Article Text

Abstract
Background: The role of exercise testing in the follow up of adults with a coarctation repair is unclear. Exercise induced systolic hypertension has been advocated as an indication for further investigation; however, the value of exercise testing in this role has been questioned, especially in paediatric populations.
Objective: To assess the value of resting and exercise blood pressure measurements in a cohort of adults with repaired coarctation.
Setting: Tertiary referral centre for adult congenital cardiac disease.
Patients: 56 patients (33 male, 23 female) with a previous coarctation repair, and 33 age matched controls.
Main outcome measures: Resting and exercise blood pressures, including arm–leg systolic blood pressure gradients; standard echocardiographic measurements of left ventricular mass, aortic root diameter, and repair site gradient.
Results: The coarctation cohort had higher resting upper limb blood pressures than the controls (systolic: 129.7 v 120.7 mm Hg, p = 0.014; diastolic: 76.8 v 72.2 mm Hg, p = 0.02). Mean resting arm–leg systolic blood pressure gradient was also higher, at 3.6 v −2.2 mm Hg, p = 0.027. However, there were no differences between the peak exercise systolic blood pressures of the two groups. Peak exercise systolic blood pressure did not correlate with resting arm–leg blood pressure gradient (r = 0.24, p = 0.13) or with repair site gradient (r = 0.14, p = 0.39). Resting upper limb systolic blood pressure and resting arm–leg systolic blood pressure gradient were related to repair site gradient (r = 0.33, p = 0.03, and r = 0.47, p = 0.002).
Conclusions: Measurements of upper limb blood pressure during exercise are of limited value in the assessment of the post-repair coarctation patient. If routine exercise testing is to be advocated in this population it must be for another indication.
- coarctation
- blood pressure
- exercise
Statistics from Altmetric.com
It has been advocated that exercise testing is an essential part of the postsurgical follow up of the patient with a coarctation repair.1 The indications for this assessment have included detection of aortic recoarctation and identification of patients with abnormally raised exercise systolic blood pressure.2 Recoarctation is not uncommon in this population3 and can be effectively treated with a wide range of surgical and transcatheter techniques.4 Magnetic resonance imaging has greatly facilitated the diagnosis of recoarctation but is not always available, particularly in non-specialist centres. The clinician therefore has a limited number of diagnostic tools to determine which patients should be investigated further. The value of the exercise test in this role remains unclear,5 and our aim in the present study was to investigate the relative usefulness of upper and lower limb blood pressures at rest and following exercise in a cohort of adults with repaired coarctation.
METHODS
Patients
Consecutive adults with repaired coarctation attending the outpatient clinic of the University of Toronto Congenital Cardiac Centre for Adults were identified from the institute’s database. Patients were invited to participate in the study when attending their review appointment. Exclusion criteria were: any degree of left ventricular outflow tract obstruction (defined as an echo Doppler gradient of more than 16 mm Hg on their last echocardiographic examination); patients with known coronary artery disease; and patients who would be unable to perform an exercise test.
A control cohort was also studied. This consisted of normotensive healthy subjects recruited from hospital staff.
Approval for the study was given by the institute’s ethics committee.
Blood pressure recordings
Blood pressure was measured in the right arm and left leg using an automated device (Dinamap vital signs monitor, Critikon Inc, Tampa, Florida, USA). Measurements were made with subjects in the supine position at rest and averaged from at least two separate readings. These measurements were repeated immediately after symptom limiting exercise and at four minutes into recovery.
Echocardiography
Patients underwent transthoracic echocardiography using a Sonos 2500 system (Hewlett-Packard Inc, Andover, Massachusetts, USA). Echocardiographic investigations followed the guidelines of the American Society of Echocardiography. A leading edge to leading edge technique was used for M mode measurements. Left ventricular mass was calculated using the Penn convention.6 Successful imaging of the aortic arch was possible from the suprasternal approach in all but one case. The peak aortic repair site gradient was determined by continuous wave Doppler flow signals, using the modified Bernoulli equation. Echocardiographic analysis was undertaken by a single experienced individual blinded to the subjects’ other results. All measurements analysed were taken from the average of at least four cardiac cycles.
Exercise testing
Symptom limited treadmill exercise testing followed a standard Bruce protocol. Exercise time, peak heart rate, and functional capacity (in metabolic equivalents (METs)) were recorded in all cases. Immediately after exercise, further supine blood pressure recordings were made and repeated after four minutes.
Statistics
Descriptive data for the cohort are quoted as mean (SD). Differences between groups were compared using an unpaired t test. The relations between variables are quoted as Pearson’s correlation coefficients (r). A probability value of p < 0.05 was taken to be significant.
RESULTS
Study population
We studied 56 subjects (33 male, 23 female), mean (SD) age 29.8 (11.0) years. Age at initial repair was 8.4 (8.9) years. Twenty three per cent of the cohort had coarctation repair within the first year of life. The most common form of repair was end to end anastomosis (n = 30 (54%)), followed by patch grafting (n = 7 (11%)), and subclavian flap repair (n = 6 (11%)). Six subjects (11%) had a catheter procedure as their primary intervention. Ten patients had had redo surgical procedures (at mean age 20 (17.5) years) for recoarctation or the presence of an aneurysm.
The majority of the cohort (n = 37 (66%)) had bicuspid aortic valves, although none was associated with haemodynamically significant aortic stenosis or regurgitation. Nine patients were taking regular vasoactive drugs (eight for hypertension; one for angina) and their data were therefore excluded in the subsequent analysis. The mean age of the control cohort (23 men and 13 women) was 30.6 years.
Resting blood pressure
The coarctation subjects had higher resting upper limb blood pressures than the control group (systolic: 129.7 v 120.7 mm Hg, p = 0.014; diastolic: 76.8 v 72.2 mm Hg, p = 0.02). Twelve (26%) of the coarctation cohort had a resting systolic blood pressure of more than 140 mm Hg; eight (17.4%) had a resting diastolic blood pressure of more than 85 mm Hg. The equivalent numbers from the control group were three (9%) and 0. Resting and exercise blood pressure values for the two groups are given in table 1.
Resting and exercise blood pressures in the two groups
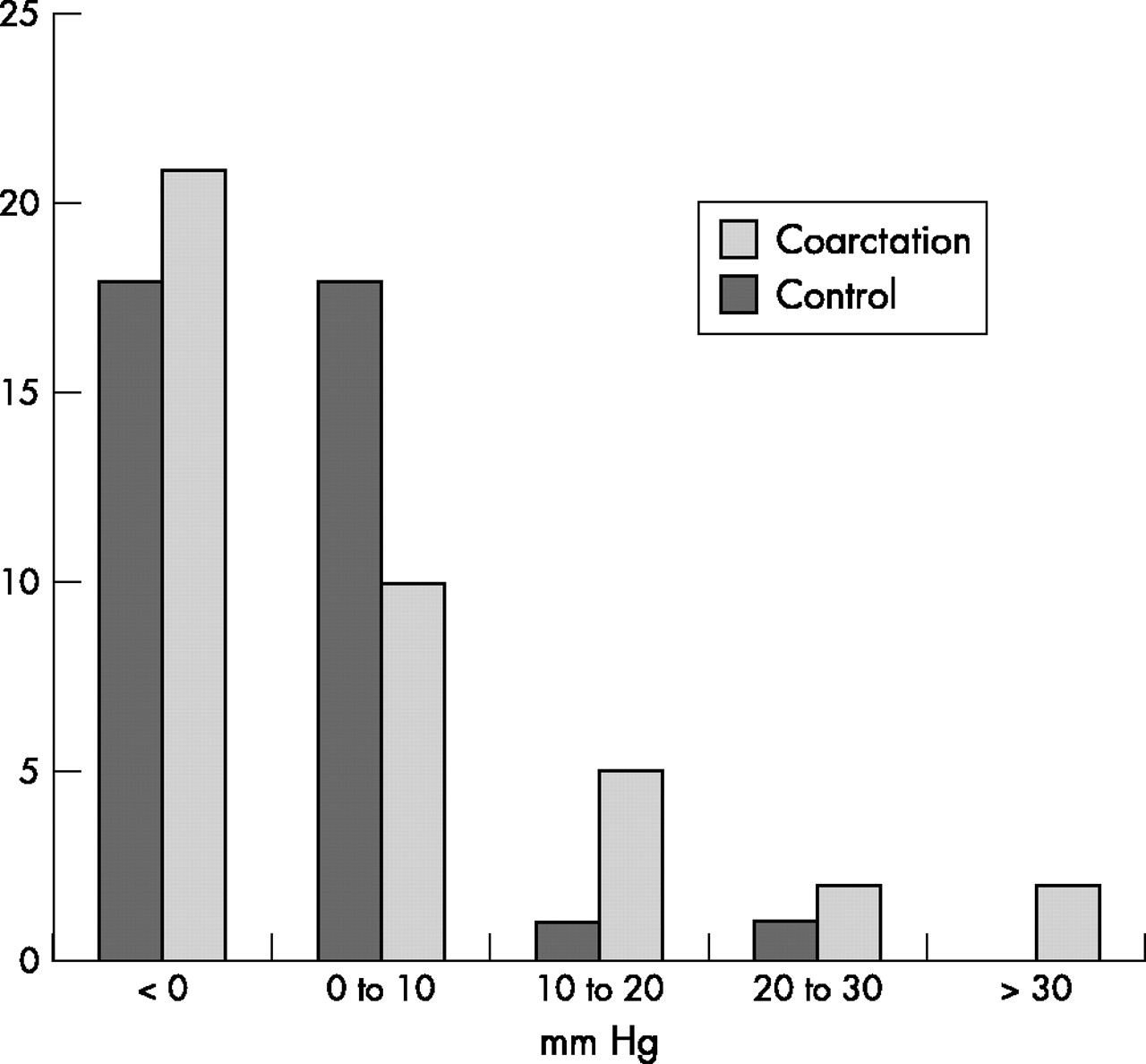
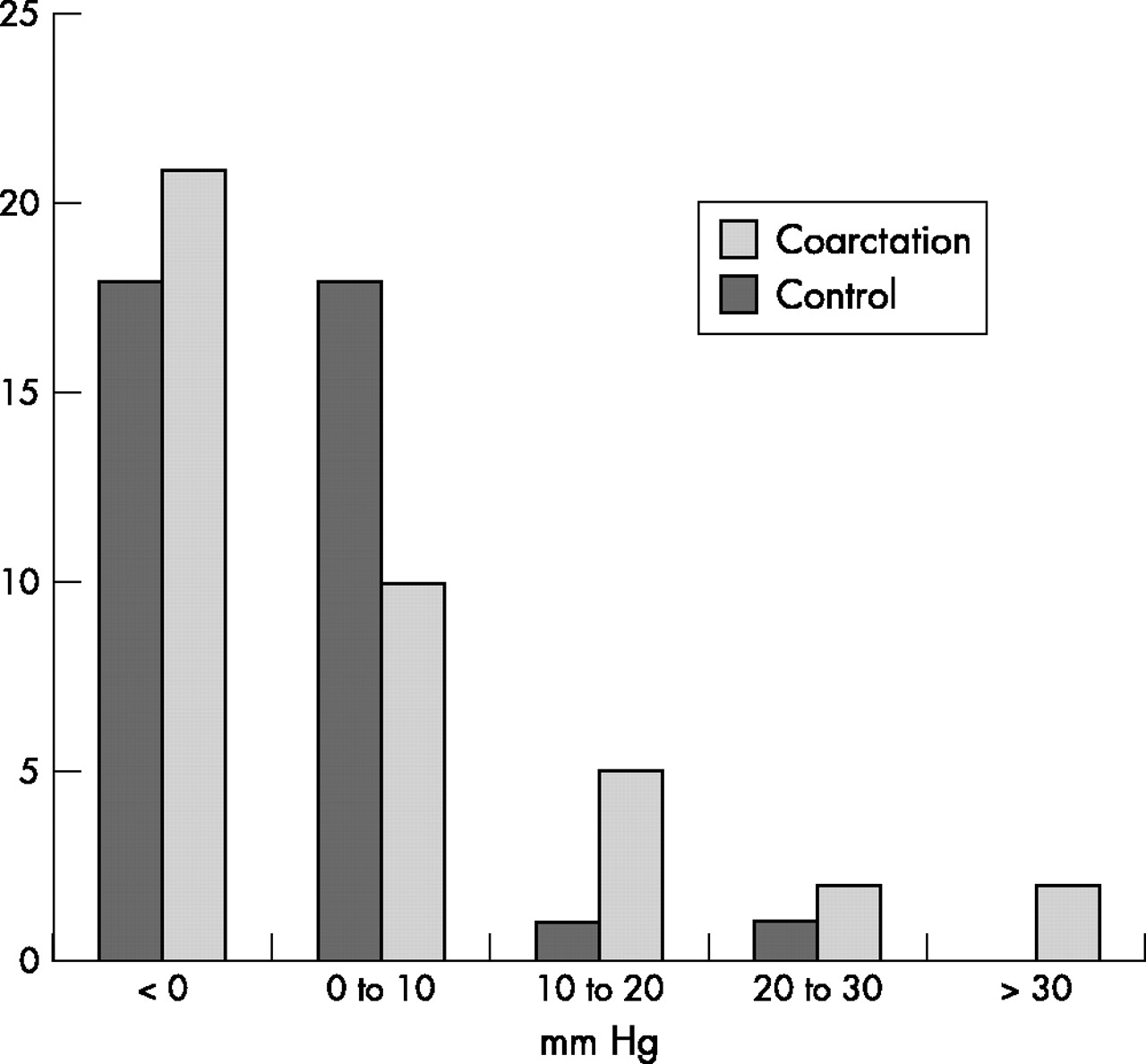
The mean arm–leg systolic blood pressure gradient was 3.6 (12.7) mm Hg in the patient group and −2.2 (8.0) mm Hg in the control group (p = 0.027). In 50% of the coarctation group and 30% of the control group, systolic blood pressure was higher in the right arm than in the leg (that is, there was a positive arm–leg gradient). This difference was more than 10 mm Hg in nine coarctation subjects and in two of the control subjects (fig 1).
{kind=link}
Resting arm–leg systolic blood pressure gradient (mm Hg).
The sensitivity and specificity of resting blood pressure variables in detecting a Doppler repair site gradient of more than 30 mm Hg are shown in table 2.
Sensitivity and specificity of resting blood pressure measurements
Exercise blood pressures
The coarctation subjects had a reduction in their exercise capacity (12.7 v 14.6 METs, p = 0.002) but no difference in peak exercise heart rates (177 v 183 beats/min, p = 0.1) when compared with controls. The majority of the patients, however, had a well preserved exercise capacity with the mean exercise time of 11 (2.6) minutes in the Bruce protocol.
Following exercise, the mean peak systolic arm blood pressure was 186.3 (37.5) mm Hg in the coarctation subjects, representing an increase of 57 (28.0) mm Hg (44% from baseline). Seven subjects (12.7%) had peak systolic pressures of ≥ 230 mm Hg, compared with none of the controls. However, there was no difference in peak exercise upper limb systolic blood pressure between the coarctation and control groups (186.3 v 178.5 mm Hg, p = 0.25). This was also true for diastolic blood pressures (71.5 v 69.6 mm Hg, p = 0.45). Following exercise, the mean arm–leg systolic blood pressure gradient was significantly higher in the coarctation cohort (50.4 v 25.9 mm Hg, p = 0.001) (table 1).
In the patient group, peak exercise systolic blood pressure correlated with simple anthropometric measurements (body mass index: r = 0.46, p = 0.002) and with resting blood pressure (r = 0.69, p < 0.001). It did not, however, correlate with either repair site gradient (r = 0.14, p = 0.39) or left ventricular mass (r = 0.18, p = 0.28).
Echocardiography
Repair site gradient
The mean repair site gradient, measured by transthoracic echo, was 18.9 (11.6) mm Hg. Eight subjects (14%) had resting repair site gradients of more than 30 mm Hg. Repair site gradient did not correlate with age at follow up (r = −0.3, p = 0.06), years since initial surgery (r = 0.1, p = 0.55), or height (r = 0.27, p = 0.1).
Resting systolic blood pressure (r = 0.3, p = 0.03) and resting arm–leg gradient (r = 0.47, p = 0.002) were positively correlated with repair site gradient (table 3). However, there was no relation with either resting diastolic blood pressure (r = −0.03, p = 0.84) or peak exercise systolic blood pressure (r = 0.13, p = 0.4). During recovery, arm–leg gradients were significantly related to the Doppler gradient (r = 0.38, p = 0.02), unlike peak exercise values (r = 0.19, p = 0.24) (table 2). The positive association between arm–leg gradients and repair site gradients persisted even following correction for age and body mass index (rest, r = 0.38, p < 0.05; recovery, r = 0.37, p < 0.05).
Correlations with repair site gradient on echocardiography and resting arm–leg gradient
Left ventricular mass
The mean left ventricular mass in the coarctation cohort was 170 (50.9) mm Hg. Left ventricular mass corrected for height and weight (LVMcorr) did not correlate with age at repair (r = −0.14, p = 0.45), systolic blood pressure (r = −0.007, p = 0.96), diastolic blood pressure (r = 0.08, p = 0.66), pulse pressure (r = −0.04, p = 0.83), repair site gradient (r = 0.11, p = 0.52), or peak exercise systolic blood pressure (r = −0.21, p = 0.23).
Aortic root dimensions
In the coarctation cohort, aortic root dimensions were related to height (r = 0.44, p = 0.006) and age at follow up (r = 0.56, p < 0.001). An aortic root diameter of ≥ 35 mm was present in 10 subjects (22%) but only one subject had a root of 40 mm or more. When root measurements were corrected for the influence of height there remained a relation between age at follow up (r = 0.58, p < 0.001) but not with years since surgical repair (r = 0.28, p = 0.08). Subjects with a bicuspid aortic valve had a slightly increased aortic root diameter but this did not reach significance (31.3 v 29.0 mm, p = 0.07).
Aortic root size also correlated with resting systolic blood pressure (r = 0.42, p = 0.008) but not with arm–leg systolic pressure gradient (r = 0.09, p = 0.59). The relation between root size and age was not explained by this blood pressure association (r = 0.5, p = 0.001 following correction for resting systolic blood pressure and height), suggesting a progressive increase in aortic root size that was not fully explained by changes in body morphology or blood pressure.
DISCUSSION
There is ongoing controversy regarding the extent and significance of abnormal exercise blood pressures in patients with repaired coarctation of the aorta. Several studies have suggested an exaggerated exercise systolic blood pressure response and advocated the routine use of exercise testing.7 However, there have been few large controlled investigations of exercise blood pressures in adults with repaired coarctation, and questions have been raised over the value of stress testing.8 Leandro and colleagues9 were unable to show that coarctation patients had an increased peak exercise blood pressure compared with controls—a finding previously reported in the paediatric literature.5 Our study confirms that finding, with no significant difference in peak exercise systolic blood pressure compared with our control group, despite a difference in resting blood pressures. These findings call into question the role of exercising these individuals to identify “latent hypertension”.
Although there are interesting questions over the significance of exercise blood pressure profiles and their relation to outcome and end organ damage, these are of secondary importance if a simple difference over a control cohort cannot be reliably proven. If exercise testing were to be advocated one would need to establish: first, what the test is actually assessing; second, what constitutes a pathophysiologically abnormal response; and third, whether specific treatment of the abnormality has an impact on morbidity and mortality. Treatment with β blockers reduces exercise upper limb systolic blood pressure,10 but only if it could be shown that there was a link with adverse outcome would there be justification for giving treatment that might reduce episodes of exaggerated vascular wall stress. At present the balance of evidence is such that exercise blood pressures cannot be used to guide management in this group of patients.
In this study we made some attempt to assess the value of exercise testing in detecting recoarctation. The use of Doppler echocardiography, rather than a gold standard of invasive measurements, limits the conclusions that can be drawn. However, peak exercise systolic blood pressure did not contribute to the identification of individuals with an increased repair site gradient on echocardiography or those with a positive arm–leg systolic blood pressure gradient. Although these are simply surrogates for true repair site gradient, they may help to identify patients who are at risk of restenosis. The diagnosis of recoarctation is difficult clinically. Resting blood pressures and arm–leg gradients may be relatively more informative than exercise indices, but these simple measurements are insufficiently sensitive or specific to exclude recoarctation. The use of other imaging modes, such as magnetic resonance imaging, is essential and may be more cost–effective.11
This study highlights a further area of interest, aortic root dilatation. In this cross sectional study aortic root diameter was related to age at the time of follow up—a relation that was not dependent on body size or blood pressure. The histology of the aorta proximal to the coarctation site is known to be abnormal, particularly in the setting of bicuspid valve disease,12 and a prospective study is needed to determine if these results are a manifestation of progressive ascending aortic dilatation in this setting.
Conclusions
Exercise testing may have a role in assessing patients with coarctation—for example, by quantifying exercise capacity and detecting ST segment change—but at present exercise systolic blood pressures are of limited diagnostic value. Our study suggests that exercise systolic blood pressures, in particular peak exercise systolic upper limb blood pressure, are not informative variables either in their difference from controls or in their relation to increased repair site gradient.
Although the goal posts are now changing in the follow up and risk stratification of these patients,13 the early diagnosis of hypertension and “vascular dysfunction” must remain a lynch pin of the management of these patients, who are at risk from future cardiovascular events. With time new non-invasive markers of vascular risk, such as pulse wave velocity, will become available. In the interim, time and attention need to be focused on well proven outcome variables. Until a large and perhaps multicentred study answers the questions documented above, the indiscriminate use of exercise testing for this indication should be discouraged.