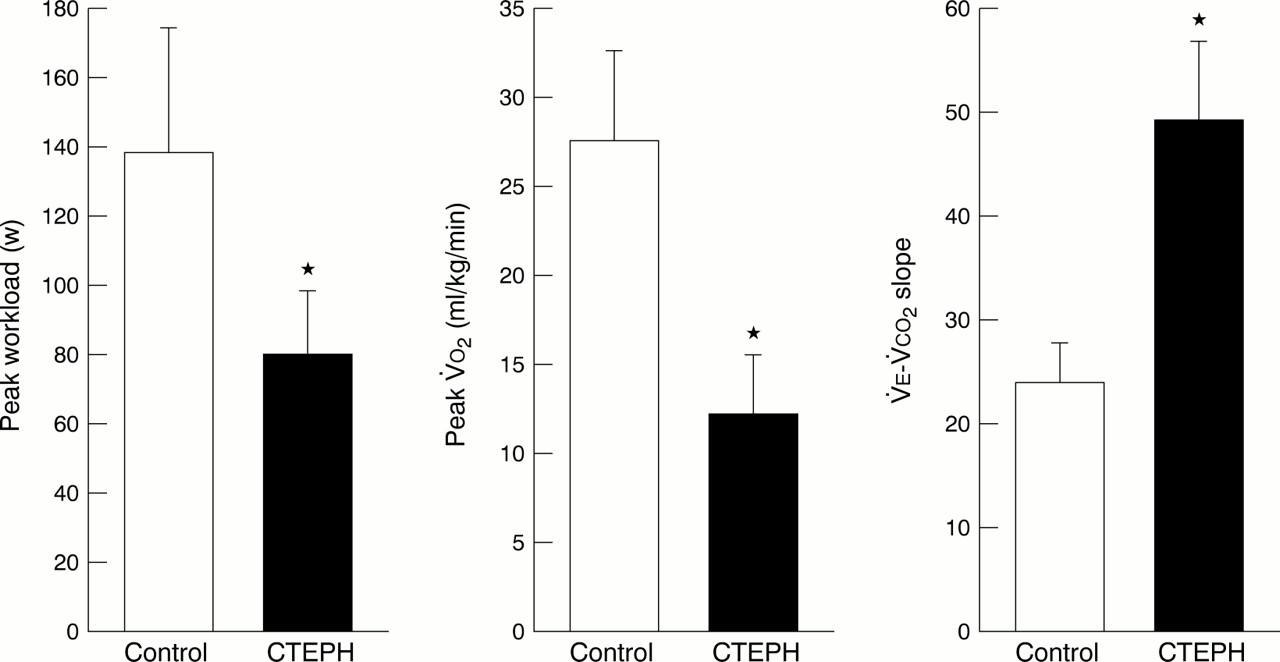
Baseline peak work load was significantly lower in patients with CTEPH than in the age matched healthy subjects (fig 1). Baseline peakV˙o 2 was also lower in patients with CTEPH than in the healthy subjects, whereas theV˙e-V˙co 2 slope was much higher than the normal value. There was a negative correlation between pulmonary vascular resistance and peakV˙o 2(r = −0.50, p < 0.05) and a positive correlation between pulmonary vascular resistance and theV˙e-V˙co 2 slope (r = 0.46, p < 0.05). A negative correlation was also found between mean pulmonary arterial pressure and peak V˙o 2(r = −0.61, p < 0.05), and a positive correlation between mean pulmonary arterial pressure and theV˙e-V˙co 2 slope (r = 0.45, p < 0.05). PeakV˙o 2 andV˙e-V˙co 2 slope were correlated with cardiac output (r = 0.50 and r = −0.45, both p < 0.05); however, neither was significantly correlated with pulmonary capillary wedge pressure (r = −0.26;r = 0.35, both NS).
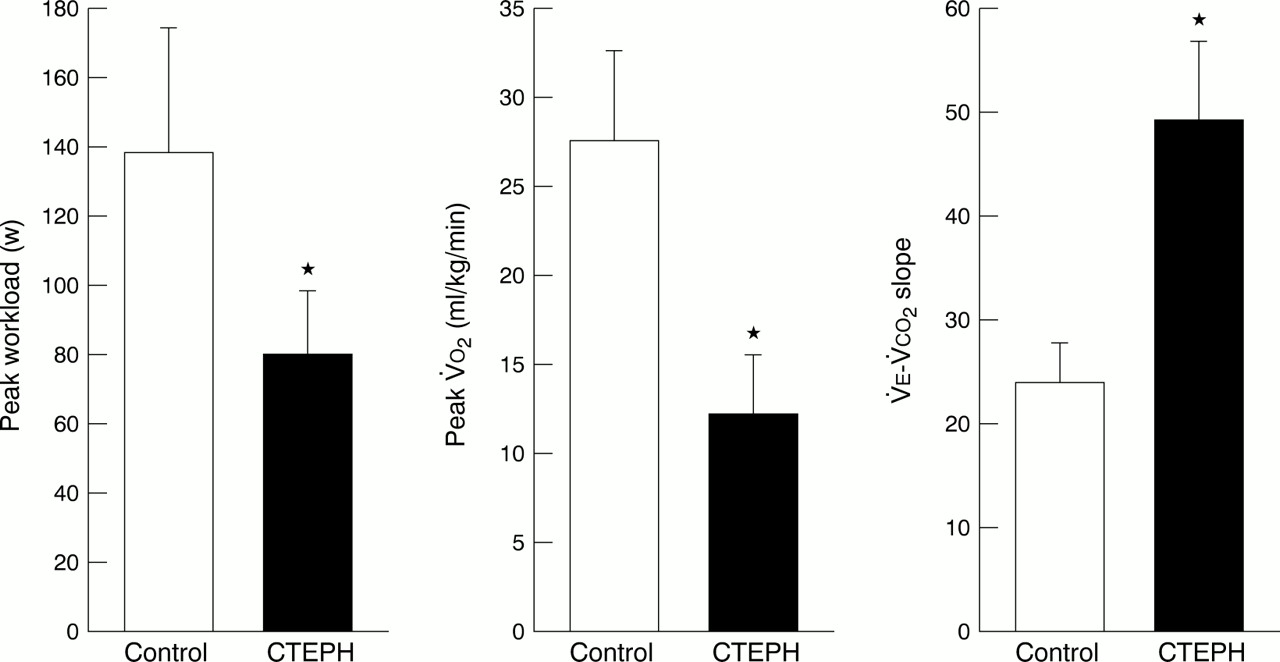
Peak work load (left panel), peakV˙o 2 (middle panel), and theV˙e-V˙co 2 slope (right panel) at baseline in patients with chronic thromboembolic pulmonary hypertension (CTEPH) and control subjects (Control). *p < 0.001 v control.
TIME COURSE OF EXERCISE CAPACITY AND VENTILATORY EFFICIENCY
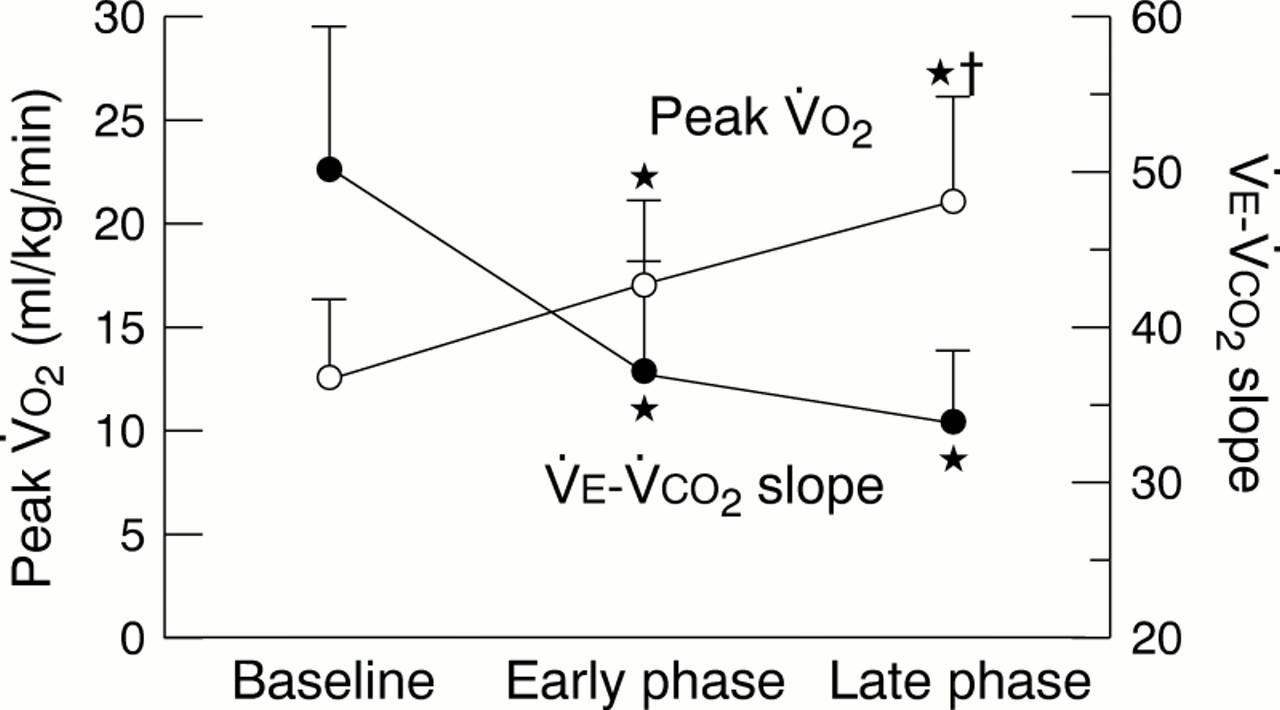
Pulmonary thromboendarterectomy caused an early improvement in haemodynamic responses: mean pulmonary artery pressure and pulmonary vascular resistance were notably decreased, while cardiac output was increased (table 2). TheV˙e-V˙co 2 slope decreased from baseline to the early phase (50 (9) to 37 (7), p < 0.05, fig 2) and reached a steady level thereafter, at around 33 (5). In contrast, a continued increase in peak V˙o 2 was noted from baseline to the early phase, as well as from the early phase to the late phase (baseline, 12.1 (3.6) ml/kg/min; early phase, 16.9 (4.1) ml/kg/min; late phase, 21.1 (5.0) ml/kg/min; fig2).
Haemodynamic variables before and after thromboendarterectomy

Time course of changes in peakV˙o 2 (empty circles) and theV˙e-V˙co 2 slope (filled circles) after thromboendarterectomy. *p < 0.05 v baseline;†p < 0.05 v early phase.
CHANGES IN EXERCISE CAPACITY AND VENTILATORY EFFICIENCY AND HAEMODYNAMIC IMPROVEMENTS
After thromboendarterectomy, there was no correlation between peakV˙o 2 and pulmonary vascular resistance (r = −0.41, p = 0.07). In contrast, there was still a positive correlation between theV˙e-V˙co 2 slope and pulmonary vascular resistance (r = 0.54, p < 0.05). The increase in peak V˙o 2from baseline to the early phase did not correlate significantly with the decrease in pulmonary vascular resistance (r = 0.42, p = 0.06, fig 3). However, the decrease in theV˙e-V˙co 2 slope from baseline to the early phase correlated strongly with the decrease in pulmonary vascular resistance (r = 0.75, p < 0.001). There were no correlations between changes in cardiac output and either peak V˙o 2 orV˙e-V˙co 2 slope (r = 0.16;r = 0.35, both NS).

Relations between changes in pulmonary vascular resistance (PVR) and changes in peak V˙o 2(left panel) and theV˙e-V˙co 2 slope (right panel) after thromboendarterectomy.
Discussion
There is little information about the acute and chronic effects of surgical thromboendarterectomy on exercise capacity and ventilatory efficiency in patients with CTEPH. In the present study we showed first, that baseline peak V˙o 2 decreased and the V˙e-V˙co 2 slope increased in parallel with an increase in pulmonary vascular resistance in patients with CTEPH; second, that theV˙e-V˙co 2 slope decreased significantly from baseline to the early phase after thromboendarterectomy and reached a steady level thereafter, whereas there was a continuous increase in peakV˙o 2 from baseline to the late phase; and third, that the decrease in theV˙e-V˙co 2 slope from baseline to the early phase, but not the increase in peakV˙o 2, correlated strongly with the decrease in pulmonary vascular resistance after surgery. Thus exercise capacity and ventilatory efficiency may represent differing responses after thromboendarterectomy, as indicated by peakV˙o 2 and theV˙e-V˙co 2 slope.
We noted a continued increase in peak V˙o 2from the early to the late phase after surgery, as well as from baseline to the early phase, suggesting that exercise capacity may continue to improve toward the late phase after thromboendarterectomy. These results support an earlier report that patients who underwent thromboendarterectomy showed continued improvement in quality of life over several months.2 Surprisingly, the increase in peakV˙o 2 after surgery did not correlate with the decrease in pulmonary vascular resistance. PeakV˙o 2 is influenced not only by cardiac output during exercise, but also by oxygen extraction in skeletal muscles and vasodilatation of the nutrient arterioles within working skeletal muscles.16-18 Thus peripheral adaptation to exercise in the late phase, as well as haemodynamic improvement in the early phase, may contribute to the increase in peakV˙o 2 and the improvement in exercise capacity after surgery.
The baseline V˙e-V˙co 2slope was higher in patients with CTEPH than in healthy subjects, suggesting the presence of an exaggerated ventilatory response to exercise (impaired ventilatory efficiency) in patients with CTEPH. One of the possible reasons for the increased ventilatory response during exercise could be the presence of significant ventilation–perfusion mismatch.7 ,8 In the present study, theV˙e-V˙co 2 slope decreased significantly from baseline to the early phase after thromboendarterectomy and reached a steady level thereafter. In addition, the decrease in theV˙e-V˙co 2 slope correlated strongly with the decrease in pulmonary vascular resistance. Thus we first demonstrated that unlike exercise capacity, the ventilatory efficiency was rapidly improved after thromboendarterectomy in association with acute haemodynamic changes. These results are consistent with recent reports that some vasodilators improve ventilatory efficiency in association with the reduction in pulmonary vascular resistance.19 ,20 Considering that lung perfusion scans and pulmonary angiography show major improvements in pulmonary perfusion after thromboendarterectomy,2 ,4 it is possible that the decrease in theV˙e-V˙co 2 slope may result from a decrease in physiological dead space caused by improvement in the ventilation to perfusion ratio. In contrast, theV˙e-V˙co 2 slope did not change from the early to the late phase after surgery. In the present study, right heart catheterisation was not performed in the late phase. However, it is well known that both pulmonary vascular resistance and angiographic findings are unaltered during a follow up period ranging from 3–16 months after surgery,2 which may be responsible for the lack of change in theV˙e-V˙co 2 slope in the late phase after surgery.
CLINICAL IMPLICATIONS
Cardiopulmonary exercise testing may allow non-invasive and relatively inexpensive assessments of exercise capacity and ventilatory response to exercise in patients with CTEPH. Baseline peakV˙o 2 decreased and theV˙e-V˙co 2 slope increased in relation to the degree of pulmonary vascular resistance. In addition, the immediate postoperative improvement in pulmonary vascular resistance was reflected by the decrease in theV˙e-V˙co 2 slope. Peripheral adaptation to exercise in the late phase is likely to parallel the increase in peak V˙o 2. Thus the combined measurement of peak V˙o 2(exercise capacity) and theV˙e-V˙co 2 slope (ventilatory efficiency) may serve as a non-invasive indicator of the severity of CTEPH and of the likely efficacy of surgical treatment.
CONCLUSIONS
Pulmonary thromboendarterectomy may result in an immediate improvement in ventilatory efficiency, probably through its beneficial haemodynamic effects. In contrast, exercise capacity may continue to improve toward the late phase, and this improvement may be related to peripheral adaptation to exercise.

{kind=link}
{kind=link}
{kind=link}
{kind=link}