Article Text

Abstract
Objective: To determine whether the changes in the manifestations of myocardial ischaemia during sequential angina episodes caused by exercise or coronary artery occlusion are collateral dependent.
Methods: 40 patients awaiting percutaneous transluminal coronary angioplasty for an isolated left anterior descending artery stenosis underwent three sequential treadmill exercise tests, with the second exertion separated from the first by 15 minutes, and from the third by 90 minutes; 28 patients subsequently completed two (> 180 s) sequential intracoronary balloon inflations with measurement of collateral flow index from mean coronary artery wedge, aortic, and coronary sinus pressures.
Results: On second compared with first exercise, time to 0.1 mV ST depression (mean (SD): 340 (27) v 266 (25) s) and rate–pressure product at 0.1 mV ST depression (22 068 (725) v 19 586 (584) beats/min/mm Hg) were increased (all p < 0.005), while angina and ventricular ectopic beat frequency were diminished (p < 0.05). This advantage, which had waned by the third effort, was independent of collateral flow index. Similarly, at the end of the second compared with the first coronary occlusion, ventricular tachycardia (21% v 0%, p < 0.05), ST elevation (0.47 (0.07) v 0.33 (0.05) mV, p < 0.005), and angina severity (6.1 (0.7) v 4.6 (0.7) units, p < 0.005) were reduced despite similar collateral flow indices.
Conclusions: In patients with coronary artery disease, ventricular arrhythmias, ST deviation, and angina are reduced during a second exertion or during a second coronary occlusion. This protective effect can occur independently of collateral recruitment. These characteristics, together with the breadth and temporal pattern of protection, are consistent with ischaemic preconditioning.
- angina
- collateral circulation
- ischaemia
- arrhythmia
- CFI, collateral flow index
- CSP, coronary sinus pressure
- LAD, left anterior descending
- Pao, aortic pressure
- Poccl, distal coronary artery wedge pressure
- PTCA, percutaneous transluminal coronary angioplasty
Statistics from Altmetric.com
- CFI, collateral flow index
- CSP, coronary sinus pressure
- LAD, left anterior descending
- Pao, aortic pressure
- Poccl, distal coronary artery wedge pressure
- PTCA, percutaneous transluminal coronary angioplasty
The variable relation between exercise and angina has been recognised for more than 200 years.1 This variability is reflected by the terms “first effort”, “warm up”, or “first hole” angina, used to describe the ability of some patients to exercise to angina, rest, and then continue exertion with reduced symptoms or none at all. The traditional view is that angina is the result of an imbalance between the supply and demand of the myocardium for blood.2,3 The explanation of warm up angina has therefore been that myocardial blood flow is enhanced on second effort by the opening of collateral channels. However, the relatively recent observation of an experimental phenomenon known as ischaemic preconditioning4 has increased our understanding of how the heart is able to adapt to brief episodes of ischaemia.5
Ischaemic preconditioning is the term used to describe the increased myocardial resistance to ischaemia that follows a brief episode of ischaemia.4 In animal models it protects against infarct size and arrhythmias.6 In contrast to warm up angina, ischaemic preconditioning does not depend on an increase in myocardial blood flow but is definitely caused by an increase in the intrinsic resistance of the heart to ischaemia.5
In order to determine whether a phenomenon similar to preconditioning occurs in patients, investigators have measured the severity of ischaemia during two sequential coronary artery occlusions at the time of percutaneous transluminal coronary angioplasty (PTCA).7–,9 Under these circumstances most investigators find that angina and myocardial ischaemia are more severe at corresponding times during the first than during subsequent balloon inflations. However, the interpretation of these studies is confounded by the use of durations of coronary artery occlusion that may be too short to alter myocardial resistance to ischaemia,10,11 by infrequent measurements of collateral blood flow, and by a focus on ST segment deviation and angina severity rather than on other measures of myocardial ischaemia such as arrhythmias.
Our aim in this investigation was to determine the magnitude, manifestations, and mechanisms of adaptation to myocardial ischaemia induced by exercise and coronary artery occlusion in a single group of patients with angina caused by an isolated left anterior descending (LAD) coronary artery stenosis.
METHODS
Patients
Patients entered in the study had chronic stable angina caused by single vessel LAD disease, and were awaiting elective PTCA. All patients had normal left ventricular function and a normal resting ECG without bundle branch aberration.
The study consisted of two parts. First, to assess warm up during exercise, patients underwent serial exercise testing. Second, to assess the effects of repeated coronary artery occlusions, patients underwent serial balloon inflations during PTCA. It was during the second study that the collateral flow index was measured. Calcium antagonists, angiotensin converting enzyme inhibitors, nicorandil, β blockers, long acting nitrates, and sulfonylureas were discontinued for at least 48 hours before each study.
The St Thomas’ Hospital research ethics committee approved the study, and written informed consent was obtained from each patient.
Exercise protocol
Patients completed three consecutive exercise tests one week before PTCA. All patients were tested at 9 am and were instructed neither to undertake strenuous exercise nor to take caffeine for 24 hours before their test. The first test was considered the baseline test and the second was separated from the first by a 15 minute rest period. A third exercise test was performed after a further 90 minutes of rest and was used to control for a possible training effect. Exercise tests were done using the standard Bruce protocol on a Quinton Q5000 exercise treadmill (Quinton, Seattle, Washington, USA). A 12 lead ECG tracing was obtained every 20 seconds and blood pressure was recorded at baseline, peak exertion, 0.1 mV ST depression, and every three minutes during exercise and every two minutes during recovery. The level of the ST segment measured 0.08 seconds after the J point was calculated after signal averaging using the computer assisted system on the Q5000. ST segment deviation was also checked manually by a blinded investigator to confirm that conduction defects, arrhythmias, or a wandering baseline did not affect the computer interpretation. The lead with the greatest deviation was used for subsequent analysis. The ventricular ectopic beat frequency was also recorded. Chest pain was recorded on a subjective scale of 0 to 10 (0, no pain; 10, severe pain) every minute.
Criteria for terminating the exercise tests were physical exhaustion, severe chest pain, attaining maximum age related heart rate, ST depression of > 0.4 mV, or occurrence of severe arrhythmias. The primary end point was time to 0.1 mV ST depression; secondary end points were rate–pressure product at 0.1 mV ST depression, exercise duration, and ectopic frequency during the last minute of exercise.
PTCA protocol
Coronary sinus cannulation was done through the right femoral vein using a 6.0 F Simmons catheter. This allowed coronary sinus blood sampling and pressure measurement in the coronary venous bed. Baseline selective coronary angiography was done in multiple projections, using an 8 French guiding catheter introduced through the femoral artery, and aortic pressure was measured through this catheter. The severity of coronary artery stenosis was estimated from orthogonal views using a commercially available quantitative coronary angiography package (Quantim, Quinton, Seattle, Washington, USA).
Coronary collateral assessment
A 0.014 inch (0.36 mm) guide wire mounted pressure sensor (PressureWire XT, Radi Medical Systems, Uppsala, Sweden) was calibrated and advanced through the guiding catheter and positioned distal to the target lesion. The predilating balloon was then advanced over the wire and inflated to occlude antegrade flow. During balloon inflation, aortic pressure (Pao), coronary sinus pressure (CSP), and distal coronary artery wedge pressure (Poccl) were continually recorded. Collateral flow index (CFI) was calculated as (Poccl − CSP)/(Pao − CSP)12 at 30 second intervals during balloon occlusion.
Two balloon inflations of at least 180 seconds’ duration were separated by at least five minutes of reperfusion. The balloon was deflated prematurely only if the patient experienced one of the following: severe chest pain; a fall in systolic blood pressure of > 30 mm Hg; or a severe arrhythmia. For the period between inflations the balloon was withdrawn from the lesion site, with continuous monitoring of distal coronary artery pressure. Nitrates and opiates were withheld until completion of the protocol; if necessary benzodiazepines were used to sedate the patient.
Assessment of myocardial ischaemia
A 12 lead surface ECG was recorded before and every 30 seconds during inflation and reperfusion. Maximum ST segment deviation during PTCA on each trace was obtained from anonymised coded ECGs. The epicardial ECG of the ischaemic zone was monitored continuously through the guide wire. Chest pain severity was scored by the patient at 60 second intervals during balloon occlusion on an analogue scale from 0 to 10 (0, no pain; 10, severe pain). Ectopic beat frequency and the occurrence of ventricular tachycardia or fibrillation were recorded. The diagnosis and quantification of arrhythmias conformed to the Lambeth conventions.13
Statistical analysis
Collateral flow indices were compared at identical time points during the two coronary artery occlusions. Chest pain grade was compared every 60 seconds. Missing data points resulted in the exclusion of the patient from the relevant analyses.
Measurements obtained during either the first effort or during coronary artery occlusion were compared with corresponding measurements during the second effort or coronary artery occlusion, using a two tailed paired t test with Bonferroni correction for multiple comparisons. The non-parametric data were compared using Fisher’s exact test. Data are presented as mean (SEM). Significance was assumed at a probability value of p < 0.05.
RESULTS
Forty patients who met the entry criteria were recruited into the study. Of those in the exercise study, four were unable to perform all three tests and in three patients the first exercise test ended before 0.1 mV of ST depression. Thus 33 patients completed the exercise study. Thirty four patients underwent the PTCA protocol. Incomplete data were obtained in four patients and a further two patients experienced transient vessel closure during PTCA. Thus complete data were available in 28 patients, and 25 patients completed both studies.
The demographic characteristics of the patients are shown in table 1⇓.
Baseline characteristics
Exercise study
Figure 1A⇓ shows ECGs from a patient with reduced ST deviation on the second compared with the first exercise test. During subsequent PTCA this patient had no collateral recruitment despite two 3 minute periods of total coronary occlusion. Figure 1B⇓ shows ECGs of a patient who developed ventricular bigeminy with chest pain and ST segment depression during the first and third but not the second bout of exercise. These individual responses are reflected in the pooled data summarised in table 2⇓. Although patients were not selected on the basis of a history of warm up angina, ischaemic variables consistently improved during the second compared with the first exertion. This effect had worn off by the third exertion. Ectopic beat frequency at peak exertion was also significantly reduced during the second test (fig 1B⇓ and table 2⇓). Protection during warm up was as effective in patients who had or did not have significant coronary collateral support to the same ischaemic zone during coronary artery occlusion in the subsequent PTCA study (table 2⇓). In keeping with previous studies the main determinant of the improved performance of second effort was the amount of ischaemia during first effort. Heart rate and blood pressure were comparable at corresponding time points in each of the three exercise tests.
Collated results of three consecutive exercise tests: test 2 was separated from test 1 by 15 minutes of rest, and test 3 was separated from test 2 by 90 minutes of rest
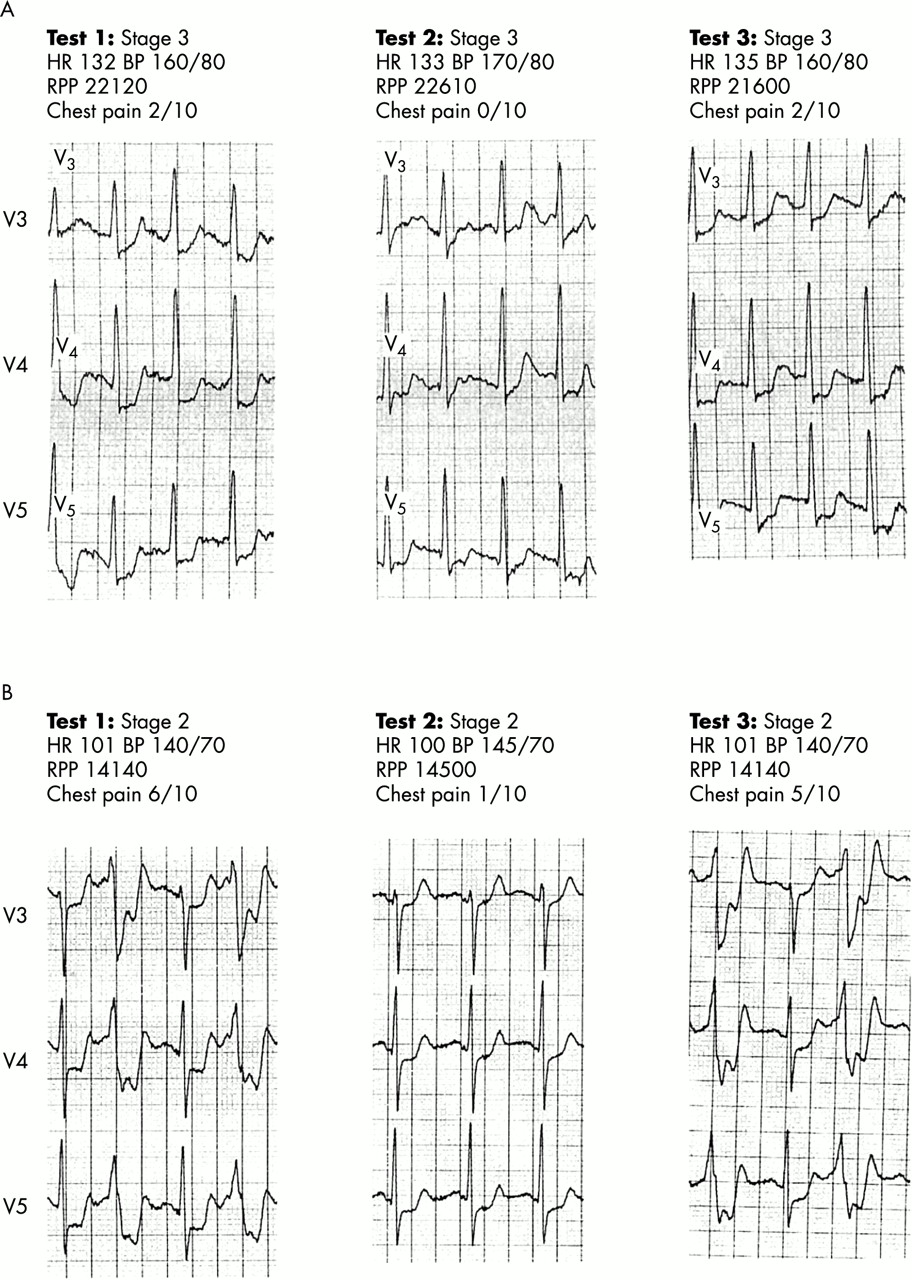
The appearance of the surface ECG during repetitive exercise. Patients were subjected to three consecutive treadmill exercise tests. Test 2 started 15 minutes after test 1 had been completed, and test 3 was begun 90 minutes after the end of test 2. Panels A and B consist of serial ECG recordings taken at identical time points into each of the three exercise tests in two different patients. (A) ST segment depression occurs in tests 1 and 3, but is absent at the identical time point in test 2 despite a similar rate–pressure product. (B) The record of a patient who developed ventricular bigeminy during tests 1 and 3. During these tests, the complexes with a narrow QRS morphology represent normally conducted beats with 0.4 mV of ST segment depression. At the corresponding time point during test 2, ST segment depression is less pronounced (0.2 mV) and is no longer accompanied by ventricular bigeminy.
PTCA study
Inflation time for first and second occlusions were 187 (5) and 196 (7) seconds, respectively. Figure 2A⇓ shows a 12 lead surface ECG recorded at 180 seconds of first and second coronary artery occlusion. There is less ST deviation during the second occlusion. Figure 2B⇓ shows the intracoronary ECG appearance, aortic pressure, coronary sinus pressure, and distal coronary artery pressure in the same patient and at the same time points as the recording of the surface ECG in fig 2A⇓. Mirroring the changes in the surface ECG, there is a notable reduction in ST segment elevation on the second versus the first occlusion, despite the absence of a change in myocardial collateral support. The attenuation of myocardial ischaemia on second coronary occlusion is reflected by the group data.
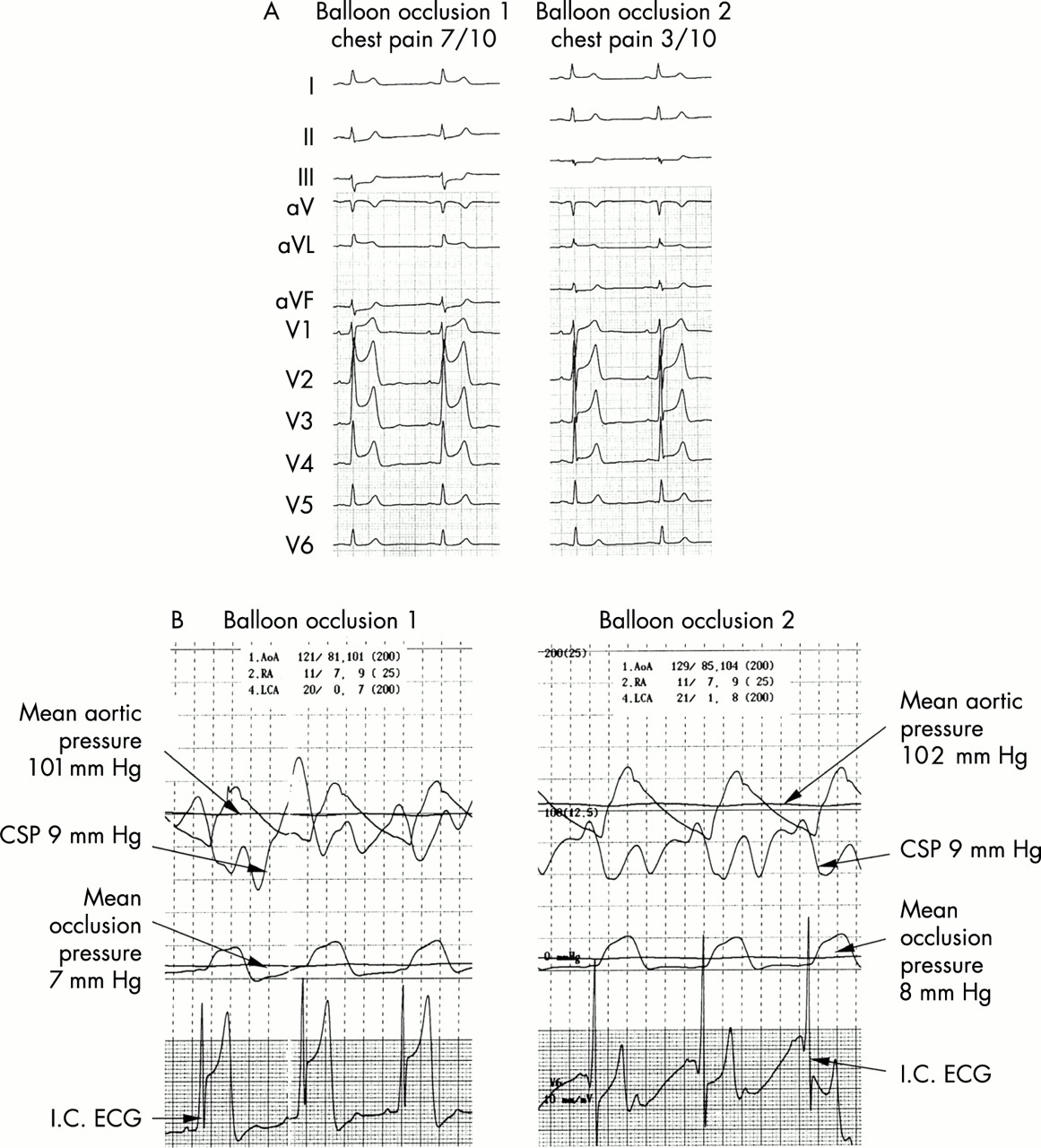
The effect of serial coronary artery occlusions on the surface ECG, intracoronary ECG, and pressures determining myocardial collateral blood flow. (A) The appearance of the surface ECG after 180 seconds of occlusion of the left anterior descending coronary artery (LAD) during percutaneous transluminal coronary angioplasty. The second occlusion began five minutes after the end of the first occlusion. The first episode of ischaemia causes ST segment elevation and QRS broadening without a shift in R wave axis. These changes are much less pronounced during the second occlusion. ST segment elevation confirms the presence of transmural myocardial ischaemia during both occlusions. (B) Records of pressures and intracoronary ECG during serial coronary artery occlusion. These traces were synchronous with the surface ECG appearing in panel A. The lowermost trace represents the intracoronary ECG recorded from the angioplasty guide wire. The intracoronary ECG reflects the changes seen in panel A with pronounced attenuation of ST segment elevation on second occlusion. The next uppermost trace is the pressure in the LAD distal to the site of balloon occlusion. The next uppermost trace is of the coronary sinus pressure (CSP) which is on a 25 mm Hg scale, as opposed to a 100 mm scale. Flow across the myocardial bed is largely determined by the difference between the venous and arterial pressure. During the first and second balloon occlusions the mean distal arterial pressure is virtually the same as the mean coronary sinus pressure and therefore there is no appreciable gradient to drive myocardial blood flow. Despite the absence of a change in myocardial blood flow, myocardial ischaemia is notably attenuated during the second inflation. This implies that myocardial resistance to ischaemia is enhanced during the second coronary artery occlusion. (For an explanation of the relation between pressure and collateral flow, see Methods.)
Figure 3⇓ shows the changes in ST deviation on the surface ECG, chest pain score, and collateral flow index during each of the two coronary artery occlusions for the whole patient group. There were no differences in collateral flow index between the first and second occlusions. However, there was a significant increase in collateral support with inflation time during both occlusions (p < 0.005). Despite identical collateral support, patients experienced reduced symptoms and ECG changes during the second coronary occlusion (both p < 0.005). Furthermore, ventricular arrhythmias were seen in 14 patients (50%) during the first occlusion compared with seven (25%) during the second occlusion (p < 0.05) (table 3⇓). In addition, six patients (21%) developed probable ventricular tachycardia during the first coronary occlusion but not during the second occlusion (p < 0.05) (fig 4⇓, table 3⇓). Although collateral support did not determine the magnitude of adaptation on second occlusion, the depth of ischaemia during the first occlusion was related closely to the degree of subsequent protection (correlation coefficient 0.78, p < 0.000006).
Frequency of arrhythmias during consecutive 180 second balloon occlusions of left anterior descending coronary artery
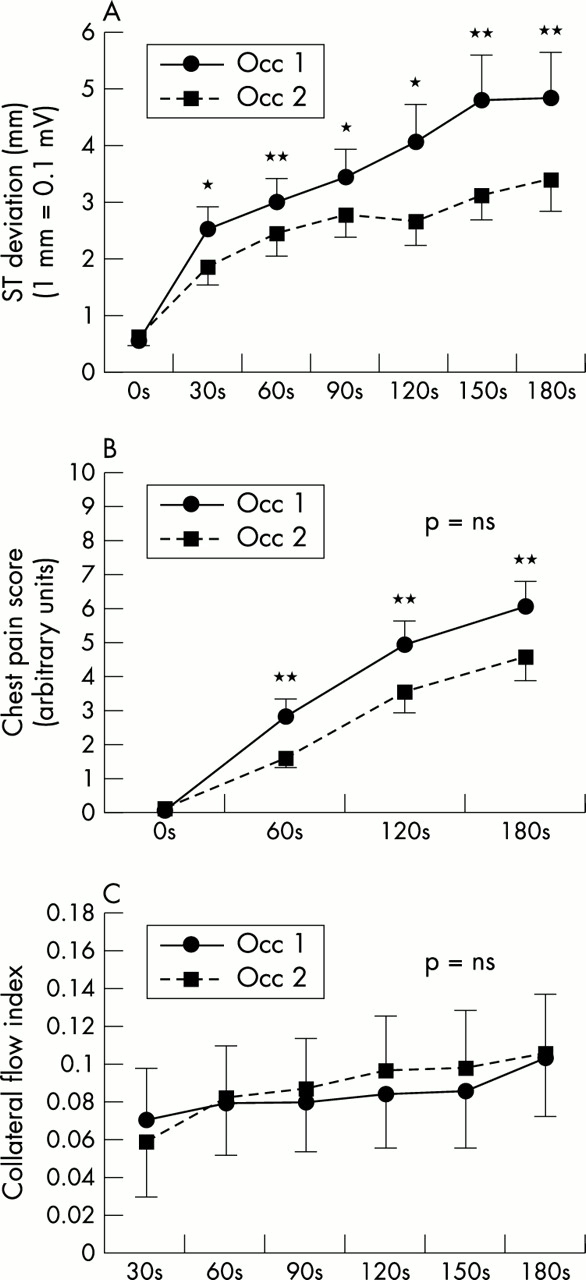
Changes in (A) ST segment deviation, (B) chest pain intensity, and (C) collateral flow index during the first and second coronary artery occlusions. Chest discomfort and ST segment deviation are significantly reduced on the second compared with the first balloon occlusion. In keeping with the changes seen in fig 2⇑, the reduction in these measures of myocardial ischaemia is not accompanied by an increase in myocardial collateral blood flow. In patients reaching three minutes of balloon occlusion the collateral flow increased in both groups with increasing duration of ischaemia. *p < 0.05, occlusion 1 v occlusion 2; §p < 0.005, occlusion 1 v occlusion 2; †p < 0.001, occlusion 1 v occlusion 2; ‡p < 0.0005 occlusion 1 v occlusion 2.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cardiac rhythm at peak inflation in patients with ventricular tachycardia associated with coronary artery occlusion. The left panel shows traces from patients developing ventricular arrhythmias during the first intracoronary balloon occlusion. The right panel shows traces at similar time points during the second occlusion. Note that ventricular tachycardia was confined to first balloon occlusion and absent during the second at the same and later time points. The collateral flow index at the time of recording appears above each trace. Collateral flow indices below 0.25 are thought insufficient to prevent ischaemia.
DISCUSSION
To our knowledge this is the first clinical study to show that myocardial ischaemia induced by prolonged coronary occlusion during PTCA, followed by a short episode of reperfusion, reduces the occurrence of ventricular tachycardia during a second occlusion. Furthermore, it is also the first to demonstrate that ischaemia induced by exercise reduces the occurrence of ventricular ectopic activity during a subsequent similar exertion. In addition, whether initiated by exercise or coronary artery occlusion, the magnitude of the reduction in angina and ST segment deviation is pronounced, at approximately 25–30%.
We have also shown that this adaptation to ischaemia was not caused by an increase in collateral flow and was equally notable in patients without coronary collaterals. This suggests that an increase in the endogenous resistance of the myocardium to ischaemia is responsible for the improved electrical stability, attenuated ST segment shift, and diminished angina.
Potential mechanisms underlying the warm up effect
Our observations indicate less myocardial injury with second exercise or coronary artery occlusion. The amount of myocardial injury caused by ischaemia has four determinants.14 The first determinant is the duration of ischaemia. This cannot explain our results, as the duration of both the second exercise and second coronary artery occlusion were greater than the first. The second determinant is the volume of myocardium subjected to ischaemia. As our patients had a single discrete obstruction within the left anterior descending coronary artery the volume of myocardium rendered ischaemic would not vary between each exercise test or balloon occlusion. The third determinant is the depth of myocardial ischaemia. This depends on the amount of blood flow reaching the myocardium through a combination of antegrade flow through the diseased coronary artery and retrograde flow through collaterals. During the PTCA study, antegrade flow was prevented by an occlusive balloon, while retrograde flow was measured by distal coronary pressure and did not vary between first and second balloon inflations. The fourth and only remaining determinant is the endogenous resistance of the myocardium to ischaemia.
Determinants of endogenous resistance to myocardial ischaemia
It has been shown that myocardial ischaemia may initiate an increase in the endogenous resistance of the myocardium to further ischaemia.4 This form of protection, known as ischaemic preconditioning, could explain the findings in our study. Some of our observations are suggestive of ischaemic preconditioning. For example, with repeat coronary occlusion ischaemic preconditioning causes an identical pattern of attenuated ST segment deviation15 and this a true measure of protection from necrosis in the absence of specific blockers of the sarcolemmal ATP dependent potassium channel.16 Animal models of ischaemic preconditioning have also usually, but not universally, been characterised by a reduction in ventricular arrhythmias.6 Other features in common with preconditioning are the presence of protection at 5 and 15, but not 90, minutes17 after an initiating ischaemic episode of at least three minutes’ duration.18 These results and other features add further weight to the argument that the adaptation we observed may be a clinical correlate of the experimental phenomenon of ischaemic preconditioning.2 Although previous studies support the concept that adaptation to myocardial ischaemia induced by intracoronary balloon occlusion is a form of ischaemic preconditioning, reports on serial exertion are more complex, with studies both consistent19 and inconsistent20 with a preconditioning-like mechanism.
Preconditioning and arrhythmia
The mechanisms that trigger ischaemia induced arrhythmias are complex but may involve the generation of reactive oxygen species. These are thought to arise from NADPH oxidase, xanthine oxidase, and mitochondrial derived oxidants. Although the xanthine/xanthine oxidase system is thought to be relatively unimportant in the human heart, this view has been challenged by recent studies.21 It is therefore possible that the mechanism of ischaemia induced arrhythmia is similar in human and animal hearts. Thus it is not surprising that an antiarrhythmic effect was also documented in the earliest of preconditioning studies22 and consistently reproduced in dogs and rodents but not pigs and rabbits. As a similar antiarrhythmic effect has also been observed by others during spontaneous sequential episodes of myocardial ischaemia in patients,23,24 it seems that human myocardium may behave like rodent myocardium in this respect.
Role of collateral flow
The first description of a reduction in angina following a previous episode of angina was in 1772, when, at the Royal College of Physicians in London, William Heberden read a letter that he had received from a patient. The patient described the ability to exercise to angina and then continue exertion with few or no symptoms. In the past it was thought that the warm up phenomenon was caused by vasodilatation of coronary collaterals.25,26 However, documentary proof was lacking, while more recent attempts to demonstrate collateral recruitment failed to show the expected associated increase in coronary vein flow or radiographic opacification of collateral vessels.27 However, these techniques are insensitive12 and may have failed to detect significant collateral flow.
In the present study there were nine patients (25%) with no demonstrable collaterals despite six minutes of coronary artery occlusion. Collateral recruitment is determined by the blood pressure gradient between adjacent myocardial vascular beds.28 The absence of collateral recruitment after six minutes of coronary artery occlusion, when the pressure in the myocardial vascular bed is as low as venous pressure, almost certainly predicts the absence of collateral recruitment during exercise when the coronary artery remains patent. We believe that our results indicate that in warm up angina initiated either by exercise, when collaterals were not assessed, or by coronary artery occlusion, when collaterals were assessed, protection is independent of collateral recruitment. However, in patients with well developed collaterals—who were relatively poorly represented in our study—collateral recruitment has been shown to contribute to the attenuation of ischaemia on subsequent balloon inflations.8,29
The issue of collateral recruitment as an important confounding variable has also been addressed by other groups. Sakata and colleagues employed myocardial contrast echo,30 and Tomai and associates used the flow wire positioned in the contralateral coronary artery,31 to determine small changes in collateral flow between inflations. However, both techniques are insensitive and subject to error.32 In addition, previous studies have used balloon inflation times of only 120 seconds. Although inflations of this duration attenuate subsequent ischaemia in many studies, this cannot always be replicated.33 Furthermore, more prolonged durations of occlusion may be required to trigger adaptation in elderly patients.11 One possible explanation that is supported by laboratory data is that 120 seconds lies on, or very close to, the duration threshold that triggers preconditioning.17 A further difficulty with coronary occlusions of 120 seconds or less is incomplete collateral recruitment (see fig 3⇑). Thus the use of shorter occlusions may have resulted in the greater contribution of collaterals to the overall attenuation of ischaemia on subsequent inflations reported by other investigators who also adopted a similar protocol of pressure derived collateral flow measurement.29
Clinical implications
We present the first observation that a previous episode of myocardial ischaemia can paradoxically reduce the occurrence of ventricular arrhythmia during coronary artery occlusion and exercise. These observations may have direct clinical relevance. Although the causes of sudden cardiac death can be diverse, it is thought that most are the result of ventricular arrhythmias.34 In those patients with a macroscopically normal heart these arrhythmias are thought to occur within minutes of a coronary artery occlusion.34 Thus these so called fatal “phase I” arrhythmias share the initiation by coronary artery occlusion and the temporal characteristics with the iatrogenic arrhythmias that we observed during the first intracoronary balloon occlusion. However, despite the absence of alterations in collateral flow these arrhythmias did not occur during the second balloon occlusion (fig 4⇑). Similarly, although the prognostic value of exercise induced ventricular ectopy remains controversial, there is recent evidence that it too may be associated with an adverse prognosis.35,36 By inference, our observation of reduced ventricular ectopy on second exercise may have prognostic connotations. If these extrapolations of our findings are correct the adaptive phenomenon we have observed could have an unmeasured benefit on mortality in addition to the measured benefit on morbidity.
Acknowledgments
This study was supported by the British Heart Foundation, grant FS/97084. We thank our colleagues at St Thomas’ hospital for enabling this study to take place.