Article Text

Abstract
Objective: To characterise the effects of acetylcholinesterase inhibition with pyridostigmine on parasympathetic tone in patients with chronic heart failure (CHF).
Design: Prospective randomised, double blind crossover trial.
Setting: University hospital outpatient heart failure clinic.
Patients: 20 ambulatory subjects with stable CHF (mean age 55 years, mean ejection fraction 24%).
Interventions: Oral administration of a single dose of pyridostigmine 30 mg and matching placebo on separate days.
Main outcome measures: Heart rate recovery at one minute and three minutes after completion of maximal exercise.
Results: Heart rate recovery at one minute after exercise was significantly greater after administration of pyridostigmine than after administration of placebo (mean (SEM) 27.4 (3.2) beats/min v 22.4 (2.4) beats/min, p < 0.01). Heart rate recovery at three minutes after exercise did not differ after administration of pyridostigmine and placebo (mean (SEM) 44.4 (3.9) beats/min v 41.8 (3.6) beats/min, NS). Peak heart rate, peak oxygen uptake, peak respiratory exchange ratio, plasma noradrenaline (norepinephrine) concentrations, and plasma brain natriuretic peptide concentrations did not differ after administration of pyridostigmine and placebo.
Conclusions: Acetylcholinesterase inhibition with pyridostigmine increased heart rate recovery at one minute but not at three minutes after exercise. A specific effect of pyridostigmine on heart rate one minute after exercise suggests that pyridostigmine augments parasympathetic tone in patients with CHF.
- autonomic nervous system
- parasympathetic nervous system
- autonomic agents
- exercise physiology
- BNP, brain natriuretic peptide
- CHF, chronic heart failure
- NYHA, New York Heart Association
- V̇co2, carbon dioxide production
- V̇E, ventilation
- V̇ o 2
- oxygen uptake
Statistics from Altmetric.com
- BNP, brain natriuretic peptide
- CHF, chronic heart failure
- NYHA, New York Heart Association
- V̇co2, carbon dioxide production
- V̇E, ventilation
- V̇ o 2
- oxygen uptake
Abnormalities in neuroendocrine regulation are thought to be important determinants of long term morbidity and mortality in patients with chronic heart failure (CHF).1 Among the major manifestations of neuroendocrine dysregulation are profound abnormalities in autonomic control, characterised by sympathetic overactivity and parasympathetic withdrawal.2–5 Inhibition of sympathetic overactivity with β adrenergic receptor blocking agents improved survival in clinical trials in patients with CHF but there are few previous clinical investigations of parasympathomimetic agents in heart failure populations.6–10
Acetylcholinesterase inhibitors increase parasympathetic neurotransmission through inhibition of the enzymatic breakdown of acetylcholine at cholinergic receptor sites in the autonomic nervous system. Pyridostigmine is a short acting, reversible acetylcholinesterase inhibitor used in the treatment of myasthenia gravis. Since CHF is characterised by withdrawal of parasympathetic tone, cholinesterase inhibition may restore autonomic balance with augmentation of parasympathetic neurotransmission. The effects of pyridostigmine on the parasympathetic nervous system in patients with CHF have not been previously reported.
Rapid deceleration of heart rate within the first minute after peak exercise is regulated primarily by reactivation of the parasympathetic nervous system.11,12 An attenuated decrease in the heart rate during the first minute of recovery after graded exercise has been previously described in patients with heart failure and is strongly associated with subsequent mortality risk in subjects with and without cardiovascular disease.13–17 Whether pharmacological modulation of parasympathetic function can effect changes in heart rate recovery after exercise is unknown.
Accordingly, the current study was undertaken to determine prospectively the acute effects of a single dose of oral pyridostigmine on parasympathetic function as assessed by measurement of heart rate recovery one minute after maximal exercise in ambulatory patients with stable CHF in a randomised, double blind, placebo controlled crossover trial. We hypothesised that augmentation of parasympathetic neurotransmission with pyridostigmine would increase early heart rate recovery after maximal exercise when compared with placebo.
METHODS
Study population
Eighteen men and two women with CHF were studied. Subjects between 21–75 years of age with CHF of more than three months’ duration, stable New York Heart Association (NYHA) functional class I to III symptoms for at least two months, and left ventricular ejection fraction ≤ 40% (determined by radionuclide angiography or echocardiography) were eligible for the study. Criteria for exclusion were history of potential contraindications to cholinergic stimulation (asthma, glaucoma, urinary retention), atrial fibrillation, sick sinus syndrome, previous implantation of a permanent pacemaker, acute coronary or cerebral vascular events within the past year, diabetes mellitus with peripheral neuropathy, systolic blood pressure < 90 or > 160 mm Hg, resting heart rate < 50 or > 100 beats/min, serum sodium < 135 mmol/l, serum creatinine > 220 μol/l, liver function tests more than three times the upper limit of normal, and exercise limited by angina or non-cardiac comorbid conditions. Subjects were treated with stable doses of diuretics, digoxin, angiotensin converting enzyme inhibitors, and β adrenergic receptor antagonists for at least two months before the study. The study protocol complied with the Declaration of Helsinki and was approved by the institutional review board at Columbia Presbyterian Medical Center. All subjects gave written informed consent before participation.
Maximal exercise testing
Eligible subjects performed symptom limited maximal exercise on an electronically braked bicycle ergometer (n = 2) or treadmill (n = 18) on each study day. After a symptom limited peak work rate was achieved, exercise was immediately stopped and subjects rested in a seated position. Heart rhythm was recorded continuously (Cambridge Heart 2000, Bedford, Massachusetts, USA) during exercise and recovery. The magnitude of heart rate recovery was calculated as the difference between the peak exercise heart rate and the heart rate (derived from the average of the RR interval of five consecutive sinus beats) recorded at one minute and three minutes during passive recovery. Oxygen uptake (V̇o2), carbon dioxide production (V̇co2), and ventilation (V̇E) were determined with expired gas analysis (Sensormedics, Yorba Linda, California, USA) at rest and during exercise. Respiratory exchange ratio, ventilatory anaerobic threshold, and V̇E–V̇co2 slope were derived from gas exchange data with standard analyses. A high V̇E–V̇co2 slope was defined as a ratio > 34. Peak V̇o2 was defined as the average V̇o2 achieved in the last 30 seconds of exercise.
Neurohormonal analysis
An indwelling catheter for blood sampling was placed into a medial antecubital vein for venous blood sampling. Five millilitres of blood was obtained in a quiet darkened room after a 30 minute rest period with subjects in a supine position 160 minutes after drug administration and immediately after completion of the peak exercise test. Plasma was separated by cold centrifugation and stored at −80°C. Plasma brain natriuretic peptide (BNP) was measured with a calibrated automated quantitative fluorescent sandwich immunoassay device (Biosite Diagnostic, San Diego, California, USA).18 Plasma noradrenaline (norepinephrine) was measured with a high performance liquid chromatography method (ESA, Inc, Chelmsford, Massachusetts, USA) in the Yale Clinical Research Center Laboratory.
Study design
This was a prospective, double blind, randomised crossover study of pyridostigmine versus placebo. The study drug consisted of a single oral dose of 30 mg of pyridostigmine or matching placebo prepared by the Columbia Presbyterian Medical Center Research Pharmacy. The order of study drug administration was assigned by a blocked randomisation allocation method. The effects of study drug administration on heart rate recovery were determined on two study days separated by 7–10 days. Study procedures were identical on each study day. Subjects were studied in the postabsorptive state. Resting, exercise, and postexercise data were collected at 160–190 minutes after study drug administration (to correspond with anticipated peak plasma concentration after oral dosing).19 An investigator blinded to treatment assignment recorded the oxygen consumption at anaerobic threshold and at peak exercise, peak respiratory exchange ratio, and heart rate at rest, at anaerobic threshold, at peak exercise, and at one minute and three minutes during recovery.
Data analysis
All continuous variables are expressed as mean (SEM). The primary analysis was a comparison of the effect of study treatment assignment on heart rate recovery at one minute and three minutes during passive recovery after maximal exercise. Secondary analyses were comparisons of the effects of study drug treatment assignment on heart rate and mean arterial pressure at rest and at peak exercise, V̇o2 at anaerobic threshold and at peak exercise, and neurohormonal concentrations at rest and at peak exercise, and analyses of the effects of potential confounders and effect modifiers (NYHA functional class, background treatment with β adrenergic receptor antagonists or digoxin, and V̇E–V̇co2 slope) on the study drug treatment effect. Data were analysed in repeated measures analysis of variance models appropriate for the crossover design. The relation between baseline clinical variables and heart rate recovery was assessed with simple linear regression. For all analyses, a two tailed p < 0.05 was used to infer significance.
RESULTS
Clinical correlates of heart rate recovery
Table 1 lists the clinical characteristics of the study population. Heart rate recovery at one minute after exercise was significantly greater in subjects with NYHA class I–II heart failure than in subjects with NYHA class III heart failure (29 (3) beats/min v 13 (1) beats/min, p < 0.01) and was significantly greater in patients with normal V̇E–V̇co2 slope than in patients with high V̇E–V̇co2 slope (25 (3) beats/min v 14 (2) beats/min, p = 0.01). Heart rate recovery one minute after exercise was significantly associated with peak V̇o2 (r = 0.72, p < 0.01) and V̇E–V̇co2 slope during exercise (r = 0.62, p < 0.01). Heart rate recovery at one minute after exercise did not differ between patients with ischaemic heart failure and those with other aetiologies of heart failure and was not significantly associated with age or left ventricular ejection fraction.
Clinical characteristics of the 20 study patients
Effects of study drug at rest
Heart rate at rest was significantly decreased after pyridostigmine administration compared with placebo (65 (2) beats/min v 68 (2) beats/min, p < 0.05). Mean arterial blood pressure at rest did not differ after administration of pyridostigmine and placebo (82 (2) mm Hg v 82 (2) mm Hg, NS).
Effects of study drug on exercise performance
Heart rate, mean arterial pressure, oxygen consumption, respiratory exchange ratio, and V̇E–V̇co2 slope did not differ during exercise after administration of pyridostigmine and placebo (table 2).
Exercise performance variables at anaerobic threshold and during exercise after administration of pyridostigmine and placebo
Effects of study drug on postexercise heart rate recovery
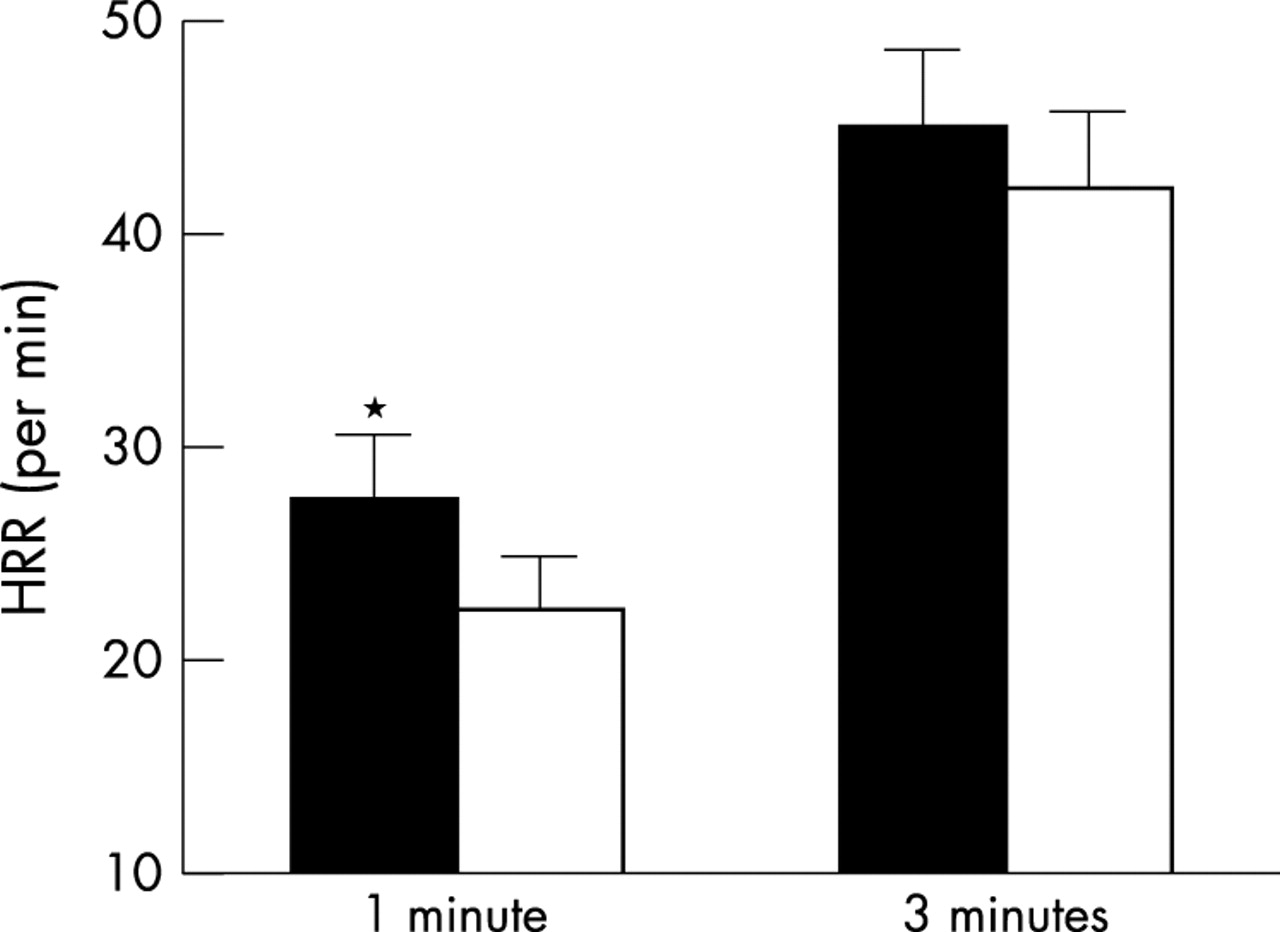
Heart rate recovery at one minute after peak exercise after administration of pyridostigmine was significantly greater than that after administration of placebo (27.4 (3.2) beats/min v 22.4 (2.4) beats/min, p < 0.01) (fig 1). Differences in heart rate recovery at one minute after peak exercise between pyridostigmine and placebo remained significant when adjusting for NYHA functional class, β blocker dose, digoxin use, and high V̇E–V̇co2 slope (all adjusted p < 0.01). NYHA functional class, dose of β adrenergic receptor antagonist, and digoxin use did not modify the effects of pyridostigmine on heart rate recovery one minute after peak exercise (NS for interaction terms). The effect of pyridostigmine on heart rate recovery one minute after peak exercise tended to be greater in subjects with normal V̇E–V̇co2 slope (difference for treatment groups 7.1 (2.3) beats/min) than in subjects with high V̇E–V̇co2 slope (difference for treatment groups 2.6 (1.3) beats/min, p = 0.17 for interaction term). Heart rate recovery at three minutes after peak exercise after administration of pyridostigmine and placebo did not differ (44.4 (3.9) beats/min v 41.8 (3.6) beats/min, NS) (fig 1).
{kind=link}
Heart rate recovery (HRR, beats/min, mean with error bar indicating positive SEM) at one minute and three minutes after maximal exercise in 20 subjects with chronic heart failure after treatment with pyridostigmine (solid bars) or placebo (open bars). *p<0.01 v placebo.
Neurohormonal effects of study drug
Plasma BNP and plasma noradrenaline concentrations were significantly greater at peak exercise than at rest (p < 0.05) (table 3). Plasma BNP and plasma noradrenaline concentrations at rest and at peak exercise did not differ after administration of pyridostigmine and placebo (table 3).
Plasma brain natriuretic peptide and noradrenaline concentrations at rest and at peak exercise after administration of pyridostigmine and placebo
Tolerability of study drug
The study drug was well tolerated in all subjects. No signs or symptoms of cholinergic excess or other adverse events were observed. PR, QRS, and QTc intervals did not differ on resting ECGs obtained 160 minutes after administration of pyridostigmine and placebo.
DISCUSSION
The central finding of this study is that acetylcholinesterase inhibition with a single dose of 30 mg of pyridostigmine acutely increased heart rate recovery at one minute after maximal exercise in patients with stable CHF when compared with placebo.
Pyridostigmine is a reversible acetylcholinesterase inhibitor used in the treatment of myasthenia gravis at typical daily doses ranging from 240–480 mg. The pharmacological action of pyridostigmine is attributable to inhibition of the enzymatic breakdown of acetylcholine and consequent potentiation of cholinergic neurotransmission. The effects of pyridostigmine on cardiovascular function have been previously reported in normal subjects and patients with coronary artery disease and hypertension. Administration of single doses of 30–45 mg of pyridostigmine was associated with a 28% reduction in serum cholinesterase activity and decrease in resting heart rate of 5–7 beats/min in normal subjects and patients with cardiovascular disease.20–22 Pyridostigmine at these doses was well tolerated and was not associated with changes in heart rate during exercise or in response to mental stress, changes in arterial pressure, or changes in ventilatory or neuromuscular function.22–24
Increased heart rate during progressive exercise is regulated by concomitant attenuation of parasympathetic activation and augmentation of sympathetic activation.2 Rapid deceleration of heart rate in the first minute after exercise is effected primarily by postexercise reactivation of the parasympathetic nervous system.2,11,12 The mechanisms for rapid reactivation of vagal tone immediately after exercise cessation are not fully characterised but are thought to be mediated in part by release of central inhibition and increased ventilatory tidal volumes at peak exercise.11,25 Withdrawal of sympathetic activation does not appear to have an important role in modulation of early heart rate recovery.11,12,26,27 The current findings of an increase in the magnitude of heart rate recovery at one minute of recovery but not at three minutes of recovery after administration of pyridostigmine are consistent with a specific augmentation of parasympathetic tone. A specific effect on parasympathetic tone is also supported by our finding that pyridostigmine decreased heart rate at rest when compared with placebo but not at anaerobic threshold or at peak exercise. Evidence of a borderline significant interaction effect with V̇E–V̇co2 slope is also consistent with a specific augmentation of parasympathetic tone, as pretreatment parasympathetic tone is greater in patients with normal V̇E–V̇co2 slope than in patients with high V̇E–V̇co2 slope.28,29 The lack of effect on plasma noradrenaline concentrations at rest or at peak exercise when compared with placebo suggests that the effects of pyridostigmine on heart rate recovery were not mediated by suppression of sympathetic activation.
Early heart rate recovery, as assessed by the exponential time constant of heart rate deceleration in the first 30 seconds after exercise and by frequency domain analysis of heart rate variability, is impaired in subjects with CHF when compared with normal subjects.11,25 Parasympathetic tone at rest, as assessed by time and frequency domain analyses of heart rate variability and baroreceptor sensitivity, is also decreased in subjects with heart failure when compared with normal subjects.2,4,30,31 Our findings are consistent with these previous studies and show that heart rate recovery is related to functional class, peak aerobic capacity, and V̇E–V̇co2 slope. The observed association between heart rate recovery and these variables is in accord with previous reports that showed that baroreceptor sensitivity was closely related to functional status and V̇E–V̇co2 slope in patients with CHF.28–30
Pharmacological modulation of parasympathetic function with scopolamine has been previously reported in subjects with heart failure. In contrast to pyridostigmine, which augments parasympathetic tone by inhibiting breakdown of endogenously released acetylcholine, scopolamine has dual effects on autonomic function that are dependent on the administered dose. At low dose scopolamine has a central vagomimetic effect, whereas at high dose scopolamine has a peripheral anticholinergic action. In patients with mild to moderate heart failure, short term courses of low dose scopolamine applied transdermally increased time domain and frequency domain indices of resting heart rate variability and improved baroreceptor sensitivity without an effect on exercise tolerance or the incidence and severity of ventricular arrhythmias.9,10,32 Practical long term administration of scopolamine has been limited by its narrow therapeutic range and consequent potential for anticholinergic side effects.9
An attenuated decrease in the heart rate during the first minute of recovery after peak exercise is strongly associated with subsequent mortality risk, independently of peak exercise workload, the presence or absence of myocardial perfusion defects, and peak heart rate in patients referred for clinical exercise testing.13–17 In patients with heart failure, autonomic dysfunction, as assessed by baroreceptor sensitivity and heart rate variability, is associated with increased mortality risk.30,31 Since the reported estimated slope of the relation between heart rate recovery and mortality risk in previous clinical studies was steep,13,15,17 relatively small changes in heart rate recovery, such as those observed in response to pyridostigmine in the current study, may potentially be associated with clinically important reductions in mortality risk.
In conclusion, augmentation of parasympathetic tone with 30 mg of pyridostigmine in patients with stable CHF was well tolerated and significantly increased the heart rate recovery in the first minute after maximal exercise when compared with placebo. Since heart rate recovery is an independent predictor of mortality in patients with cardiovascular disease, further studies to assess long term safety and efficacy of pyridostigmine in heart failure are warranted.
Acknowledgments
We gratefully acknowledge the assistance received from Dr Ary L Goldberger and staff of the NIH/NCRR Research Resource for Complex Physiologic Signals at Beth Israel Deaconess Medical Center, Boston, Massachusetts, USA in analysis of the heart rate recovery data and review of the manuscript. Supported in part by Division of Research Resources, Core Lab Facility in the General Clinical Research Center at Yale University, NIH, 5 MO1 RR00125, American Heart Association (Heritage Affiliate) Post-doctoral Fellowship Award (SA), and NHLBI grant HL K24–04024 (SDK)