Article Text

Abstract
Objective: To evaluate the ability of colour Doppler transoesophageal echocardiography (TOE) to assess quantitatively prosthetic mitral valve insufficiency.
Methods: 47 patients were studied with multiplane TOE and cardiac catheterisation. Proximal jet diameter was measured as the largest diameter of the vena contracta. Regurgitant area was measured by planimetry of the largest turbulent jet during systole. Flow convergence zone was considered to be present when a localised area of increased systolic velocities was apparent on the left ventricular side of the valve prosthesis. Pulmonary vein flow velocity was measured at peak systole and diastole.
Results: Mean (SD) proximal jet diameter was 0.63 (0.16) cm, with good correlation with angiographic grades (r = 0.83). Mean (SD) maximum colour jet area was 7.9 (2.5) cm2 (r = 0.69) with worse correlation if a single imaging plane was used for measurements (r = 0.62). The ratio of systolic to diastolic peak pulmonary flow velocity averaged 0.7 (1.3) cm (r = −0.66) with better correlation (r = −0.71) if patients with atrial fibrillation were excluded. Mean (SD) regurgitant flow rate was 168 (135) ml/s and regurgitant orifice area was 0.56 (0.43) cm2, with good correlation with angiography (r = 0.77 and r = 0.78, respectively).
Conclusions: TOE correctly identified angiographically severe prosthetic mitral regurgitation, mainly by the assessment of the flow convergence region and the proximal diameter of the regurgitant jet.
- transoesophageal echocardiography
- colour Doppler echocardiography
- mechanical valve prosthesis
- prosthetic mitral regurgitation
- valvar heart disease
- LAA, left atrial area
- MRA, mitral regurgitant area
- Qmax, maximum instantaneous regurgitant flow
- ROA, regurgitant orifice area
- TOE, transoesophageal echocardiography
- va, aliasing velocity
- vp, peak regurgitant velocity
Statistics from Altmetric.com
- transoesophageal echocardiography
- colour Doppler echocardiography
- mechanical valve prosthesis
- prosthetic mitral regurgitation
- valvar heart disease
- LAA, left atrial area
- MRA, mitral regurgitant area
- Qmax, maximum instantaneous regurgitant flow
- ROA, regurgitant orifice area
- TOE, transoesophageal echocardiography
- va, aliasing velocity
- vp, peak regurgitant velocity
Prosthetic valve regurgitation is a potentially life threatening complication after valve replacement; therefore, its early and correct detection is of great importance. Since transthoracic colour Doppler echocardiography often fails to show or underestimates the regurgitant jet within the left atrium because of shadowing of the prosthesis, transoesophageal echocardiography (TOE) has gained significant interest.1–7 Although transoesophageal Doppler methods for evaluation of the severity of native or bioprosthetic mitral regurgitation have been described and clinically validated,8,9 data are lacking for mechanical prosthetic mitral regurgitation. The purpose of this study was to evaluate the ability of colour Doppler TOE to assess quantitatively mechanical prosthetic mitral valve insufficiency.
METHODS
Population
Forty seven patients with clinically suspected prosthetic valve dysfunction, endocarditis, or embolism were studied. Sixteen patients had a Björk-Shiley valve, 13 a Carbomedics valve, three a Medtronic-Hall valve, and 15 a St Jude valve. Thirty nine patients had a mitral valve prosthesis only, and eight had both mitral and aortic valve prostheses. Nineteen patients were in New York Heart Association functional class II, 20 were in class III, and eight were in class IV. Associated clinical conditions were haemolysis (four patients), infective endocarditis (four patients), and thromboembolism (two patients). Twenty six patients had normal sinus rhythm and the remaining 21 had atrial fibrillation. They were being treated with digitalis and diuretics (26 patients), vasodilators (18 patients), oral anticoagulants (24 patients), and heparin (5 patients). The median interval from prosthetic valve implantation was 8 (12) years. All patients gave written informed consent to both TOE and cardiac catheterisation. All of them had transoesophageal two dimensional images and colour Doppler data of adequate quality to permit Doppler quantification of cardiac mitral inflow, regurgitant flow spectra, and proximal flow convergence zone.
Transoesophageal echocardiography
TOE was performed with a commercially available 5 MHz, 128 element, multiplane machine (Powervision 8000, Toshiba Corp, Tokyo, Japan). After intubation, during the examination of mitral regurgitation, the patient’s cuff blood pressure and heart rate were recorded. Colour gain was adjusted by increasing gain up to the appearance of random colour pixels and then slightly reducing it. Scanning plane orientation was mechanically changed from 0° (transverse, parallel to the coaptation line of prosthesis) continuously to 90° (longitudinal) and further to 180° (transverse with left to right inversion).
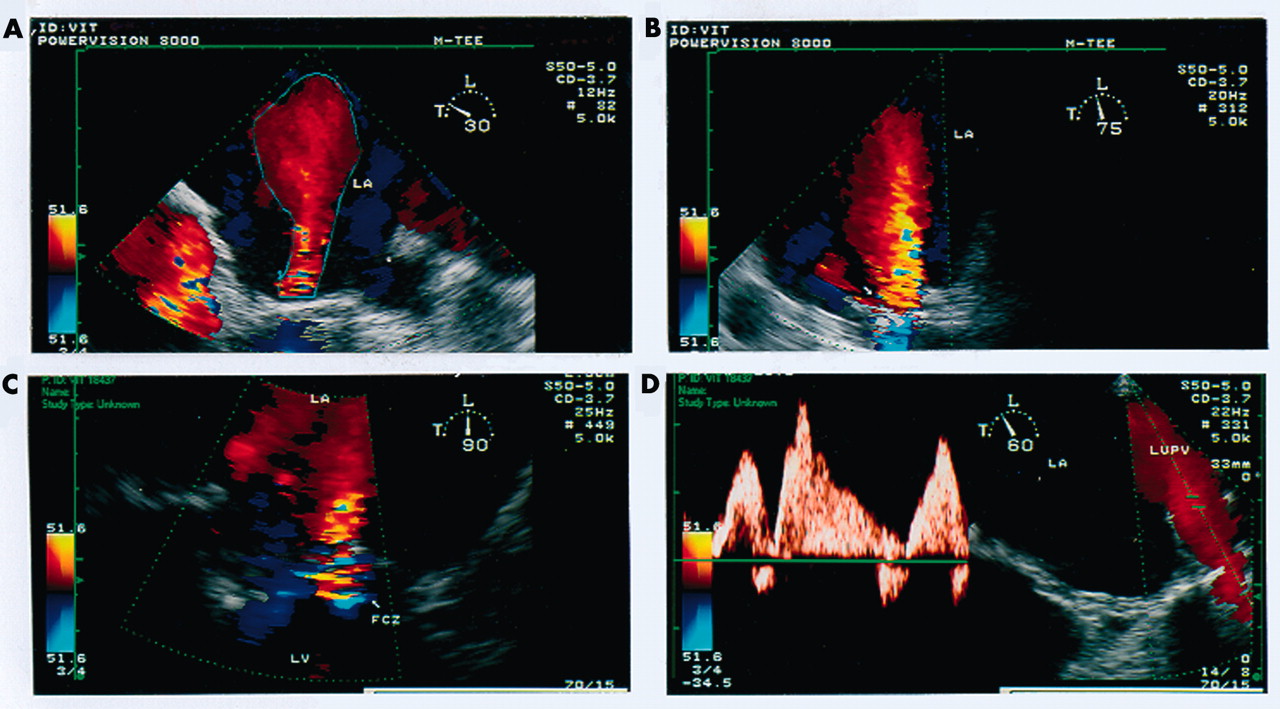
The following parameters were determined: colour jet regurgitant area, proximal jet diameter, flow convergence zone, and left upper pulmonary vein flow velocity (fig 1).

Examples of colour jet mitral regurgitant area (MRA), proximal jet diameter (PJD), flow convergence zone (FCZ), and pulmonary vein flow (PVF) velocities in a patient with mitral valve prosthesis. (A) Planimetry of colour jet MRA and left atrial area (LAA). (B) Regurgitant colour jet measured at its origin (arrow indicates PJD). (C) FCZ visualised as a blue flow pattern of increasing brightness with a yellow-red central region (aliased velocities). (D) Left upper PVF velocity pattern in systole and diastole. LA, left atrium; LUPV, left upper pulmonary vein; LV, left ventricle.
Mitral regurgitant area (MRA) was measured by planimetry of the largest turbulent jet during systole searching for the largest representation of the jet throughout the entire 180° arc. The ratio of MRA to left atrial area (MRA:LAA) was determined.
Proximal jet diameter was measured as the largest diameter of the vena contracta in each view during any portion of systole. The vena contracta was considered to be the narrowest region of the jet as it emerged through the prosthetic closure.
The flow convergence zone was considered to be present when a localised area of increased velocities (distinct and focal brightening of colour) or colour aliasing (multicolour or mosaic) of velocities was apparent on the left ventricular side of the mitral valve prosthesis during systole. This was imaged by searching the plane with the best and largest delineation of an approximately hemispheric proximal convergence zone, narrowing the colour mapping sector to a minimum. Since the left ventricular side of the mechanical prosthesis is partially obscured from the transoesophageal window, particular care in the search was taken by manipulating the gain and scan plane. The colour bar zero line was shifted in the direction of regurgitant flow to maximise the radius from the regurgitant orifice to the first aliasing point while preserving the hemispheric shape of the convergence zone. The radial distance (r) between the first aliasing contour (red-blue interface) and the centre of the regurgitant orifice was measured at the time of the largest convergence image. Maximum instantaneous regurgitant flow (Qmax, in ml/s) was calculated as Qmax = 2πr2va, where r (in cm) is the maximum distance to the contour of aliasing velocity va (in cm/s) with a hemispheric contour assumed. The regurgitant orifice area (ROA, in cm2) was determined by dividing maximum flow by the peak regurgitant velocity (vp) obtained by continuous wave Doppler, where ROA = Qmax/vp.
Pulmonary vein flow velocity was measured at peak systole and peak diastole by sampling 1–2 cm inside the left upper pulmonary vein. The ratio of peak systolic to peak diastolic velocity was calculated.
The values of three and five measurements were averaged for patients with sinus rhythm and atrial fibrillation, respectively.
Cardiac catheterisation
Biplane left ventricular angiography was performed with 40–50 ml of iodinated contrast at flow rates of 10–12 ml/s within six days after the transoesophageal study. The angiographic severity of mitral regurgitation was graded according to a historically accepted grading scheme10,11 in four grades (I, II, III, and IV, from mild to severe). The left ventricular angiogram was interpreted at the time of catheterisation by experienced angiographers who reviewed the cinefilm without knowledge that the data would be analysed for the present study.
Surgery
In 18 patients (38%), the valve was subsequently inspected during surgery 12 (15) days (range 4–55 days) after TOE. The substrate for mitral regurgitation was considered to be present when a portion of the prosthetic disc or ball was significantly disrupted by abnormal material, when a definite periprosthetic fistula was identified, or when the prosthetic annulus was dehisced.
Statistical analysis
Data are presented as mean (SD). Linear regression analysis was used to compare continuous variables. Analysis of variance (Spearman coefficient) was used to compare differences in transoesophageal parameters between angiographic grades of mitral regurgitation. A probability value of p < 0.05 was considered significant. The sensitivity and specificity of jet diameter, colour jet area, flow convergence, and pulmonary vein flow velocity were calculated according to their ability to predict the presence of significant (> 2) mitral incompetence during left ventriculography. Receiver operating characteristic curves of echocardiographic indices were tested with use of a maximum likelihood estimation approach for differences.12 Interobserver variability was determined in 20 randomly selected cases with measurements obtained independently by two observers. Intraobserver variability was also calculated by repeating measurements one month after the initial measurement.
RESULTS
Table 1 lists echocardiographic, angiographic, and surgical characteristics of patients. Of the initial 52 patients, five were excluded because of insufficient image quality, which precluded either reliable measurement of the proximal jet width (one patient) or use of flow convergence zone (four patients). Forty seven patients were included in the study. Six patients (13%) had angiographic regurgitation grade I, 16 patients (34%) had grade II, 11 patients (23%) had grade III, and 14 patients (30%) had grade IV. Mean systemic blood pressure and heart rates were not significantly different during TOE and cardiac catheterisation (mean blood pressure 107 (11) mm Hg v 100 (12) mm Hg, respectively, not significant; heart rate 96 (16) beats/min v 98 (13) beats/min, respectively, not significant).
Echocardiographic, angiographic, and surgical patient data
The mean (SD) maximum colour jet area was 7.9 (2.5) cm2 (range 0.9–12 cm2), with fair correlation (fig 2) with angiographic grades (r = 0.69) and worse correlation if a single imaging plane was used for measurements (r = 0.62). A similar correlation was found for MRA:LAA ratio (r = 0.71). Quantitative measurements of regurgitant jet area and MRA:LAA ratio obtained by different imaging planes were significantly different. By using 0° planes, the jet area was 6.2 (1.7) cm2 and MRA:LAA ratio was 17 (8)%; by 0° and 90° planes, jet area was 6.9 (2.1) cm2 and MRA:LAA was 25 (8)% (p < 0.05 v 0° planes); by using multiple imaging planes, jet area was 7.8 (2.9) cm2 and MRA:LAA ratio was 29 (10)% (p < 0.005 v 0° and 90° planes).

Plots of (A) MRA, (B) MRA:LAA, and (C) systolic to diastolic ratio of pulmonary vein flow velocity (PVF-S:D) on the y axis against angiographic grades of prosthetic mitral regurgitation on the x axis. The broken line represents cut off values for MRA of 7 cm2, MRA:LAA of 30%, and PVF-S:D ratio of −0.2, separating patients with and without severe prosthetic mitral regurgitation.
The ratio of systolic to diastolic peak pulmonary flow velocity averaged 0.7 (1.3) (range 2.3 to −2.9), with fair correlation (fig 2) with angiographic grades (r = −0.66) and better correlation (r = −0.71) if patients with atrial fibrillation were excluded.
The average proximal jet diameter was 0.63 (0.16) cm (range 0.3–1.3 cm), with good correlation (fig 3) with angiographic grades (r = 0.83). A jet width at its origin ⩾ 0.6 cm identified severe prosthetic mitral regurgitation in 26 of 27 patients (sensitivity 96%) and correctly predicted absence of severe prosthetic mitral regurgitation in 19 of 20 patients (specificity 95%). The correlation was independent of the jet spatial disposition (free jets or wall jets).

Plots of (A) maximum instantaneous regurgitant flow (Qmax), (B) regurgitant orifice area (ROA), and (C) proximal jet diameter (PJD) on the y axis against angiographic grades of prosthetic mitral regurgitation on the x axis. The broken line represents cut off values for Qmax of 200 ml/s, ROA of 0.45 cm2, and PJD of 0.6 cm, separating patients with and without severe prosthetic mitral regurgitation.
The average regurgitant flow rate was 168 (135) ml/s (range 25–757 ml/s), with good correlation (fig 3) with angiographic grades (r = 0.77). The average ROA was 0.56 (0.43) cm2 (range 0.19–1.8 cm2), with good correlation (fig 3) with angiographic grades (r = 0.78). This correlation was not modified by exclusion of patients with atrial fibrillation. A Qmax of 200 ml/s and ROA of 0.45 cm2 accurately separated patients with and without severe prosthetic mitral regurgitation.
The intraobserver variability was 6% for proximal jet diameter (mean (SD) 0.3 (1.8) cm), 7% for radius measurements (1.3 (0.7) cm), and 8% for Qmax (55 (15.1) ml/s). The interobserver variability was 7.5% for proximal jet diameter (1.7 (1.1) cm), 8% for radius measurements (1.8 (2.2) cm), and 10% for the Qmax (75 (17) ml/s).
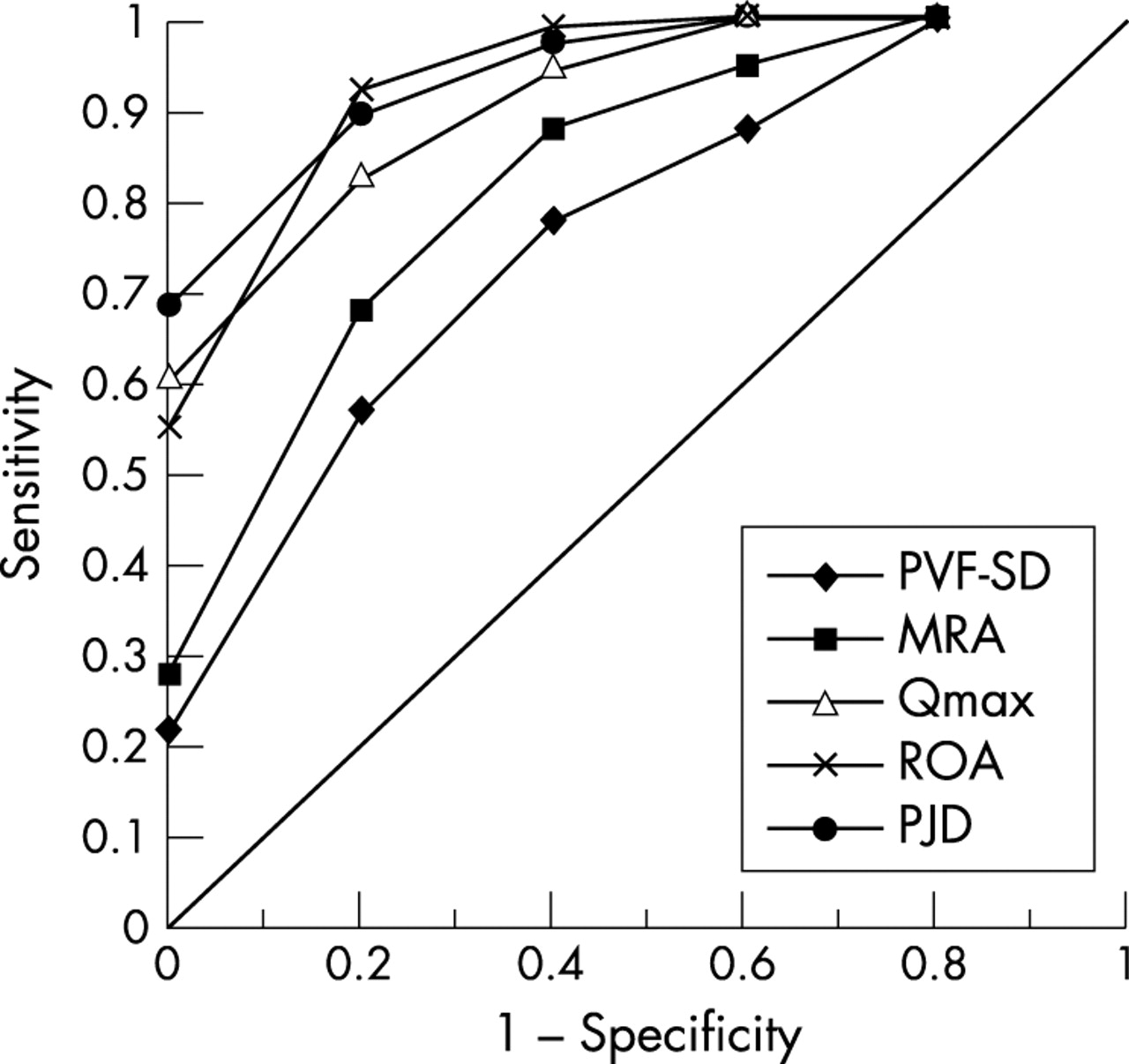
Figure 4 shows receiver operating characteristic curves of colour Doppler parameters for the detection of significant prosthetic mitral regurgitation. Table 2 lists sensitivity, specificity, and predictive values for the detection of significant regurgitation.
Sensitivity and specificity of transoesophageal echocardiographic (TOE) indices to identify angiographically severe prosthetic mitral valve regurgitation
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Comparison between the area under the curve (AUC) of the receiver operating characteristic curves obtained for the transoesophageal Doppler variables analysed: PVF-S:D (AUC 0.81), MRA (AUC 0.83), Qmax (AUC 0.93), ROA (AUC 0.93), and PJD (AUC 0.97). The variables more predictive of angiographically significant prosthetic mitral regurgitation are those with the highest AUC.
Among the 18 patients who had surgical inspection of their valves, the predominant lesion was paravalvar mitral regurgitation, which occurred with all four valve types. All of these patients had significant regurgitation during TOE and left ventriculography. In two patients with paravalvar insufficiency at surgery regurgitation was judged at TOE examination to be a peripheral transvalvar leakage (inside the sewing ring) instead of paravalvar (outside the sewing ring).
DISCUSSION
Quantitative assessment of prosthetic regurgitation
Previously only a few angiographically controlled studies comparing the diagnostic accuracy of transoesophageal Doppler methods in the grading of prosthetic mitral regurgitation have been undertaken.8,13 This study extends the value of TOE in the assessment of mechanical prosthetic mitral insufficiency by combining various methods for estimation of regurgitation severity. The abnormal regurgitant jets associated with prosthetic mitral valves can be central, through degenerated prosthetic leaflets, or paravalvar leaks. It would be most clinically relevant to examine the correlation of these abnormal jets with the angiographic grade, particularly of paravalvar jets, as they are difficult to quantify.
The indices derived from the flow convergence zone (Qmax and ROA) correlated well with angiographic severity grades, corroborating earlier transthoracic reports for prosthetic mitral regurgitation14–17 and transoesophageal reports for native mitral valve regurgitation.9,18 Since direct comparison between Doppler regurgitant stroke volume and invasively calculated regurgitant parameters showed an overestimation by Doppler, correction factors have been proposed to correct for an angled, non-planar geometry of the leaflets or discs19; however, the precise geometry of the convergence zone is difficult to determine with the current technology. A simplified proximal flow convergence method for calculating mitral ROA has been recently described.20
The proximal jet (vena contracta) had the highest correlations with angiographic severity grade. Vena contracta width is dependent on loading conditions21 as are methods that directly measure regurgitant volume, including proximal flow convergence, jet momentum, and quantitative Doppler,22–25 but is less technically demanding. Moreover, interobserver measurements of vena contracta width correlated closely in this study and others.18,26 Our cut off of 0.6 cm to differentiate mild to moderate valvar insufficiency from moderately severe to severe valvar insufficiency is in agreement with previous reports for native mitral valve regurgitation.9
Colour jet area had a fair discriminating power in this study, even if correlation with angiographic severity was improved by use of a multiplane scan and is much higher than in transthoracic reports where the severity can be greatly underestimated because of the phenomenon of flow masking behind prosthetic valves.15 Another potential limitation of Doppler colour flow imaging analysis of the jet area in the left atrium is the direction of the regurgitant jet itself. In patients with mechanical prosthetic mitral regurgitation, the regurgitant jet is often eccentric. Eccentricity can lead to underestimation of the grade of regurgitation as a result of the prosthetic regurgitant jet impinging on the left atrial walls.
The ratio of systolic to diastolic pulmonary venous flow correlated moderately with angiographic severity grade. This is not surprising given the multifactorial nature of pulmonary venous flow, which is also influenced by atrial and left ventricular function.27 The correlation is improved if patients with atrial fibrillation are excluded; thus, this method has important limitations, since patients with mitral valve regurgitation often have atrial fibrillation either permanently or intermittently. The presence of blunted or reversed systolic flow in pulmonary veins has been reported to be suggestive of significant mitral regurgitation in both native and prosthetic valves.28
Figure 4 shows receiver operating characteristic curves suggesting that the quantitative methods are an excellent test to distinguish grade I to II from grade III to IV. This implies that several candidate threshold values can be identified that have both good sensitivity and good specificity to separate grades. For example, for the threshold separating grade III from grade IV an ROA of 0.5 cm2 prioritised sensitivity but had a low specificity, and an ROA of 0.4 cm2 prioritised specificity with some loss in sensitivity. The final choice is to be made by each physician depending on the goals defined for routine clinical practice.
Study limitations
The capacity of left ventricular angiography to be an ideal and accurate reference method in validation studies is questionable.29 Angiography itself has significant limitations, including variability of the position of the catheter within the left ventricular cavity, volume and rate of injection of contrast medium, left atrial volume in which the regurgitant contrast is diluted, and the volume of forward flow that partly determines its clearance. However, one of its major merits is its historical use, which has created a clinical perception of the semiquantitative grading scale that is used to report angiographic degrees of mitral regurgitation. Therefore, left ventriculography is an essential tool for calibration of quantitative methods to define corresponding grading frameworks and to translate the perception of angiography to values reported by quantitative methods. Furthermore, in the 18 patients who had surgery, the transoesophageal and angiographic findings were confirmed. In those patients classified as having normal or mild regurgitation, the clinical course showed no evidence contradicting this classification.
The transoesophageal and cardiac catheterisation studies were not conducted simultaneously; thus, a change in loading conditions between echocardiography and ventriculography may account for some of the misclassifications between quantification and angiographic grade observed in this study. Despite a difference between systolic blood pressure at the time of echocardiography and angiography, the absolute difference was small and the haemodynamic conditions were clinically similar. In routine practice, these tests are rarely performed simultaneously and, despite possible changes in loading conditions, the interpretation of the non-simultaneous grading guides all clinical decisions.
Even under optimal conditions, flow convergence may be missed because of its small size or shadowing. In addition, normal flow through the left ventricular outflow tract may be confused with flow convergence. Because some mitral prostheses are tilted towards the outflow tract, increased velocities in that location are sometimes difficult to distinguish from left ventricular outflow and flow convergence near the anterior mitral annulus. Furthermore, a variety of technical factors inherent in the performance of Doppler colour flow imaging can influence the size of acceleration flow signals. Although small variations in colour gain do not produce any change in the regurgitant jet area, an excessive decrease in gain may produce a significant reduction in the acceleration flow area because of the elimination of lower velocities.
Since mitral leaflet or disc coaptation is not planar, the regurgitant jet may be tangential to the imaging plane and some errors in measurements can be made in transthoracic echocardiography as well in TOE. These potential problems may be overcome by three dimensional reconstruction of the vena contracta by multiplane TOE.
Clinical implications
Despite an overlap between angiographic grades, as expected in routine clinical practice, the diagnostic value of the quantitative transoesophageal variables is excellent, as shown by the receiver operating characteristic curves. The use of complementary methods to assess mitral regurgitation is particularly relevant for mechanical prostheses, where paravalvar eccentric leaks are common and quantification can be a challenge. The correlation of quantitative Doppler measures of the degree of prosthetic mitral regurgitation by angiographic grading provides grading ranges for the quantitative variables and allows an improved perception of the meaning and interpretation of the measured values. On this basis, patients with jet diameter > 0.6 cm, Qmax > 200 ml/s, and ROA > 0.45 cm2 are classified as having severe prosthetic mitral regurgitation. Additional criteria of mitral regurgitant jet area > 7 cm2 or MRA:LAA > 30% are less reliable but clinically useful in selected patients when flow convergence and vena contracta data are difficult to determine.
Conclusions
TOE correctly identified angiographically severe mechanical prosthetic mitral regurgitation, mainly by assessment of the proximal diameter of the regurgitant jet and flow convergence region, which reflect its effective ROA. Moreover, the estimation of severity of the prosthetic mitral regurgitation by absolute or relative jet area is improved by multiplane imaging views. Thus, TOE can be used instead of angiography to make the decision to proceed with surgical intervention.