Article Text

Abstract
Objective: To compare survival and adverse outcome of patients with non-valvar atrial fibrillation (NVAF) treated with or without warfarin.
Design: Record linkage method to identify patients with a previous hospital diagnosis of atrial fibrillation and to link these patients to international normalised ratio (INR) test results and mortality data.
Setting: Cardiff and the Vale of Glamorgan, Wales.
Main outcome measures: Mortality, specifically from ischaemic and thromboembolic events.
Results: 6108 patients were identified with NVAF, of whom 36.4% received warfarin. Mean survival in the warfarin and non-warfarin groups was 52.0 months and 38.2 months, respectively (p < 0.001), and 14.4 months (p < 0.001) after adjustment for confounding factors. Warfarin treated patients in the upper quartile of INR control had significantly longer survival (57.5 months) than did those in the lowest quartile of control (38.1 months, p < 0.001). The risk of stroke in the warfarin group when treated was lower than that in the non-warfarin group (relative rate (RR) 0.74, p < 0.001). The risk of death from ischaemic stroke was lower in the warfarin group (RR 0.43, p < 0.001). The risk of all ischaemic and embolic events in the warfarin group was lower when they were taking warfarin (RR 0.74, p < 0.001). The risk of bleeding in the warfarin group when treated was greater (RR 1.78, p = 0.001).
Conclusions: Patients with NVAF within the recommended target INR range of 2.0–3.0 survive longer and have reduced morbidity. Probably too few people are anticoagulated with warfarin in NVAF.
- AF, atrial fibrillation
- ICD-10, International classification of diseases, 10th revision
- INR, international normalised ratio
- NVAF, non-valvar atrial fibrillation
- RR, relative rate
- atrial fibrillation
- warfarin
- anticoagulation
- stroke
Statistics from Altmetric.com
- AF, atrial fibrillation
- ICD-10, International classification of diseases, 10th revision
- INR, international normalised ratio
- NVAF, non-valvar atrial fibrillation
- RR, relative rate
Non-valvar atrial fibrillation (NVAF) affects about 1% of the general population1 with the incidence increasing to 4.7% in people over the age of 65 years. NVAF is associated with a significant increase in morbidity and mortality, with a three- to fivefold increased risk of stroke.2,3
Randomised clinical trials have shown that anticoagulation with warfarin reduces the risk of stroke by up to two thirds.4,5,6,7,8,9,10 However, fewer than half of patients eligible for warfarin treatment actually receive it.11,12 Recent national initiatives such as the National Strategic Framework for the Elderly have included standards that aim at improving the proportion of NVAF patients at risk of stroke who receive anticoagulation.13,14
The pharmacokinetic profile of warfarin is complex9 and frequent monitoring is required to maintain patients with NVAF within the recommended international normalised ratio (INR) target range of 2.0–3.0. Mortality is increased among patients with NVAF who are outside the target range.14 Among patients treated with warfarin who are below the target range at the time of a stroke event, severity is greater and 30 day survival is reduced compared with patients at an INR greater than 2.0.15 Many factors have been reported as barriers to treatment with warfarin, including interactions between warfarin and other medications and foods, concerns over the risk of bleeding, and practical problems relating to frequent INR monitoring.16
The purpose of this study was to characterise the epidemiology of serious thromboembolic and bleeding events and mortality among patients with NVAF who were anticoagulated with warfarin compared with those who were not anticoagulated with warfarin in a large UK general population.
METHODS
Data sources
As has been described previously,17 three sets of routinely collected data were used: inpatient data from April 1995 to March 2000 containing a range of information including discharge diagnosis (International classification of diseases, 10th revision (ICD-10)), length of stay, and operative procedures (Classification of surgical operations and procedures, fourth revision); haematology laboratory reports dating from June 1995 to January 2002 containing details of INR monitoring test results (including any initiated by primary care providers); and mortality data derived from the Office of National Statistics from January 1995. These data records were linked both within and between the various data sets by probability matching algorithms to identify those records relating to the same patient.18
Participants
The study was conducted in Cardiff and the Vale of Glamorgan, a largely urban area of South Wales, UK, with a population of 424 000. The patients studied were those identified during the study period with a diagnosis of atrial fibrillation (AF) (ICD-10 rubric I48*) recorded on inpatient admission and with no record of heart valve procedures before AF. Patients with more than four INR recordings before or after their initial NVAF admission were assumed to have received oral anticoagulation in the form of warfarin. These patients constituted the warfarin group. We assumed that the remaining patients, the non-warfarin group, had not been maintained on warfarin.
Linear interpolation of INR values
To estimate the daily INR values between routine measurements, we assumed that the actual difference in INR between any two consecutive measurements was linear, and the data were interpolated accordingly.19 The level of coagulation control for each patient was assessed by the percentage of interpolated INR values within the target range of 2.0–3.0.
Selection and coding of clinical outcomes
Serious cardiovascular events, including acute myocardial infarction, pulmonary embolism, deep vein thrombosis, ischaemic stroke, and bleeding events, were characterised. Events were selected as being a primary diagnosis only on inpatient admissions; however, an event was recorded as such if a selected code was anywhere on the death record.
The epidemiology of stroke20 and heart disease21 has been described previously in the same population by similar methods.
Statistical analyses
The time origin for these analyses was the first identifiable inpatient diagnosis of AF. In addition to this index date for all patients, a second time origin was necessary for the group who received warfarin because they were not necessarily anticoagulated with warfarin immediately after the index diagnosis of AF. This allowed statistical comparisons to be made between the warfarin group when treated versus the non-warfarin group, as well as comparisons of the rate of events within the warfarin treated group while treated and untreated. A key assumption was that a patient in the warfarin group was considered to be untreated with warfarin if the clinical event occurred before the first INR reading or longer than 42 days after the final recorded INR reading (95% of INR readings were taken within 42 days of the previous reading). The effect of this assumption was tested in a sensitivity analysis that limited the period during which patients were assumed to be receiving warfarin to within 21 days of the previous test. Kaplan-Meier and Cox proportional hazards models were applied to characterise survival. The Cox proportional hazards models were adjusted for age, sex, and relative morbidity at baseline. The total number of days spent in hospital in the year before the index AF diagnosis was used as a proxy measure of morbidity at baseline. If a patient had one of the quantified events at death, this event was listed among the event rates in tables 1 and 2. Mean life expectancy is detailed rather than median because some of the survival curves did not always reach the 50th centile within the maximum five year window. Event rates were compared by multivariate logistic or Poisson regression models. For the comparison of event rates in the warfarin group when treated and not treated, the non-parametric sign test was applied.
Rates of the serious adverse events among patients with non-valvar atrial fibrillation when treated or untreated with warfarin
Comparison of relative rate of events for ischaemic stroke, thromboembolism, and bleeding in the W+ and NW groups
RESULTS
Identification of the NVAF study groups
Of 222 398 patients hospitalised during the study period 6247 patients with AF were identified. Of these 139 (2.2%) patients were excluded on the basis of a history of heart valve surgery; the remaining 6108 patients constituted the NVAF study group. Of the NVAF study group 2828 (46.3%) had an INR reading, with 2223 (36.4%) having five or more INR readings (the warfarin group). The 3885 (63.6%) patients with fewer than five INR readings were assumed to be untreated with warfarin (the non-warfarin group). Demographic characteristics differed between the warfarin and non-warfarin groups. The proportion of women was slightly lower in the warfarin group (46.9% v 55.4%). The elderly (age > 75 years) were less likely than younger patients (49%) to be treated with warfarin (27%); thus, for both men and women the mean age of warfarin treated patients was lower (men: 69.8 years v 73.6 years; women: 75.5 years v 80.7 years).
Ischaemic stroke
There were 631 strokes in the study population; 392 (62%) strokes occurred in the non-warfarin group and 481 (76%) strokes occurred when patients, from either group, were not being treated with warfarin. The risk of stroke was lower in the warfarin group when treated (4.61/100 person years) than in the non-warfarin group (6.23/100 person years, relative rate (RR) 0.74, p < 0.001). The risk of stroke was also lower in the warfarin group taking treatment (4.61/100 person years) than in the same group not taking treatment (6.36/100 person years, RR 0.72, p < 0.001). The risk of death from ischaemic stroke was lower in the warfarin group (2.39/100 person years v 5.51/100 person years, RR 0.43, p < 0.001), with the hospital admission rate for stroke being similar in both groups (2.70/100 person years v 2.86/100 person years, RR 0.95, p = 0.308).
Bleeding events
There were 202 bleeding events in the study population, of which 112 (55%) occurred when patients, from either group, were not being treated with warfarin. In the warfarin group, the risk of a bleeding resulting in hospitalisation was higher while treated with warfarin (2.76/100 person years) than in periods of non-treatment (1.07/100 person years, RR 0.39) and higher than in the non-warfarin group (1.54/100 person years, RR 1.78, p = 0.001) (table 2). The increased risk of a bleeding event appeared greatest in the oldest patients.
All ischaemic or thromboembolic events
There were 1076 ischaemic or thromboembolic events, including ischaemic stroke, specifically outlined above, of which 818 (76%) occurred while the patient was not receiving anticoagulation. Patients in the warfarin group who were treated had a significantly lower event rate of 7.92/100 person years than did both the same group of patients while not taking warfarin (10.50/100 person years, RR 0.75, p < 0.001) and the non-warfarin group (10.69/100 person years (RR 0.74, p < 0.001).
Survival
The mean life expectancy after diagnosis of NVAF was 43.3 months. In a Kaplan-Meier analysis, patients who were treated with warfarin had a mean life expectancy of 52.0 months, whereas those who were not treated with warfarin had a corresponding life expectancy of 38.2 months (Δ = 13.8 months, p < 0.001) (fig 1). The non-warfarinised group had a high mortality in the first 12 months after AF diagnosis. Subsequent analysis (conditioned on surviving more than 12 months after AF diagnosis) showed that the increased life expectancy in the warfarinised group was maintained (p < 0.01). After age, sex, and morbidity at baseline were added to the Cox proportional hazards model, life expectancy in the warfarinised group increased slightly to 52.6 months, whereas survival in the non-warfarinised group remained at 38.2 months (Δ = 14.4 months, p < 0.001). The difference in mortality was preserved in elderly patients older than 75 years, who had an increased life expectancy of 44.7 months (with warfarin) and 32.5 months (without warfarin; Δ = 12.2 months, p < 0.001).

Kaplan-Meier survival analysis of patients with non-valvar atrial fibrillation when treated and untreated with warfarin.
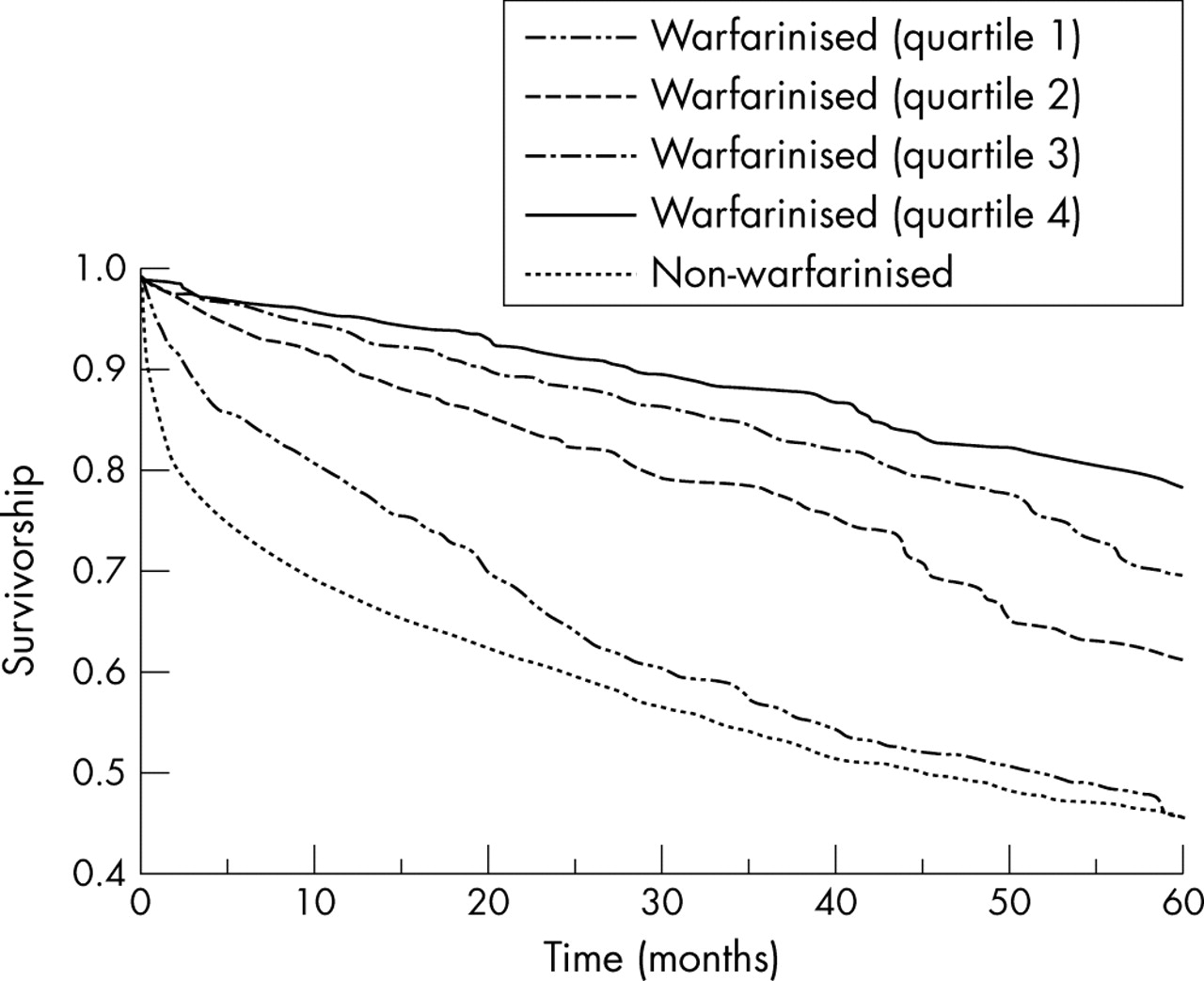
After dividing patients who received warfarin into quartiles based on their degree of anticoagulation control (percentage of time in target range), a difference in life expectancy was observed. Those in the upper quartile of control (best control), as defined above, had a mean life expectancy of 57.5 months (Δ = 19.3 months v non-warfarin treated patients, p < 0.001), whereas those in the lowest quartile of control (worst control) had a mean life expectancy of 38.1 months (Δ = −0.1 months v non-warfarinised patients, not significant) (fig 2). The difference in life expectancy between the upper and lower quartile of control was 19.4 months (p < 0.001).
{kind=link}
{kind=link}
Cox proportional hazards model analysis of survival of patients with non-valvar atrial fibrillation by quartiles of control (proportion of international normalised ratio within target range). The average percentage time in range was 32.4% in the first quartile, 59.1% in the second, 71.6% in the third, and 83.9% in the fourth.
Sensitivity analysis
A key assumption in the analyses was that an event that occurred ⩾ 42 days after the last INR test was not occurring during warfarin treatment. The effect of changing this to ⩾ 21 days was to decrease the number of events in the warfarin treated group when they were classified as being treated with warfarin: ischaemic stroke decreased by 22 events, bleeding events by six events, and all ischaemic diagnoses by 37 events. This had the effect of decreasing the rate of stroke to 3.93/100 person years and increasing the RRs of the warfarin group when treated versus the non-warfarin group to 1.59.
DISCUSSION
This retrospective study of a large UK population compared the risk of serious thromboembolic and bleeding events and survival in patients with NVAF treated with or without warfarin. Survival was increased in patients treated with warfarin, and this was related to the proportion of time they spent within the target INR range (2.0–3.0). Warfarin treatment was found to be associated with a lower risk of ischaemic and thromboembolic events and an increase in bleeding events.
The rate of stroke was significantly lower among patients treated with warfarin than among patients who were not treated with warfarin. However, the risk reduction observed (26%) was substantially lower than in clinical trials where reductions in risk of stroke of up to two thirds have been reported.4,5,6,7,8,9,10 This suggests that in routine medical management such reductions are not achieved. The level of INR control may be an important factor in explaining this discrepancy. The rate of stroke observed in both groups is high relative to previous reports.22–24 The requirement for a hospitalisation in the selection criteria may have biased the study population towards patients with more severe NVAF and a greater risk of stroke. If patients were treated according to guidelines, it would be expected that patients at greater risk would be selected for treatment.25 It is therefore unlikely that the lower stroke rate in the warfarin group is explained by this group being at lower initial risk than the non-warfarin group. This is supported by the very similar risk of stroke and all ischaemic or embolic events seen in the untreated group and in the treated group while not receiving warfarin.
The results show that the mean survival of patients treated with warfarin was more than a year longer than that of the group who did not receive warfarin. This survival advantage was maintained after controlling for age and for morbidity status. For morbidity status, days in hospital in the year before the NVAF index event was used. This was a convenient measure but we acknowledge that it is limited, as extent of morbidity may not necessarily be measured by length of stay.
The differences in survival are apparent even in the oldest patients. These data may indicate that a failure to treat patients with warfarin is associated with decreased survival. It has previously been shown that patients whose warfarin treatment is well controlled have a lower risk of thromboembolic events, in particular stroke.17,26 In this study, the survival of patients with NVAF treated with warfarin was stratified by the quality of the INR control based on the proportion of time spent in the target INR range 2.0–3.0. In routine clinical practice the time individual patients spend in this target range varies considerably.25 Patients with well controlled INR survived on average more than a year and a half longer than patients with poor control, whose survival was indistinguishable from the non-warfarin treatment group. Although this difference in survival may be influenced by factors outside the dataset, it is consistent with previous reports that mortality is increased in warfarin treated patients with NVAF when their INR is outside the target range.15
This study confirmed previous observations that many patients with NVAF remain untreated.12 In this UK study population, only 36% of patients (27% of the elderly > 75 years) were treated with warfarin over the study period, and even these patients were treated for only 70% of the possible time from NVAF diagnosis. Several factors may have influenced this apparent undertreatment. Patients who were not treated with warfarin may have been at low risk and appropriately treated with aspirin. However, this is not consistent with the patterns observed in this study, where the proportion of patients treated with warfarin did not increase with increasing age. Only 26% of women older than 75 years, a group known to be at high risk,27 were treated with warfarin. The risk of all thromboembolic events is very similar for the non-warfarin group and the warfarin group when not treated. Reluctance by the physician or patient to accept the risk of adverse events associated with warfarin is known to contribute to undertreatment.16 The rate of hospital admission due to bleeding was lower in the warfarin group while untreated than in the non-warfarin treated group, suggesting that the non-warfarin group included patients at a higher initial risk of bleeding. This may have influenced the decision not to treat some of the patients with NVAF in this study. A physician would also be more reluctant to treat any patients who were already receiving medication that may interact with warfarin.16 The non-warfarin group was older than the warfarin group and the older patients may have been considered unable to cope with the regular INR monitoring required during warfarin treatment. Although some patients should not be treated with warfarin because of safety concerns, many patients within the untreated group probably would benefit from warfarin treatment.
The study design has some limitations. No data were available directly describing medication with warfarin and aspirin. Because of this, we assumed that only patients who had some degree of continuous monitoring (more than four INR tests) were treated with warfarin. Some of the patients with one to four tests may have discontinued treatment very early on. Further, only patients who had an inpatient diagnosis or record of NVAF were included. Patients examined in primary care and with no hospital admission relating to NVAF were excluded, and therefore the patients included in the study may be predicted to have had greater morbidity than a sample selected from both hospital and primary care. These morbidities may also include alcoholism, dementia, or other diseases that may preclude anticoagulation. There are methodological issues when attempting to estimate the proportion of time a patient is within or outside the INR target range. However, linear interpolation has also been shown to be the most valid and simplest technique compared with other methods.28 Given these limitations, these data describe the care and monitoring of a large cohort of patients, with a very large number of INR values, events, and deaths, and over a lengthy study period. Systematic biases—for example, coding inaccuracies—would be common to all comparative groups.
These data suggest that the failure to treat according to national guidelines in routine clinical practice, in terms both of patients selected for anticoagulation and of difficulty maintaining those selected patients within the recommended INR target range of 2.0–3.0, was associated with additional mortality and morbidity among patients with NVAF.
REFERENCES
Footnotes
-
Published Online First 12 May 2005
-
The study was funded by AstraZeneca (UK), which developed a product that will compete directly with warfarin for some indications including non-valvar atrial fibrillation. Their input was minimal, although they reviewed an almost finalised manuscript and made acceptable presentational changes.